Download presentation
Presentation is loading. Please wait.

1
Robotic Assisted Surgery
Marc Mitchell, DO

3
Open surgery Long incision Prostate accessed directly
Blood loss: 900 ml (about 2 units) Hospital stay: 3.5 days Catheterization: 15 days As you recall, there are currently three approaches to surgical removal: The first I will discuss is open surgery. The differences between da Vinci Prostatectomy and the traditional open procedure include the way surgeons access the prostate. In the open procedure, we have to make a long incision down the center of the abdomen and spread the tissues apart in order to gain direct access the prostate. With this approach, it is likely that you’ll lose blood and need a transfusion. Usually a hospital stay of several days is required. You will have a catheter in, which is removed after about two weeks. Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropublic Prostatectomy. BJU Int. 91(3): 175. February 2003. Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropubic Prostatectomy. BJU Int. 91(3): 175. February 2003.
 Hospital stay: 3.5 days. Catheterization: 15 days. As you recall, there are currently three approaches to surgical removal: The first I will discuss is open surgery. The differences between da Vinci Prostatectomy and the traditional open procedure include the way surgeons access the prostate. In the open procedure, we have to make a long incision down the center of the abdomen and spread the tissues apart in order to gain direct access the prostate. With this approach, it is likely that you’ll lose blood and need a transfusion. Usually a hospital stay of several days is required. You will have a catheter in, which is removed after about two weeks. Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropublic Prostatectomy. BJU Int. 91(3): 175. February Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropubic Prostatectomy. BJU Int. 91(3): 175. February")
4
Conventional laparoscopy
Small incisions Better visualization Less blood loss: 380 ml (≤ one unit) Shorter hospital stay: 1.3 days Reduced risk of infection Shorter catheterization: 7-10 days Traditional laparoscopy is different from open surgery. The procedure uses a specialized surgical camera and rigid instruments to access and remove the prostate using a series of small incisions. This approach provides better visualization of the prostate, urethra and surrounding nerves than with the traditional open approach. Since the incisions are smaller, the hospital stay is shorter and the risk of infection is reduced. 5 small incisions 1-1.5 cm (less than half an inch) Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropubic Prostatectomy. BJU Int. 91(3): 175. February 2003.
 Shorter hospital stay: 1.3 days. Reduced risk of infection. Shorter catheterization: 7-10 days. Traditional laparoscopy is different from open surgery. The procedure uses a specialized surgical camera and rigid instruments to access and remove the prostate using a series of small incisions. This approach provides better visualization of the prostate, urethra and surrounding nerves than with the traditional open approach. Since the incisions are smaller, the hospital stay is shorter and the risk of infection is reduced. 5 small incisions cm. (less than half an inch) Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropubic Prostatectomy. BJU Int. 91(3): 175. February")
5
Conventional laparoscopy drawbacks
Instruments controlled at a distance - fulcrum effect 2–D flat image video Rigid instruments – with decreased range of motion Decreases the surgeon’s precision and dexterity Surgeon fatigue Is more difficult with complex operations like radical prostatectomy Despite these advantages, there are many drawbacks to a conventional laparoscopy. For example, The surgeon operates on your tissues and organs by looking at a monitor that shows only a two dimensional image, so natural depth of field is lost. To see the target anatomy better, the surgeon may have to spread the incision wider to get a direct view. This may increase pain after surgery. The rigid instruments the surgeon works with have no wrists, which decreases precision, dexterity and control. As a result, the surgeon will also tire more quickly. Because of these drawbacks, conventional laparoscopy doesn’t lend it to complex procedures like prostatectomy. As a result, very few surgeons use this approach for prostatectomy.

6
How can we overcome these drawbacks?
da Vinci® Surgical System State-of-the-art robotic technology 3-D Visualization Intuitive Movement Improved Dexterity The da Vinci System was designed to overcome the limitations of the traditional open surgery and conventional laparoscopy. da Vinci is a state-of-the-art surgical robotic system that provides the extended capabilities necessary to remove the prostate using only a few small incisions. With da Vinci Surgery, the surgeon is seated at a nearby console and always in full control of the robotic instruments. Since the assistant is next to the patient and has direct access to the prostate, he or she can assist during complex steps of the procedure. The da Vinci System provides the surgeon with a high resolution 3–D color image It is designed to increase the surgeon’s dexterity for the difficult aspects of the procedure, especially Removing all cancer Sparing the nerves to preserve erectile function Preserving continence

7
Vision System Surgeon immersed in 3D image of the surgical field
While sitting at the console the surgeon is immersed in a three-dimensional image of the surgical field. The robotic system provides a high-resolution, magnified image that lets the surgeon see the prostate, urethra and surrounding nerve bundles in a way he has never seen this anatomy before.

