Download presentation
Presentation is loading. Please wait.

1
Urinary Incontinence - Assessment
Bronwyn Peck Continence Nurse Advisor Grampians Regional Continence Service Ballarat Health Services – Queen Elizabeth Centre

2
Incontinence is…… Loss of control of the bladder or bowel that is involuntary and socially unacceptable A symptom ….. not a disease Grampians Regional Continence Service - Ballarat Health Services

3
The extent of the problem
Common….. Affects 4.2 million Australians aged over 15 living in the community This is equivalent to 26% of the population This is predicted to rise to 5.6 million by 2030 Affects up to 37% of women Affects up to 13% of men Around 71% in residential care 70% of people affected do not seek advice Grampians Regional Continence Service - Ballarat Health Services

4
The extent of the problem
Enormous financial burden In 2010 in Australia total financial cost of incontinence was estimated to be $42.9 billion This equates to $9,014 per person with incontinence Productivity losses of those with incontinence estimated to be $34.1 billion in 2010 due to lower than average employment rates Productivity losses of family and friends who care for people with incontinence on an unpaid basis $2.7 billion Grampians Regional Continence Service - Ballarat Health Services

5
Social Costs Loss of independence
Reduced social activity and isolation Decline in self care and physical health Feelings on fear, embarrassment, shame, depression, anger and stress Loss of self esteem, dignity and confidence Increased burden

6
Who is prone to incontinence?
Something that affects all ages But those at particular risk include: Children Pregnant women Women at menopause The elderly Those in hospital or other institutions Those with disabilities Sufferers of particular medical conditions People who strain at stool Grampians Regional Continence Service - Ballarat Health Services

7
Age related changes Altered urine production Hormonal changes
Decrease in strength of pelvic floor muscles Prostatic hypertrophy Changes in the cortical micturition centre Neurological changes Mobility and dexterity Medical conditions Medications

8
Grampians Regional Continence Service - Ballarat Health Services

9
The myths about incontinence
A normal part of ageing Expected with childbearing There is nothing that can be done “I am the only one” Children will grow out of bedwetting It is not a serious problem Grampians Regional Continence Service - Ballarat Health Services

10
Attitudes and incontinence
Present a major problem in tackling this condition Attitudes of sufferers and their families Health professionals and carers The general public and the media Grampians Regional Continence Service – Ballarat Health Services

11
Continence is complex….
To be continent you need to be able to: Be aware of an urge to void/pass urine Know what to do and where to go Be able to get there & manage clothing Store urine in bladder till right time Empty bladder on cue Manage wiping/drying/clothing Grampians Regional Continence Service - Ballarat Health Services

12
Grampians Regional Continence Service - Ballarat Health Services

13
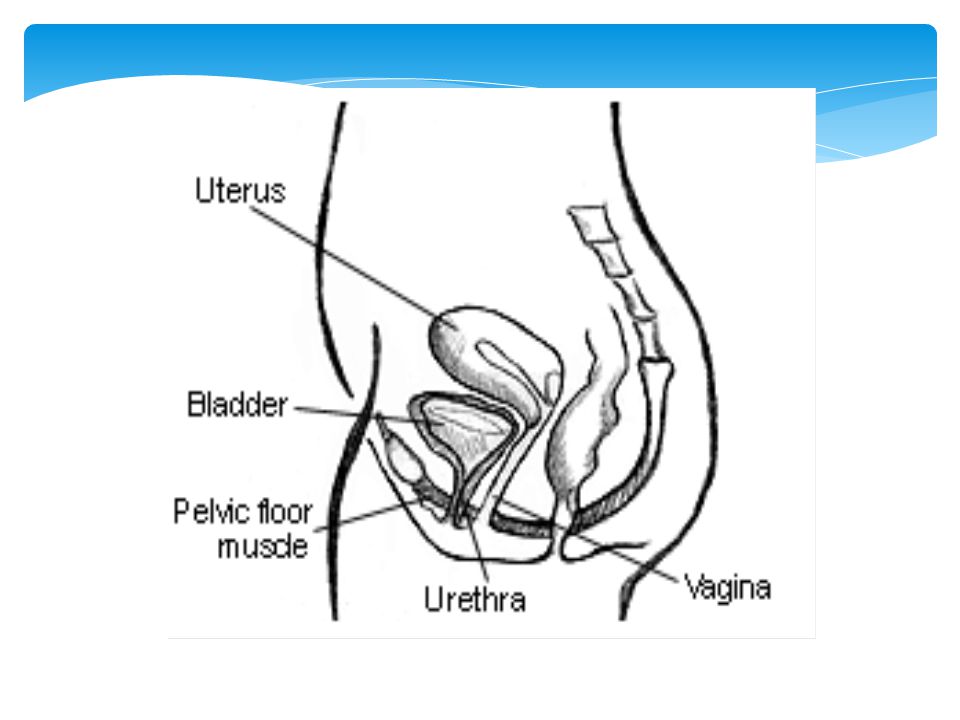
Not just about the bladder
We need Intact central nervous system Intact peripheral nervous system Adequate mobility & dexterity Adequate cognition Bladder that is able to store and empty Intact & functioning urinary sphincters An environment that supports continence Grampians Regional Continence Service - Ballarat Health Services

