Download presentation
Presentation is loading. Please wait.

1
Optimizimg Colorectal Cancer Screening and Surveillance Thomas B. Hargrave M.D March 23, 2013

2
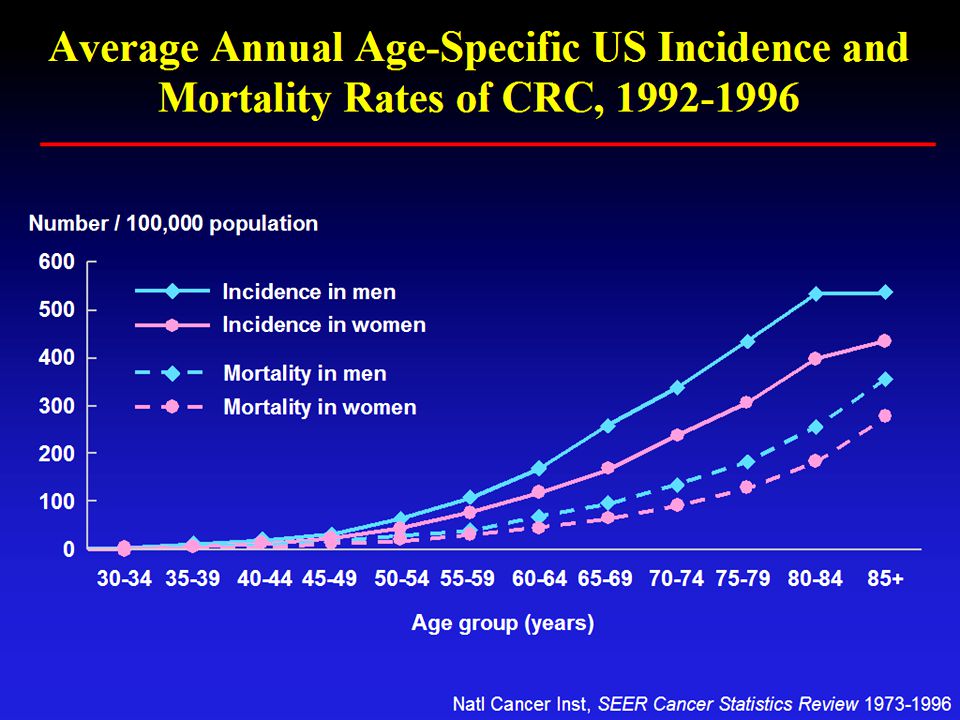
CRC: Overview In 2012, colorectal cancer (CRC) was estimated to be diagnosed in 143,460 persons and responsible for the death of 51,690 persons in the US Colorectal cancer is the third most common cancer in California, and second deadliest cancer in men and women The incidence of CRC has been declining over the last 2 decades Screening for and removal of colonic adenomas appears to significantly reduce the incidence of and risk of dying from colorectal cancer
 was estimated to be diagnosed in 143,460 persons and responsible for the death of 51,690 persons in the US Colorectal cancer is the third most common cancer in California, and second deadliest cancer in men and women The incidence of CRC has been declining over the last 2 decades Screening for and removal of colonic adenomas appears to significantly reduce the incidence of and risk of dying from colorectal cancer")
4
Colorectal Cancer Rates by Race and Ethnicity

5
Projected Annual Hospital Admissions for Colon Cancer in the US: 1990-2050 Seifeldin and Hantsch, Clin Ther 1999; 21: 1370 Year Number of admissions (thousands)
")
6
Rationale for Screening