8
The surgeon directs the instruments
Surgeon directs the instrument movements using Console controls Using master controls at the console, the surgeon directs the instrument movements. The System directly translates the surgeon’s hand movements into precise micro-movements of the instrument tips. The da Vinci System cannot be programmed to act on its own, and therefore requires the continuous, direct input of your surgeon.

9
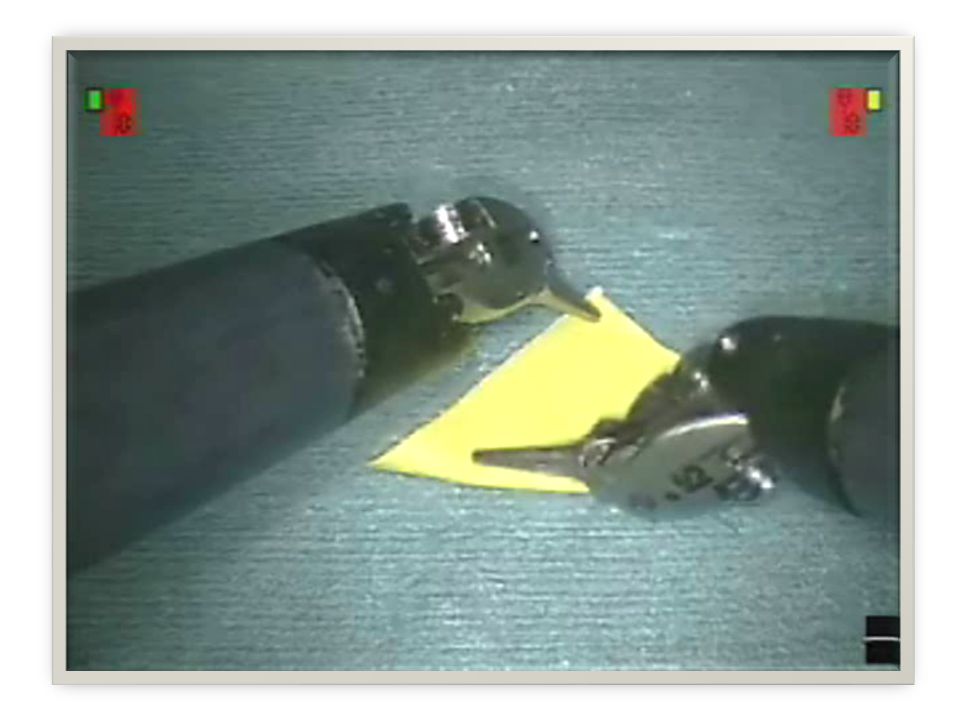
Wrist and finger movement
Conventional laparoscopic instruments are rigid with no wrists EndoWrist® Instrument tips move like a human wrist Allows increased dexterity and precision If you remember from before, conventional laparoscopic instruments are rigid and have no wrists. The EndoWrist instruments of the da Vinci System move like a human wrist. This allows the surgeon to control the instruments with the precision necessary to perform the most complex aspects of delicate procedures like prostatectomy. Specialized instruments increase dexterity, and help the surgeon to remove all cancer, to preserve the nerve bundles and make a tighter closure to the urethra.

10
Small instruments, small incisions
EndoWrist® Instruments fit through dime-sized incisions A wide range of instruments are available The instruments fit through small incisions, which are about the size of a dime. A wide range of specialized instruments are available for the surgeon to perform a very precise operation.

11
da Vinci Prostatectomy access
The da Vinci System’s enabling features allow the surgeon to perform this complex procedure using a minimally invasive approach. In the open procedure on the left, we make a long incision down the center of the abdomen. In the da Vinci Prostatectomy on the right, we make a series of small incisions, each about the size of a dime. These access points allow us to insert a high-resolution, 3D camera as well as the specialized da Vinci instruments into the abdomen. We can now see, under high-magnification, the prostate and surrounding anatomy. We can then perform a much more precise & delicate operation with the robotic instruments. Open Surgical Incision da Vinci® Prostatectomy Incision

12
Typical Prostatectomy access

13
Typical Prostatectomy incisions

14
Potential benefits of da Vinci® Prostatectomy
Fewer complications Less postoperative pain Quicker return to normal activities Shorter hospital stay Shorter catheterization Less scarring Less blood loss Faster recovery da Vinci Prostatectomy offers all the potential benefits of a minimally invasive procedure, including fewer complications, less blood loss, significantly less pain and faster return to normal daily activities.