14
Grampians Regional Continence Service - Ballarat Health Services

15
Normal Bladder Function
Dryness at all times Voiding 4-6 times per day & not more than once at night Passing mls of urine per void Ability to defer as long as required to get to toilet Passing a continuous stream of urine without burning or pain Sense of incomplete emptying once finished Grampians Regional Continence Service - Ballarat Health Services

18
Continence Assessment
Assessment of incontinence is a necessary preliminary step in planning appropriate intervention and management of presenting problems. As there are different types and causes of incontinence which impact on people differently, an individual approach is essential.

19
There are different types of urinary incontinence therefore:
Need to identify the cause of the symptoms The different types of incontinence require different treatments Need to collect information so the correct type of management can be put into place Grampians Regional Continence Service - Ballarat Health Services

20
When do you do a continence assessment?
When the person has been observed to have a continence problem When a continence problem has changed When current management is no longer effective and requires evaluation.

21
Who should be involved? Person Family/carers Nursing team Local doctor
Allied health workers, eg. OT, PT, dietician Community service personnel

22
What basic information do we need to collect?
Bladder symptoms: History of the condition Onset & duration Person’s perception of the problem Bowel status Dietary & fluid intake Aids & appliances used and effectiveness Grampians Regional Continence Service - Ballarat Health Services

23
For a complete assessment we need to collect…
Social history Medical & surgical history Obstetric/gynaecological Urological – including previous investigations Medications Functional status Cognitive, mobility, dexterity, ADL’s Environmental factors Grampians Regional Continence Service - Ballarat Health Services

24
What is included in a continence assessment?
Subjective data What the person tells you about the problem Objective data What is observable about the problem

25
What is included in a continence assessment?
Objective data Medical history from medical records Medication list Urinalysis/MSU Bladder/bowel charts Functional assessment tools MMT,CFT, Bartels X-rays/scans/ultrasounds Residual urine volumes Uroflowmetry/Urodynamics Physical Examination

26
What is included in a continence assessment?
Subjective data Person’s perception of the problem History of the condition Onset, duration Medical and surgical history Obstetric/gynaecological Urological Medications Functional Status Cognitive, mobility, dexterity, ADL’s Environmental factors

27
Effect of Medications Medication review by a doctor may be warranted
Examples of medications that could effect continence: Opiates Antidepressants Antihypertensives (blood pressure medications) Diuretics Anticholinergics (possible urinary retention)
 Diuretics. Anticholinergics (possible urinary retention)")
28
Bladder diaries/charts
Design of the chart will depend on The purpose of charting The setting The client They can be used for a number of purposes: Baseline Implementation of management Evaluation

29
Diaries/charts They are not the complete assessment, but form a part of the assessment The data needs to be interpreted and used for the management Recommendation is 3 full days of charting

30
Diaries/charts Every chart needs to provide the following basic information: Fluid intake – times and volumes of drinks Frequency/time of voiding Frequency/time of incontinent episodes Voided volumes/estimate of loss Other relevant information

31
Bladder diaries/charts
At Base line 3 x 24 hour periods Person to self initiate If not able check regularly To evaluate management Maintain current strategies Chart what is happening

32
Grampians Regional Continence Service - Ballarat Health Services

33
Using the data from the charts
We need to be able to establish: Presence of patterns Frequency of voids Number of incontinent episodes Voided volumes & intervals How can we change the current situation?