7
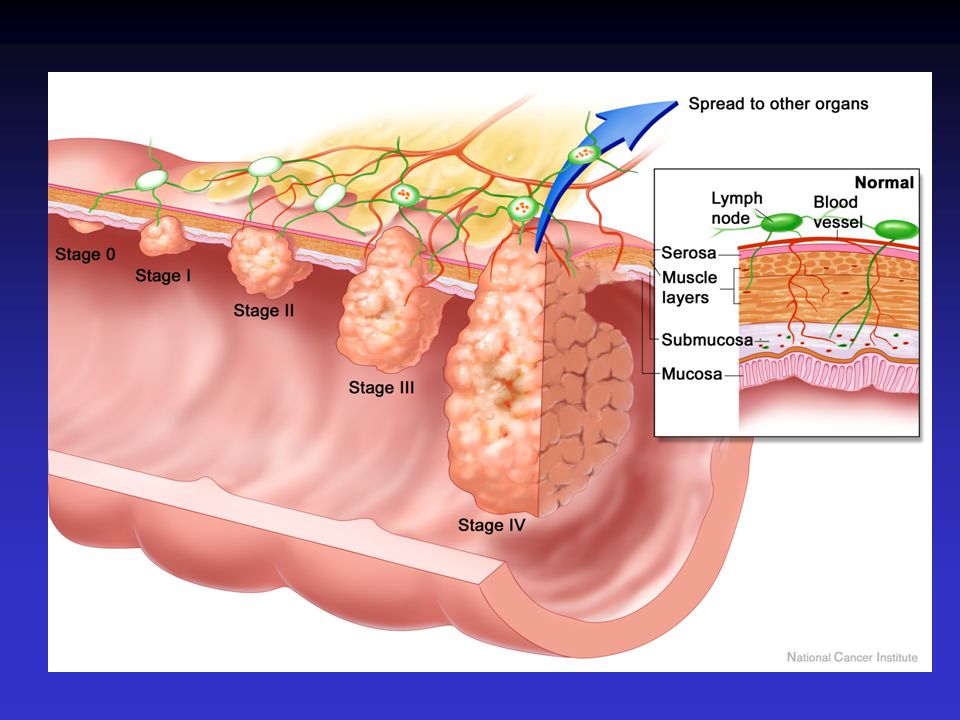
Most CRC are slow growing with a doubling time of approximately 600 days Estimated 75-80% of colon cancers develop from a polypoid adenoma (>10 years) “Polyp-Cancer Sequence” Removal of advanced adenomas (over 10 mm, or associated with villous features) reduces the incidence of invasive CRC Cancers discovered by screening tend to be less advanced and associated with greater probability of curative resection
 Polyp-Cancer Sequence Removal of advanced adenomas (over 10 mm, or associated with villous features) reduces the incidence of invasive CRC Cancers discovered by screening tend to be less advanced and associated with greater probability of curative resection")
8
Benefit of Screening: Earlier Stage = Improved Survival

10
Distribution of Cancer Stages at Time of Diagnosis: 1999-2006 American Cancer Society Facts and Figures 2012

11
Flexible Sigmoidoscopy in the Randomized Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial Of 77 447 enrollees, 67 073 (86.6%) had at least one FSG and 39 443 (50.9%) had two FSGs. Repeat FSG increased colorectal cancer or advanced adenoma detection in women by one- fourth and in men by one-third Of 223 pts who received a diagnosis of colorectal carcinoma within 1 year of a positive FSG, 64.6% had stage I and 17.5% had stage II disease ( i.e. 82% localized disease) J Natl Cancer Inst. 2012;104(4):280-289
 J Natl Cancer Inst. 2012;104(4):")
12
2012 CRC Screening and Surveillance Guidelines

13
CRC Screening Options Colonoscopy, Flexible sigmoidoscopy, CT colonography (CTC), Stool tests –Guaiac-based tests –FIT –Fecal DNA
, Stool tests –Guaiac-based tests –FIT –Fecal DNA")
14
CRC Screening Options: Average Risk In 2008 two important CRC screening guidelines were published: –American Cancer Society and the US Multi- Society Task Force with the American College of Radiology –US Preventative Services Task Force (USPSTF) The USPSTF recently updated surveillance guidelines in August 2012
 The USPSTF recently updated surveillance guidelines in August 2012")
15
CRC Screening Options: Average Risk ACS and Multi-Society Task Force Annual screening with high-sensitivity FOBT –FIT vs guaiac-based tests Sigmoidoscopy every 5 years with high sensitivity FOBT every 3 years Colonoscopy every 10 years Double contrast BE every 5 years CT colonography (CTC) every 5 years
 every 5 years")
16
CRC Screening Options: Average Risk USPSTF Annual screening with high-sensitivity FOBT –FIT vs guaiac-based tests Sigmoidoscopy every 5 years with high sensitivity FOBT every 3 years Colonoscopy every 10 years Insufficient evidence –CT colonography - ACBE –Fecal DNA

17
Family History of Colon Cancer Single first-degree relative with CRC or advanced adenoma (adenoma 1 cm in size, or with high-grade dysplasia or villous elements) diagnosed over age 60 years. –Recommended screening: same as average risk (colonoscopy every 10 years beginning at age 50 years) Single first-degree relative with CRC or advanced adenoma diagnosed at age <60 years or two first- degree relatives with CRC or advanced adenomas. –Recommended screening: colonoscopy every 5 years beginning at age 40, or 10 years younger than age at diagnosis of the youngest affected relative
 Single first-degree relative with CRC or advanced adenoma diagnosed at age <60 years or two first- degree relatives with CRC or advanced adenomas. –Recommended screening: colonoscopy every 5 years beginning at age 40, or 10 years younger than age at diagnosis of the youngest affected relative.")
18
Importance of Surveillance Colonoscopies