15
Potential benefits of da Vinci® Prostatectomy
Improved cancer control Faster return to continence Faster return of potency And as a result of the enabling features offered by the da Vinci System, a da Vinci surgeon can also often achieve equal or better cancer control, equal or faster return to continence and potency as compared with traditional approaches.

16
Potential CONCERNS of da Vinci® Prostatectomy
Incomplete cancer removal Urinary Incontinence Erectile Problems Safety of Procedure Hospitalization And as a result of the enabling features offered by the da Vinci System, a da Vinci surgeon can also often achieve equal or better cancer control, equal or faster return to continence and potency as compared with traditional approaches.

17
As measured by % positive margins
Cancer control with da Vinci® Prostatectomy in T2 or organ-confined cancer Best-in-class results pathologic T2 As measured by % positive margins Traditional MIS1 7.7% Traditional Open2 5.9% da Vinci3 3.8% da Vinci4 2-4% Taking a closer look at organ-confined prostate cancer outcomes data, we show here a comparison of data from several leading prostate cancer centers. When comparing the outcomes from the best radical prostatectomy surgeons in the world, da Vinci offers equal to or better outcomes in terms of cancer removal. da Vinci Prostatectomy is now demonstrating world class cancer control outcomes as measured by positive margins. 1. Touijer K, Kuroiwa K, Saranchuk JW, Hassen WA, Trabulsi EJ, Reuter VE, Guillonneau B. Quality improvement in laparoscopic radical prostatectomy for pT2 prostate cancer: impact of video documentation review on positive surgical margin. J Urol Mar;173(3): p. 766 (Results) 2. Scardino PT. Open Radical Retropubic Prostatectomy. Presented at the American Urological Association’s Carcinoma of the Prostate Course, San Francisco, California, Sept. 30 – Oct T Ahlering. J. Urol. 175(4):217A, pg VR Patel. Urology Centers, Vestavia Hills, USA. Histopathologic Outcomes and Short Term PSA Data after Robotic Radical Prostatectomy. 500 Patients. Moderated Poster Session MP27, Wednesday, August 24, rd World Congress on Endourology and SWL 21st Basic Research Symposium August 23-26, 2005, Amsterdam, The Netherlands. J Endourol Aug.; 19, Supplement 1: A135.
: p. 766 (Results) 2. Scardino PT. Open Radical Retropubic Prostatectomy. Presented at the American Urological Association’s Carcinoma of the Prostate Course, San Francisco, California, Sept. 30 – Oct T Ahlering. J. Urol. 175(4):217A, pg VR Patel. Urology Centers, Vestavia Hills, USA. Histopathologic Outcomes and Short Term PSA Data after Robotic Radical Prostatectomy. 500 Patients. Moderated Poster Session MP27, Wednesday, August 24, rd World Congress on Endourology and SWL 21st Basic Research Symposium August 23-26, 2005, Amsterdam, The Netherlands. J Endourol Aug.; 19, Supplement 1: A135.")
18
Continence with da Vinci® Prostatectomy (defined as no pads)
Best-in-class results 3 mo 6 mo 12 mo Traditional Open1 54 % 80% 93% Traditional laparoscopy2 N/A 74% 97% da Vinci3 92.9% 94.9% 97.4% da Vinci4 82% 89% 98% Now let’s look at urinary continence outcomes. In this slide, we will compare “Best in Class” outcomes for open and traditional laparoscopic surgery with top da Vinci Prostatectomy results. Comparing two important end points, “Early Return to Continence” (defined as a return to urinary continence at 3 – 6 months) and overall return of “Urinary Continence” (defined as a return to urinary continence at 12 months), you can see that da Vinci offers equal to or better outcomes at all three end points. Based on these outcomes, da Vinci Prostatectomy demonstrates equal to or better urinary continence outcomes as compared to best results from open and laparoscopic surgery. 1. Walsh PC. Patient-reported urinary continence and sexual function after anatomic radical prostatectomy. J Urol Jul;164(1):242. p. 59 table Rassweiler J, Sentker L, Seemann O, Hatzinger M, Rumpelt HJ. Laparoscopic radical prostatectomy with the Heilbronn technique: an analysis of the first 180 cases. J Urol Dec;166(6): Locke, DR, Klimberg IW and Sessions RP. Robotic Radical Prostatectomy With Continence And Potency Sparing Technique: An Analysis Of The First 250 Cases. Submitted To Journal Of Urology, Publication Date TBD. p. 5 table Patel VR, Tully AS, Holmes R, Lindsay J. Robotic radical prostatectomy in the community setting--the learning curve and beyond: initial 200 cases. J Urol Jul;174(1): p. 270 table 3.