34
Grampians Regional Continence Service - Ballarat Health Services

35
Types of Urinary Incontinence
Use the information collected to determine type of incontinence: Stress Incontinence Urge Incontinence Mixed Incontinence Overflow Incontinence Reflex Incontinence Functional Incontinence Transient Incontinence

36
Grampians Regional Continence Service - Ballarat Health Services

37
Urinary Incontinence - Management
Andrea Green Continence Nurse Consultant Grampians Regional Continence Service BHS-QEC

38
Goals of Continence Management
Whilst we would like to, we can’t always achieve dryness for all The aim of continence management should be improved quality of life and social continence Social Continence when complete continence is not attainable, appropriate aids and appliances can allow for socialization with absolute discretion Whilst cure for all is ideal, our management needs to be achievable and realistic. Grampians Regional Continence Service - Ballarat Health Services

39
Stress Incontinence Not enough pressure in urethra to stop leak
Involuntary loss of a small amount of urine, when coughing, sneezing or on sudden movements with increased abdominal pressure Not enough pressure in urethra to stop leak Weakened sphincters & pelvic floor muscles Excessive intra-abdominal pressure No detrusor contraction Grampians Regional Continence Service - Ballarat Health Services

40
Stress Incontinence Causes Weakened pelvic floor muscles
Childbirth Persistent heavy lifting Obesity Straining at stool Chronic cough Fall in oestrogen levels Sphincter damage post surgery Grampians Regional Continence Service - Ballarat Health Services

41
Stress Incontinence Small amount of urine lost
Difficulty stopping urine mid-stream Leakage with cough, sneezing, laughing, lifting, standing up, position changes. Grampians Regional Continence Service - Ballarat Health Services

43
Management SUI Pelvic floor exercises Oestrogen cream/pessary
Identify muscles to be exercised Do not over tire muscle Brochure, dvd Check technique Prescribed sets to monitor progress and compliance Oestrogen cream/pessary ? Alter type of anti-hypertensive Brace pelvic floor to lift, before coughing etc Grampians Regional Continence Service - Ballarat Health Services

44
Pelvic floor muscle exercises
We want to close off the bladder neck so we stay “high and dry” Technique… How often? 25% of women will bulge downward instead of lifting up Lets do some now… Grampians Regional Continence Service - Ballarat Health Services

45
Urge Incontinence Involuntary loss of urine, associated with a strong desire to void Complete bladder emptying – often a large volume Usually as the result of an involuntary contraction of the detrusor muscle Over active bladder Grampians Regional Continence Service - Ballarat Health Services

46
Grampians Regional Continence Service - Ballarat Health Services

47
Urge Incontinence Cystitis/Calculi/Tumours Urinary tract infection
Constipation Caffeine/food additives Medications (anti-cholinergics) Anxiety Neurological causes CVA M.S Parkinson’s Disease Grampians Regional Continence Service - Ballarat Health Services
 Anxiety. Neurological causes. CVA. M.S. Parkinson’s Disease. Grampians Regional Continence Service - Ballarat Health Services.")
48
Urge Incontinence Inability to defer Urgency Frequency
Decreased bladder capacity or large volumes Nocturia 2 or more Nocturnal enuresis Grampians Regional Continence Service - Ballarat Health Services

49
Management of UUI Treat UTI Alleviate constipation
Review type and amount of fluid intake Bladder retraining – deferment, don’t void “just in case” Urge suppression strategies – high and dry Toileting times (sometimes) Oestrogen replacement Medications Grampians Regional Continence Service - Ballarat Health Services
 Oestrogen replacement. Medications. Grampians Regional Continence Service - Ballarat Health Services.")
50
Overflow Incontinence
Inability to pass urine – so builds up and overflows Blockage of bladder outlet/ obstruction Enlarged prostate, strictures, sphincters not relaxing on cue Faecal impaction Bladder muscle not contracting sufficiently e.g. Diabetes, some spinal injuries, MS Epidural anaesthetics Grampians Regional Continence Service - Ballarat Health Services