19
Cumulative Probabilities of CRC Based on Adenoma Histology and the Presence or Absence of Surveillance. Gut. 2012;61(8):1180-1186
:")
20
2012 Consensus Update by the USPSTF on Colorectal Cancer Surveillance Baseline colonoscopy: most advanced finding(s) Recommended surveillance interval (y) Quality of evidence supporting the recommendation New evidence stronger than 2006 No polyps10ModerateYes Small (<10 mm) hyperplastic polyps in rectum or sigmoid 10ModerateNo 1–2 small (<10 mm) tubular adenomas 5–10ModerateYes 3–10 tubular adenomas3ModerateYes >10 adenomas<3ModerateNo One or more tubular adenomas ≥10 mm 3HighYes One or more villous adenomas 3ModerateYes Adenoma with HGD3ModerateNo
 Recommended surveillance interval (y) Quality of evidence supporting the recommendation New evidence stronger than 2006 No polyps10ModerateYes Small (<10 mm) hyperplastic polyps in rectum or sigmoid 10ModerateNo 1–2 small (<10 mm) tubular adenomas 5–10ModerateYes 3–10 tubular adenomas3ModerateYes >10 adenomas<3ModerateNo One or more tubular adenomas ≥10 mm 3HighYes One or more villous adenomas 3ModerateYes Adenoma with HGD3ModerateNo")
21
2012 Consensus Update by the USPSTF on Colorectal Cancer Surveillance Baseline colonoscopy: most advanced finding(s) Recommended surveillance interval (y) Quality of evidence supporting the recommendation New evidence stronger than 2006 Sessile serrated polyp(s) <10 mm with no dysplasia 5LowNA Sessile serrated polyp(s) ≥10 mm or Sessile serrated polyp with dysplasia or Traditional serrated adenoma 3LowNA Serrated polyposis syndrome a** a 1ModerateNA ** 1) at least 5 serrated polyps proximal to sigmoid, with 2 or more ≥10 mm; (2) any serrated polyps proximal to sigmoid with family history of serrated polyposis syndrome; and (3) >20 serrated polyps of any size throughout the colon.
 Recommended surveillance interval (y) Quality of evidence supporting the recommendation New evidence stronger than 2006 Sessile serrated polyp(s) <10 mm with no dysplasia 5LowNA Sessile serrated polyp(s) ≥10 mm or Sessile serrated polyp with dysplasia or Traditional serrated adenoma 3LowNA Serrated polyposis syndrome a** a 1ModerateNA ** 1) at least 5 serrated polyps proximal to sigmoid, with 2 or more ≥10 mm; (2) any serrated polyps proximal to sigmoid with family history of serrated polyposis syndrome; and (3) >20 serrated polyps of any size throughout the colon.")
22
Sessile Serrated Polyps

23
Serrated polyps are distinct from conventional adenomas and represent a heterogeneous group of polyps with varying histology and malignant potential Certain serrated polyps may be precursors for colorectal cancers that develop via a "serrated polyp pathway“ Molecular markers suggest a link between SSPs and colorectal cancers characterized as having a CpG island methylator phenotype (CIMP) Precursors of CIMP-positive colorectal cancer, such as SSPs, have been proposed to have a particularly important role in proximal colon cancer development.
 Precursors of CIMP-positive colorectal cancer, such as SSPs, have been proposed to have a particularly important role in proximal colon cancer development.")
24
75-80%

25
Serrated Adenomas Can be Difficuly to Identify Mucous cap

26
Sessile Serrated Adenoma with Focus of HGD

27
So Which Screening Test Is Best for Average Risk Patients? “The best test is the one that gets done.” John M. Inadomi, M.D. N Engl J Med 2012

28
Adults 50-75 with Up-to-date CRC Screening 2012 Fecal occult blood test (FOBT) during the previous year, a sigmoidoscopy within the previous five years and a FOBT within the previous three years, or a colonoscopy within the previous 10 years
 during the previous year, a sigmoidoscopy within the previous five years and a FOBT within the previous three years, or a colonoscopy within the previous 10 years")
29
CRC Screening Options Colonoscopy, Flexible sigmoidoscopy, CT colonography (CTC) Stool tests –Guaiac-based tests –FIT –Fecal DNA 59% reduction in CRC mortality >90% sensitivity for adenomas > 1 cm 86% sensitivity for adenomas >6 mm
 Stool tests –Guaiac-based tests –FIT –Fecal DNA 59% reduction in CRC mortality >90% sensitivity for adenomas > 1 cm 86% sensitivity for adenomas >6 mm")
30
Screening Colonoscopy : Statistics The use of colonoscopy for screening has increased steadily over the last decade Estimates 15 million colonoscopies performed each year in US No randomized, controlled trials have tested whether colonoscopy reduces the incidence of colon cancer. Support for the role of colonoscopy in CRC prevention derives entirely from indirect evidence and observational studies Only 50% of eligible adults screened

31
Use of Colonoscopy and Flexible Sigmoidoscopy Among Medicare Fee-for-Service Beneficiaries JAMA. 2006;296:2815-2822. Procedures per 100 000 beneficiaries from a piecewise linear regression model.