 and overall return of Urinary Continence (defined as a return to urinary continence at 12 months), you can see that da Vinci offers equal to or better outcomes at all three end points. Based on these outcomes, da Vinci Prostatectomy demonstrates equal to or better urinary continence outcomes as compared to best results from open and laparoscopic surgery. 1. Walsh PC. Patient-reported urinary continence and sexual function after anatomic radical prostatectomy. J Urol Jul;164(1):242. p. 59 table Rassweiler J, Sentker L, Seemann O, Hatzinger M, Rumpelt HJ. Laparoscopic radical prostatectomy with the Heilbronn technique: an analysis of the first 180 cases. J Urol Dec;166(6): Locke, DR, Klimberg IW and Sessions RP. Robotic Radical Prostatectomy With Continence And Potency Sparing Technique: An Analysis Of The First 250 Cases. Submitted To Journal Of Urology, Publication Date TBD. p. 5 table Patel VR, Tully AS, Holmes R, Lindsay J. Robotic radical prostatectomy in the community setting--the learning curve and beyond: initial 200 cases. J Urol Jul;174(1): p. 270 table 3.")
19
Potency with da Vinci® Prostatectomy
Best-in-class results for … Open1 da Vinci 2 da Vinci3 Average age 50.1 55.7 57.4 Intercourse 71 % 74 % 86 % Average potency score 15.7 19.3 21.9 Last, but not least, we will compare “Best in Class” endpoints for potency. Here, we are looking at the best available potency outcomes with an open approach and with da Vinci Prostatectomy. In this group of patients, we can see more da Vinci patients had reported having intercourse. Moreover, the da Vinci patient’s overall potency score was up to 40% better. Please note that the da Vinci patients were also up to 5 ½ years older on average age as compared to the open surgery patients. In summary, da Vinci Prostatectomy patients had a better overall recovery of sexual function. 1. Parsons JK, Marschke P, Maples P, Walsh PC. Effect of methylprednisolone on return of sexual function after nerve-sparing radical retropubic prostatectomy. Urology Nov;64(5): 2. Ahlering T. The UC Irvine Experience: Potency Preservation. Presented at UC Irivine’s 2006 ART (Advanced Robotic Techniques) of Prostatectomy Symposium, January 5, 2006, Anaheim, Calif. 3. Menon M, Kaul S, Bhandari A, Shrivastava A, Tewari A, Hemal A. Potency following robotic radical prostatectomy: a questionnaire based analysis of outcomes after conventional nerve sparing and prostatic fascia sparing techniques. J Urol Dec;174(6):2291-6, discussion p fig. 2.
: Ahlering T. The UC Irvine Experience: Potency Preservation. Presented at UC Irivine’s 2006 ART (Advanced Robotic Techniques) of Prostatectomy Symposium, January 5, 2006, Anaheim, Calif. 3. Menon M, Kaul S, Bhandari A, Shrivastava A, Tewari A, Hemal A. Potency following robotic radical prostatectomy: a questionnaire based analysis of outcomes after conventional nerve sparing and prostatic fascia sparing techniques. J Urol Dec;174(6):2291-6, discussion p fig. 2.")
20
Summary of outcomes Variable Open da Vinci® Cancer margins 5.9%1 2-4%2
