Download presentation
Presentation is loading. Please wait.

1
Pelvic Inflammatory Disease (PID) Natasha Lomax Tamika Missouri Monique Veney
 Natasha Lomax Tamika Missouri Monique Veney")
3
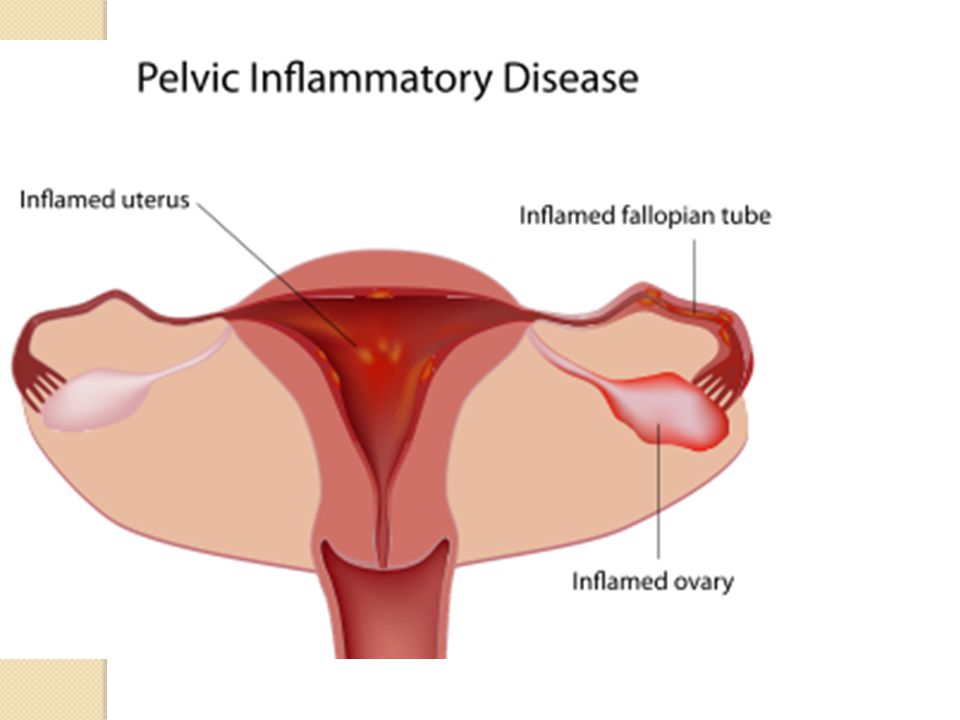
Definition Pelvic inflammatory disease is an infection of a woman’s reproductive organs It’s an inflammatory disorder that affects a female’s upper genital tract.

4
Epidemiology Women can get PID if untreated bacteria moves up from the vagina and infects the pelvic organs. Different organisms can cause PID but the most common are caused by organisms of two STIs (chlamydia and gonorrhea). PID affects ~ 1 million women annually with 85% coming from STIs. African American Women under the age of 25 are most infected.
. PID affects ~ 1 million women annually with 85% coming from STIs. African American Women under the age of 25 are most infected..")
5
Risk Factors Not Associated With STIs Multiple sex partners Douching Sexually active at a young age Prior History of PID infections History of IUD insertion in the past 3-4 weeks where the cervical mucosa is broken.

6
Symptoms Abdominal Pain Abnormal Vaginal Discharge Bleeding After Sex Bleeding Between Periods UTIs Symptoms Fever Nausea/Vomiting Cervical Motion Tenderness Uterine Tenderness Adnexal Tenderness Guarding or Rebound Tenderness LQ Pain Temperature > 101F Purulent Cervical/Vaginal Discharge Subjective Objective

7
Diagnostic Test Vaginal exam that includes cervical cultures and wet mount. Pregnancy Test Labs- CBC, CRP, Erythrocyte Sedimentation Rate(ESR) ***CRP and ESR will be elevated if the inflammatory process is taking place*** Urinalysis Pelvic Ultrasound
 ***CRP and ESR will be elevated if the inflammatory process is taking place*** Urinalysis Pelvic Ultrasound.")
8
Differential Diagnoses Acute Appendicitis Ectopic Pregnancy Ovarian Torsion UTI/ Pyelonephritis Other Vaginal Infections Salpingitis, Endometritis, Ovarian Cysts or Masses

9
Treatment Outpatient- CDC (2010) Recommended Regimen Ceftriaxone 250 mg IM in a single dose Doxycycline 100 mg WITH or WITHOUT Metronidazole 500 mg orally twice a day for 14 days Other parenteral third-generation cephalosporin (e.g., ceftizoxime or cefotaxime) Patients who do not respond to oral therapy within 72 hours should be reevaluated to confirm the diagnosis and should be administered parenteral therapy.
 Recommended Regimen Ceftriaxone 250 mg IM in a single dose Doxycycline 100 mg WITH or WITHOUT Metronidazole 500 mg orally twice a day for 14 days Other parenteral third-generation cephalosporin (e.g., ceftizoxime or cefotaxime) Patients who do not respond to oral therapy within 72 hours should be reevaluated to confirm the diagnosis and should be administered parenteral therapy.")
10
Treatment Inpatient- CDC (2010) Recommended Regimen Cefotetan 2 g IV every 12 hours Cefoxitin 2 g IV every 6 hours Doxycycline 100 mg orally or IV every 12 hours
 Recommended Regimen Cefotetan 2 g IV every 12 hours Cefoxitin 2 g IV every 6 hours Doxycycline 100 mg orally or IV every 12 hours")
11
Education Importance of follow-up in 48-72 hours and then again in 10-14 days Test to cure (3-6 months) if STI was present Safe sexual practices Medications side effects Importance of finishing antibiotic regimen and avoiding intercourse until complete Evaluation and treatment of partner
 if STI was present Safe sexual practices Medications side effects Importance of finishing antibiotic regimen and avoiding intercourse until complete Evaluation and treatment of partner")
Similar presentations


>")





 as PID is an infection that affects a woman’s reproductive.>")
>")

 Study.>")


>")