32
Which CRC Screening Approach is Most Cost- Effective?

33
Markov Model: Estimated Reductions in CRC Deaths for Various Screening Protocols Gastroenterology 2005;129:1151-62

34
Estimated Cost Per Life-Year Gained Compared With Natural History Gastroenterology 2005;129:1151-62 This is the Kaiser rationale for the use of annual FIT over colonoscopy

35
Colonoscopic Polypectomy is the Therapeutic “Tip of the Spear” of CRC Prevention Colonoscopy Positive F.I.T Positive FOBT Positive FS Family HistoryVirtual CTCDC Ba Enema Surveillance

36
Colonoscopic Screening: How Well Does It Actually Work?

37
Screening Colonoscopy Efficacy Although the National Polyp Study suggested that colonoscopic polypectomy reduced subsequent cancer risk by 70-90%, real-world studies indicate significantly less efficacy Population studies from Germany and Canada have reported reductions of as low as only 30% to 50%. The ability of colonoscopy to reduce proximal colon cancer appears significantly less than in distal cancers

38
Retrospective Analysis from the National Polyp Study (NPS): Removal of Adenomatous Polyps Associated with a 53% Reduction in CRC Mortality: Mean Follow-up of 15.8 years. Zauber AG et al. N Engl J Med 2012;366:687-696 53% mortality reduction

39
65% CRC Reduction May Be Best We Can Practically Achieve 715 patients with screening and surveillance colonoscopies 1989-2003 (Univ. Indiana) 10,492 patient-years of follow-up –Doctors, dentists, nurses and spouses –95% White 12 cases of colon cancer/ 3 cancer deaths at average of 8 years of follow-up –8/12 (66%) cancers in proximal colon. 67% reduction in cancer incidence 65% reduction in cancer death Clin Gastro Hep 2009;7;770-775
 10,492 patient-years of follow-up –Doctors, dentists, nurses and spouses –95% White 12 cases of colon cancer/ 3 cancer deaths at average of 8 years of follow-up –8/12 (66%) cancers in proximal colon. 67% reduction in cancer incidence 65% reduction in cancer death Clin Gastro Hep 2009;7;")
40
Colonoscopy: Marginally Effective Against Proximal Cancers

41
CRC Mortality Reduction with Colonoscopy: Proximal vs. Distal StudyOR: Distal CancersOR: Proximal Cancers Canada 2009 (1)0.330.99 Germany 2010 (2)0.290.99 California 2004 (3)0.160.67 Germany 2011 (4)0.160.44 Canada 2010 (5)0.530.94 Netherlands (2010) (6)0.360.98 USA 2012 (7)0.240.58 1)Annals Int Medicine 2009;150:1-82 2) J. of the National Cancer Institute 2010; 102: 89 – 95 3) Gastroenterology 2004;127:452–456. 4 ) Ann Intern Med. 2011:154;22-30 5) Gastroenterology. 2010;139:1128–1137 6) Eur J Gastroenterol Hepatol. 2010;22:437–443 ) 7) J Clin Oncol. 2012;30:2664–2669
 Germany 2010 (2) California 2004 (3) Germany 2011 (4) Canada 2010 (5) Netherlands (2010) (6) USA 2012 (7) )Annals Int Medicine 2009;150:1-82 2) J. of the National Cancer Institute 2010; 102: 89 – 95 3) Gastroenterology 2004;127:452– ) Ann Intern Med. 2011:154; ) Gastroenterology. 2010;139:1128–1137 6) Eur J Gastroenterol Hepatol. 2010;22:437–443 ) 7) J Clin Oncol. 2012;30:2664–2669.")
42
Why Does Colonoscopy Fail to Reduce Proximal CRC?

43
Possible Reasons for Why Colonoscopy Protection is Imperfect Operator- dependent factors –Missed lesions during the initial colonoscopy, –Incomplete adenoma removal, –Failed detection of cancer despite biopsy. –Poor bowel preparation Tumor biology (sessile serrated adenomas, micro- satellite instability )
.")
44
Possible Reasons for Why Colonoscopy Protection is Imperfect Physician: Procedural/motor skill deficits –Perceptual factors (e.g., variation in color and depth perception) –Personality characteristics (e.g., conscientiousness, obsessiveness, impulsivity) –Knowledge and attitude deficits (e.g., awareness and appearance of flat lesions) –Incomplete colonoscopy –Withdrawal technique
 –Personality characteristics (e.g., conscientiousness, obsessiveness, impulsivity) –Knowledge and attitude deficits (e.g., awareness and appearance of flat lesions) –Incomplete colonoscopy –Withdrawal technique")
45
Colonoscopy May Not Reduce the Incidence of Sessile Serrated Polyps Group Health-based study population included 213 advanced adenoma cases, 172 SSP cases, and 1,704 controls aged 50–79 years, who received an index colonoscopy from 1998–2007 Previous colonoscopy was inversely associated with advanced adenomas in both the rectum/distal colon (OR=0.38; 95% CI: 0.26–0.56) and proximal colon (OR=0.31; 95% CI: 0.19–0.52), but There was no statistically significant association between previous colonoscopy and the incidence of SSPs Am J Gastroenterol. 2012;107(8):1213-1219
:")
46
Logistic Regression Analyses of the Assoc. Between Previous Colonoscopy, Advanced Adenomas (AA), and Sessile Serrated Polyps (SSP) Am J Gastroenterol. 2012;107(8):1213-1219
, and Sessile Serrated Polyps (SSP) Am J Gastroenterol. 2012;107(8):")
47
Adenoma Detection Rate Predicts Future Cancer Reduction