51
Overflow incontinence
Persistent leakage or dribbling Post micturition dribbling Hesitancy Poor or interrupted stream Feeling of incomplete emptying Frequency, small voided volumes Nocturia X 2 UTI Distended abdomen (may be painless) Confirmed via bladder scanner Grampians Regional Continence Service - Ballarat Health Services
 Confirmed via bladder scanner. Grampians Regional Continence Service - Ballarat Health Services.")
52
Management of Overflow Incontinence
Alleviate constipation Treat UTI Double void Toileting position Catheterise (long term/short term) types of catheters/flip-flow valve /suprapubic cleaning and care instructions Grampians Regional Continence Service - Ballarat Health Services
 types of catheters/flip-flow valve /suprapubic. cleaning and care instructions. Grampians Regional Continence Service - Ballarat Health Services.")
53
Management of Overflow Incontinence
ISC - Intermittent Self Catheterisation dexterity, eye sight, sensation, mobility education of ISC/teaching techniques Product supply Minipress Surgery Grampians Regional Continence Service - Ballarat Health Services

54
Functional Incontinence
Sensation to void is present but unable to reach the toilet in time (due to barriers rather than urgency) There is complete bladder emptying Causes: Cognitive impairment Impaired mobility Impaired dexterity Environmental reasons Location or toilets Chair height Availability of toilets Grampians Regional Continence Service - Ballarat Health Services
 There is complete bladder emptying. Causes: Cognitive impairment. Impaired mobility. Impaired dexterity. Environmental reasons. Location or toilets. Chair height. Availability of toilets. Grampians Regional Continence Service - Ballarat Health Services.")
55
Management of Functional Incontinence
Physiotherapy or occupational therapy to improve mobility Appropriate chair height Clothing alternation Remove obstacles blocking the path to the toilet Commode if toilet access is difficult Well lit and private toilet Toileting routines Grampians Regional Continence Service - Ballarat Health Services

56
Grampians Regional Continence Service - Ballarat Health Services

57
Good bladder habits An adequate fluid intake consists of
About 1½ litres per day Minimal caffeinated fluids Don’t go to the toilet “just in case”, except before bed Ability to defer when not appropriate to void Avoid constipation Correct sitting positioning on toilet Foot stool Leaning forward Relaxing abdominal muscles Grampians Regional Continence Service - Ballarat Health Services

58
Fluid Intake Fluid intake range 30 – 50ml per kg of body weight
When encouraging adequate fluid, intake take into consideration reduced sense of thirst with age & altered environment drinking habits likes & dislikes the person’s understanding ability to reach drinks. Grampians Regional Continence Service - Ballarat Health Services

59
Bladder Training a program must be individualised
obtain a base-line bladder chart ensure good fluid intake chart periodically and use comparisons as bio-feedback teach deferment techniques timed toileting a regular pattern needs to be established prompted voiding person needs help to initiate toileting Grampians Regional Continence Service - Ballarat Health Services

60
Asymptomatic bacteriuria
Presence of bacteria in the urine with the absence of clinical features 25-50% of Women in residential aged care 14-30% of Men at some time asymptomatic bacteriuria Urine odour alone Cloudy urine Why asymptomatic bacteriuria should not be treated with antibiotics Affected residents suffer no increased mortality Following course of antibiotics there is a rapid re-establishment of bacteria Increasing incidence of resistant bacteria with unnecessary antibiotic use Grampians Regional Continence Service - Ballarat Health Services

61
Symptomatic UTI’s in a non-catheterised person
Require 3 of the following features before treatment: Dysuria Fever Frequency Urgency Flank pain Suprapubic pain Worsening functional/mental status Change in character of urine Grampians Regional Continence Service - Ballarat Health Services

62
Portable Bladder Scan Ensure male/female setting is correct. Adjust the female/male setting for women who have had a hysterectomy Ensure the scan head is pointing in the correct direction 3 cms above pubic bone - midline Press button and release immediately Not to be used on pregnant women Inaccurate reading post birth Grampians Regional Continence Service - Ballarat Health Services

63
Thank you Questions?

Similar presentations








>")











>")