Catheter3 15 days 5 Complications3 15% Return to potency at 12 mo. 71% 1 86% 4 Blood loss3 900 ml 153 Hospitalization3 3.5 days 1.2 Compare the benefits and decide what’s best for you. Published data has shown that the robotic-assisted procedure is less invasive, with shorter hospital stay, less blood loss, and decreased catheter time compared to the open surgical approach. And recent clinical studies also suggest that the da Vinci System may help surgeons provide better cancer control and a lower incidence of impotence and incontinence with da Vinci Prostatectomy.[1] [1] Cancer control is defined in part by margin rates and PSA test scores. The following studies provide support for these claims: Ahlering TE, Woo D, Eichel L, Lee DI, Edwards R, Skarecky DW. Robot-assisted versus open radical prostatectomy: a comparison of one surgeon's outcomes. Urology May;63(5): Menon M, Tewari A, Peabody JO, Shrivastava A, Kaul S, Bhandari A, Hemal AK. Vattikuti Institute prostatectomy, a technique of robotic radical prostatectomy for management of localized carcinoma of the prostate: experience of over 1100 cases. Urol Clin North Am Nov;31(4): Tewari A, Srivasatava A, Menon M; Members of the VIP Team. A prospective comparison of radical retropubic and robot-assisted prostatectomy: experience in one institution. BJU Int Aug;92(3): 1 Parsons JK, Marschke P, Maples P, Walsh PC. Effect of methylprednisolone on return of sexual function after nerve-sparing radical retropubic prostatectomy. Urology Nov;64(5): 2 VR Patel. Urology Centers, Vestavia Hills, USA. Histopathologic Outcomes and Short Term PSA Data after Robotic Radical Prostatectomy. 500 Patients. Moderated Poster Session MP27, Wednesday, August 24, rd World Congress on Endourology and SWL 21st Basic Research Symposium August 23-26, 2005, Amsterdam, The Netherlands. J Endourol Aug.; 19, Supplement 1: A135. 3 Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropublic Prostatectomy. BJU Int. 91(3): 175. February 2003. 4 Menon M, Kaul S, Bhandari A, Shrivastava A, Tewari A, Hemal A. Potency following robotic radical prostatectomy: a questionnaire based analysis of outcomes after conventional nerve sparing and prostatic fascia sparing techniques. J Urol Dec;174(6):2291-6, discussion p fig. 2.
: Menon M, Tewari A, Peabody JO, Shrivastava A, Kaul S, Bhandari A, Hemal AK. Vattikuti Institute prostatectomy, a technique of robotic radical prostatectomy for management of localized carcinoma of the prostate: experience of over 1100 cases. Urol Clin North Am Nov;31(4): Tewari A, Srivasatava A, Menon M; Members of the VIP Team. A prospective comparison of radical retropubic and robot-assisted prostatectomy: experience in one institution. BJU Int Aug;92(3): Parsons JK, Marschke P, Maples P, Walsh PC. Effect of methylprednisolone on return of sexual function after nerve-sparing radical retropubic prostatectomy. Urology Nov;64(5): VR Patel. Urology Centers, Vestavia Hills, USA. Histopathologic Outcomes and Short Term PSA Data after Robotic Radical Prostatectomy. 500 Patients. Moderated Poster Session MP27, Wednesday, August 24, rd World Congress on Endourology and SWL 21st Basic Research Symposium August 23-26, 2005, Amsterdam, The Netherlands. J Endourol Aug.; 19, Supplement 1: A Data on blood loss, LOS and catheterization from Menon M. Robotic Radical Retropublic Prostatectomy. BJU Int. 91(3): 175. February Menon M, Kaul S, Bhandari A, Shrivastava A, Tewari A, Hemal A. Potency following robotic radical prostatectomy: a questionnaire based analysis of outcomes after conventional nerve sparing and prostatic fascia sparing techniques. J Urol Dec;174(6):2291-6, discussion p fig. 2.")
21
Prostatectomy: daVinci vs Traditional
Pain Medication Requirements Time on IV Pain Medications Regular Diet morphine eq's after surgery hours Open Prostatectomy 31.4 48 24.5 da Vinci Prostatectomy 5 10.5 13.5

22
Prostatectomy: daVinci vs Traditional
Surgery Time Hospital Admission minutes hours Open Prostatectomy 338 68.5 da Vinci Prostatectomy 229 26.5

23
Hysterectomy: daVinci vs Traditional
Surgery Time Hospital Admission minutes hours Abdominal Hysterectomy 116 51 Laparoscopic AV 108 26 da Vinci 152 25

24
Hysterectomy: daVinci vs Traditional
Total Pain Medications Time on IV Pain Medications Regular Diet equivalents after surgery hours Abdominal Hysterectomy 56.2 26.8 28 Laparoscopic AV 36.4 24 21.8 daVinci 22.6 22 14

25
da Vinci® Robotics I appreciate your joining me in this prostate cancer patient education seminar. Thank you.

26
Changing the Experience of Surgery
I appreciate your joining me in this prostate cancer patient education seminar. Thank you.

Similar presentations