48
Adenoma Detection Rate and Subsequent Cancer Risk Multivariate Cox proportional-hazards regression model to evaluate the influence of quality indicators for colonoscopy on the risk of interval cancer. Data were collected from 186 endoscopists who were involved in a colonoscopy-based colorectal-cancer screening program involving 45,026 subjects A total of 42 interval colorectal cancers were identified during a period of 188,788 person-years. The endoscopist's rate of detection of adenomas was significantly associated with the risk of interval colorectal cancer (P=0.008) Kaminski MF et al. N Engl J Med 2010;362:1795-1803.
 Kaminski MF et al. N Engl J Med 2010;362:")
49
Kaminski M et al. N Engl J Med 2010;362:1795-1803 Cumulative Hazard Rates for Interval Colorectal Cancer, According to the Endoscopist's Adenoma Detection Rate (ADR)
.")
50
Wide Variation in Adenoma Detection Rates Between Gastroenterologists Consecutive colonoscopy reports performed by nine attending gastroenterologists at Indiana University Hospital between January 1999 and January 2004 Among patients 50 yr of age, the range of detection of at least one adenoma per colonoscopy by nine colonoscopists was 15.5–41.1%, –At least two adenomas was 4.9–20.0%, –At least three adenomas was 0.8–10.8%, and –At least one adenoma 1.0 cm was 1.7–6.2%, and The range of average adenomas detected per colonoscopy was 0.21–0.86. (p<0.001) American Journal of Gastroenterology (2007) 102, 856–861
 American Journal of Gastroenterology (2007) 102, 856–861.")
51
Variation in Adenoma Detection Rates Between Gastroenterologists 550 consecutive screening colonoscopies, average risk individuals 10 BC GI at a tertiary academic institution 121 (22%) had at least one adenoma Adenoma detection rate per colonoscopy 0.09- 0.82 (a nine-fold range) Mean withdrawal time 7 min (3.4-9.6) Significant inverse relationship between cecal intubation time, withdrawal time, and adenoma detection (p<0.01) GIE 2008:67(5):AB294
 had at least one adenoma Adenoma detection rate per colonoscopy (a nine-fold range) Mean withdrawal time 7 min ( ) Significant inverse relationship between cecal intubation time, withdrawal time, and adenoma detection (p<0.01) GIE 2008:67(5):AB294")
53
Missed Adenomas Tandem colonoscopy studies have demonstrated adenoma miss rates of 21% to 24% Some investigators have suggested that the true miss rate could be even higher because the same technology was used twice, and lesions behind folds or flexures could be missed during both procedures. Pickhardt et. al. mapped locations of adenomas missed by colonoscopy but detected by CT colonography and found that 67% were on the proximal aspect of folds.** ** Location of adenomas missed by optical colonoscopy. Ann Intern Med. 2004;141:352–359

54
True vs. “Community” Prevalence of Adenomas and ADRs True prevalence of adenomas ADR range in published studies Mean published ADR for males Mean published ADR for females Target ADR males Target ADR females % of screened patients with adenomas >50%10-60%32%20%25%15%

55
Incomplete Polypectomy

56
Pohl et al performed biopsies on the margins of 346 polypectomy sites after apparently complete resection. The incomplete resection rate as evidenced by residual microscopic neoplastic tissue was 10.1% and ranged from 6.5% to 22.7% among different endoscopists. Larger polyp size and sessile serrated polyp histology were predictors of incomplete resection. Incomplete polyp resection during colonoscopy−results of the Complete Adenoma Resection (CARE) Study. Gastroenterology. 2013;144:74 e1–80 e1
 Study. Gastroenterology. 2013;144:74 e1–80 e1.")
57
Rates of Incompletely Resected Polyps Gastroenterology Volume 144, Issue 1, Pages 74-80.e1, January 2013Volume 144, Issue 1 Incomplete polyp resection during colonoscopy−results of the Complete Adenoma Resection (CARE) Study. Gastroenterology. 2013;144:74 e1–80 e1

58
Gastroenterology Volume 144, Issue 1, Pages 74-80.e1, January 2013Volume 144, Issue 1 Rates of Incompletely Resected Polyps Incomplete polyp resection during colonoscopy−results of the Complete Adenoma Resection (CARE) Study. Gastroenterology. 2013;144:74 e1–80 e1

59
Interval Colon Cancers Interval Cancers: CRC diagnosed within 6-36 months of a baseline examination negative for neoplasia ( i.e. presumed missed on colonoscopy) –Up to 9% of CRC in a Canadian registry were interval cancers –SEER medicare database 1994-2005: 7.2% of CRC were interval cancers Estimated that more than 70% of interval cancers are attributed to missed lesions with incomplete polypectomy accounting for another 10-27%, i.e. OPERATOR-DEPENDENT factors Gastroenterology 2011;140:65–72 Annals Gastro 2012 25:1-3
 –Up to 9% of CRC in a Canadian registry were interval cancers –SEER medicare database : 7.2% of CRC were interval cancers Estimated that more than 70% of interval cancers are attributed to missed lesions with incomplete polypectomy accounting for another 10-27%, i.e. OPERATOR-DEPENDENT factors Gastroenterology 2011;140:65–72 Annals Gastro :1-3.")
61
95% Blameless

62
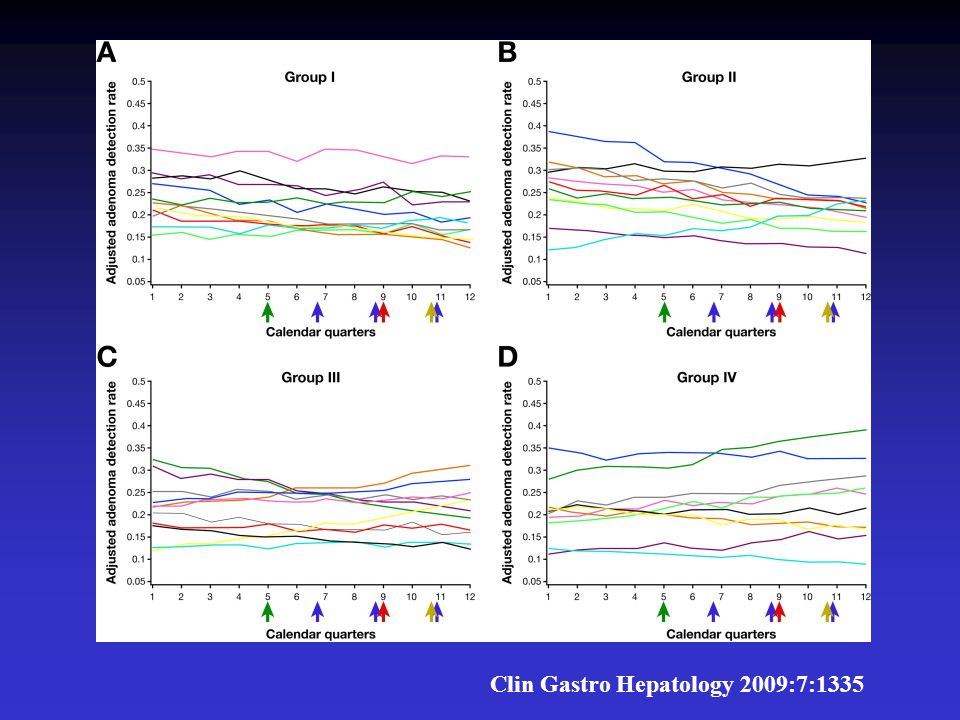
During a period of 3 years, a total of 97,623 colonoscopy examinations were performed in the 5 AECs by 51 gastroenterologists, of which 47,253 were screening examinations. Adenoma detection rates for individual physicians varied from 10%–39% Mean ADR 22% During a period of 3 years, 5 specific interventions were implemented; each was designed to improve adenoma detection rate ADR did not change in response to 5 separate educational and feedback interventions Can Poor ADA Detection be Improved with Interventions? Clin Gastro Hepatology 2009:7:1335

63
Instituting a longer withdrawal time policy or measuring withdrawal time Providing periodic feedback on withdrawal times, polyp detection rates, and patient satisfaction scores Combining longer withdrawal times with monitoring and feedback Implementation of a multifaceted program that included training, a repeat attempt at cecal intubation, and education on inspection techniques or Education and feedback on withdrawal times combined with a financial penalty. Can Poor ADA Detection be Improved with Interventions? Clin Gastro Hepatology 2009:7:1335

65
Can Poor ADA Detection be Improved with Interventions? Meta-analysis Systematic review of 15 intervention studies (2008-2011) –Total withdrawal time alone –Total withdrawal time plus confidential feedback –Segmental withdrawal time plus enhanced inspection techniques –Multiple intervention ADR range 12.7%-62% Only study one reported a demonstrable improvement in adenoma detection rate. –In that study, longer withdrawal time through use of an audible timer paired with training on enhanced inspection techniques was associated with a nearly 50% increase in adenoma detection rates among 12 examiners Gastrointestinal Endoscopy 2011; 74(3):656
 –Total withdrawal time alone –Total withdrawal time plus confidential feedback –Segmental withdrawal time plus enhanced inspection techniques –Multiple intervention ADR range 12.7%-62% Only study one reported a demonstrable improvement in adenoma detection rate. –In that study, longer withdrawal time through use of an audible timer paired with training on enhanced inspection techniques was associated with a nearly 50% increase in adenoma detection rates among 12 examiners Gastrointestinal Endoscopy 2011; 74(3):656.")
66
Videorecording of Colonoscopy Associated with Significant Increase in ADR October 2012 American College Gastroenterology Presentation

67
Videorecording of Colonoscopy Associated with Significant Increase in ADR Prospective study of 6 gastroenterologists 208 baseline exams 213 videorecorded exams Overall ADR went from 33.7% to 38.5% Individual doctors: –5/6 showed improvement –GI with second lowest ADR : 22.6% 57.7% Madhoun et al. GIE (in press)
.")
68
Can We Improve the Efficacy of Colonoscopy?

69
New Technologies to Improve Adenoma Detection Rate High-resolution colonoscopy, Chromo-endoscopy, Wide-angle colonoscopy Narrow-band imaging, Third Eye Retroscope Cap-assisted Colonoscopy Most of these techniques are associated with increased procedure duration, higher cost, reduced patient acceptance, and no clear benefit over high-quality standard colonoscopy

70
Reduce Incomplete Colonoscopies

71
Incomplete Colonoscopy A large community-based study showed that up to 13% of colonoscopies failed to reach the cecum, One common cause: a severely angulated or fixed sigmoid colon, which is often associated with sigmoid diverticular disease and/or previous pelvic surgery. –An angulated sigmoid colon can usually be overcome by the use of a thin instrument, such as a pediatric colonoscope, gastroscope, or enteroscope. A second major cause of technical difficulty is a markedly redundant colon. Poor bowel prep is also associated with lower cecal intubation

72
Water Immersion Numerous studies have evaluated the use of water immersion that warm-water immersion can speed insertion through the whole or left side of the colon and reduce pain and discomfort. In water immersion, the colon is filled with water rather than gas during the insertion phase. With the patient in the left lateral decubitus position, the sigmoid colon sinks into the left lower quadrant and remains shorter and less distended with fewer angulations compared with insertion with gas insufflation.

73
Water Immersion Simplifies Cecal Intubation in Pts with Redundant Colons and Previous Incomplete Colonoscopies 345 consecutive patients referred to a tertiary center for the indication of a previous incomplete colonoscopy Cecal intubation was achieved in 332 of 345 patients (96.2%) An external straightening device was used in 6 of 178 cases with water immersion (3.4%) compared with 25 of 168 cases with air insufflation (15%) (P <.0001). Gastrointestinal Endoscopy Volume 76, Issue 4, Pages 812-817, October 2012Volume 76, Issue 4

74
Improve Bowel Preparation

75
Poor Bowel Prep and ADR Washington University study of patients who had prior colonoscopy with inadequate prep Inadequate bowel preparation was reported on 373 patients, with an initial adenoma detection rate of 25.7% Of 133 patients who underwent repeat colonoscopy, 33.8% had at least 1 adenoma detected, and 18.0% had high-risk states detected –Per-adenoma miss rate was 47.9%. The majority of adenomas (64.8%) were missed in the proximal colon. 80% of advanced adenomas (defined as adenomas ≥1 cm or with villous components or high-grade dysplasia) also were missed in the proximal colon Gastrointestinal endoscopy 2012;75: 1197
 were missed in the proximal colon. 80% of advanced adenomas (defined as adenomas ≥1 cm or with villous components or high-grade dysplasia) also were missed in the proximal colon Gastrointestinal endoscopy 2012;75:")
76
Bowel Prep and ADR Retrospective study of 12,872 colonoscopies. Preparation quality was suboptimal (poor or fair) in 3047 patients (24%). Among these 3047 patients, repeat examination was performed in <3 years in 505 (17%) Among 216 repeat colonoscopies with optimal preparation, 83 adenoma were seen only on the second examination, an adenoma miss rate of 42% (95% CI, 35-49). The advanced adenoma miss rate was 27% For colonoscopies repeated in <1 year, the adenoma and advanced adenoma miss rates were 35% and 36%, respectively. Gastrointestinal EndoscopyVolume 73, Issue 6 :1207-1214, June 2011
 in 3047 patients (24%). Among these 3047 patients, repeat examination was performed in <3 years in 505 (17%) Among 216 repeat colonoscopies with optimal preparation, 83 adenoma were seen only on the second examination, an adenoma miss rate of 42% (95% CI, 35-49). The advanced adenoma miss rate was 27% For colonoscopies repeated in <1 year, the adenoma and advanced adenoma miss rates were 35% and 36%, respectively. Gastrointestinal EndoscopyVolume 73, Issue 6 : , June")
77
Conventional PM only Dosing versus PM/AM Split-dosed Bowel Preparations.

78
randomized study of split-dosage versus non-split dosage regimens of high-volume versus low- volume polyethylene glycol solutions Randomized Study of Split-dosage vs Non- split Dosage Regimens of PEG Solutions

79
Failed intubation to the cecum was recorded in 41 of 354 patients (11.7%) with fair/poor bowel cleansing and in 6 of 513 patients (1.2%) with good/excellent bowel cleansing (P =.00001). Aborted procedures were significantly more frequent in patients randomized to the non-split-dosage group (91/430 [21.2%] vs 30/432 [6.9%] of the split-dosage group, P <.0001). Polyp detection rate was significantly higher in patients with bowel cleansing rated as fair/good (57/209, 27.3%) or good/excellent (126/512, 24.6%) compared with those with bowel cleansing rated as poor/fair (18/147, 12.2%) (P =.001). Gastrointestinal Endoscopy 2012;72:313
. Polyp detection rate was significantly higher in patients with bowel cleansing rated as fair/good (57/209, 27.3%) or good/excellent (126/512, 24.6%) compared with those with bowel cleansing rated as poor/fair (18/147, 12.2%) (P =.001). Gastrointestinal Endoscopy 2012;72:313.")
80
Pt. Education with Cartoons Effectively Improved Bowel Prep for Colonoscopy Gastrointestinal Endoscopy Volume 76, Issue 4, Pages 804-811, October 2012Volume 76, Issue 4

81
Quality Measures for Colonoscopy Cecal intubation rate goal = >95% –Photocumentation ADR : bare minimum acceptable –Males 25% Females 15% –Reasonable ADR: Males 30-35% Females 20-25% Technique –Cecal retroflexion –Water immersion for difficult sigmoid –Minimal withdrawal time = as long as it takes –Perform your own tandem examination Pretend the exam is being videotaped

82
Optimization of Colonoscopic Examination Optimize bowel prep –Split dose if possible –Colonoscopy within 6-8 hours of last dose Compliance with recommeded post- polypectomy surveillance guidelines Tract adverse events –Perforation: <1/4000 diagnostic <1/2000 therapeutic –Post polypectomy bleeding

84
Third Eye Retroscope Catheter Cost: $375/case Processor $20,000

85
Is Cecal Retroflexion Effective? Prospective study of 1000 patients undergoing colonoscopy ( non-controlled, 2 endoscopists) Pproximal colon retroflexion was achievable in approximately 95% of routine colonoscopies, Iit was safe, and it identified additional polyps (including additional flat lesions) in 5.8% of patients. Finding additional polyps on retroflexion was associated with older age, male sex, and the detection of polyps in the forward view. Of those with no polyp detected in the forward view, 2.2% had an adenoma detected on retroflexion. Gastrointestinal Endoscopy 2011;Volume 74, Issue 2 : 246-252,
 Pproximal colon retroflexion was achievable in approximately 95% of routine colonoscopies, Iit was safe, and it identified additional polyps (including additional flat lesions) in 5.8% of patients. Finding additional polyps on retroflexion was associated with older age, male sex, and the detection of polyps in the forward view. Of those with no polyp detected in the forward view, 2.2% had an adenoma detected on retroflexion. Gastrointestinal Endoscopy 2011;Volume 74, Issue 2 : ,.")
86
Cap Assisted Colonoscopy

87
Cap-Assisted Colonoscopy Attaching a small transparent cap to the tip of the colonoscope can help depress haustral folds, thereby decreasing the blind mucosal surface area and may improve adenoma detection rates. In some studies, this approach has been reported to be associated with improved polyp detection, reduced cecal intubation time, and enhanced cecal intubation rate Meta-analysis of 16 randomized controlled clinical trials were included consisting of 8,991 subjects (CAC: 4,501; SC: 4,490) CAC demonstrated marginal benefit over SC for polyp detection and shortened the cecal intubation time. Am J Gastroenterol. 2012;107(8):1165-1173
 CAC demonstrated marginal benefit over SC for polyp detection and shortened the cecal intubation time. Am J Gastroenterol. 2012;107(8):")
Similar presentations



















:1179-1187 September 17, 2009.>")
