Download presentation
Presentation is loading. Please wait.

1
Department of Gerontology
Incontinence Dr. Gary Sinoff Department of Gerontology University of Haifa

2
Incontinence

3
Definition 2 - P C - M E

4
Definition INCONTINENCE: Involuntary loss of urine or stool in sufficient amount or frequency to constitute a social and/or health problem. A heterogeneous condition that ranges in severity from dribbling to continuous incontinence. If individuals lose only one or two drops of urine when they don’t want to, that’s considered incontinence!

5
Myths: People who are incontinent are: Very old Feeble Senile
Totally dependent No longer in control

6
Brussels

7
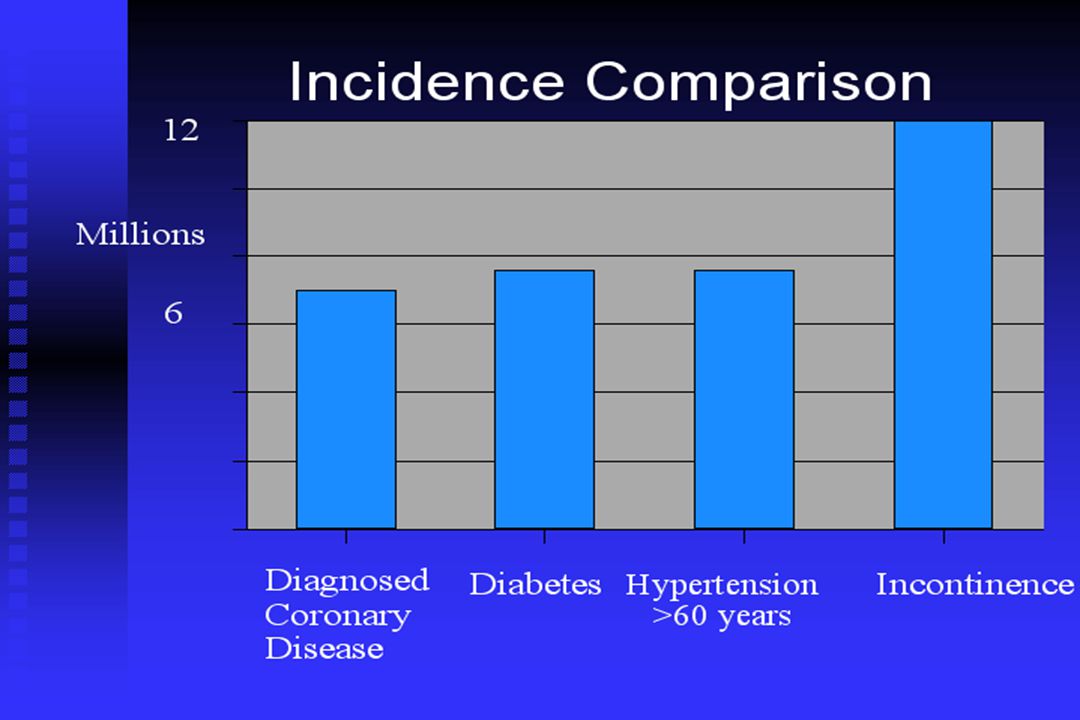
How Common is Urinary Incontinence?
Prevalence increases with age 25-30% of community dwelling older women 10-15% of community dwelling older men 50% of nursing home residents

9
Rate of Seeking Help * **
* NIH Consensus Statement on Urinary Incontinence,1988 ** Holts et al, 1988

10
Under-Diagnoses and Under-Treated
Only 32% of primary care physicians routinely ask about incontinence 50-75% of patients never describe symptoms to physicians 80% of urinary incontinence can be cured or improved

11
Why is Incontinence Important?
Social stigmata - leads to restricted activities and depression Medical complications - skin breakdown, increased urinary tract infections Institutionalization - UI is the second leading cause of nursing home placement

12
Anatomy of Micturition
Detrusor muscle External and Internal sphincter CNS control Pons - facilitates Cerebral cortex – inhibits Hormonal effects - estrogen

13
Peripheral Nerves in Micturition

14
Peripheral Nerves in Micturition
Parasympathetic (cholinergic) - Bladder contraction Sympathetic - Bladder Relaxation Sympathetic - Bladder Relaxation (β adrenergic) Sympathetic - Bladder neck and urethral contraction (α adrenergic) Somatic (Pudendal nerve) - contraction pelvic floor musculature
 - Bladder contraction. Sympathetic - Bladder Relaxation. Sympathetic - Bladder Relaxation (β adrenergic) Sympathetic - Bladder neck and urethral contraction (α adrenergic) Somatic (Pudendal nerve) - contraction pelvic floor musculature.")
15
Bladder Pressure-Volume Relationship

16
Potentially Reversible Causes
D - Delirium I - Infection A - Atrophic vaginitis or urethritis P - Pharmaceuticals P - Psychological disorders E - Endocrine disorders R - Restricted mobility S - Stool impaction

17
Degree of Bother YES : 53.7%

18
Medications That May Cause Incontinence
Diuretics Anticholinergics - antihistamines, antipsychotics, antidepressants Sedatives/hypnotics Alcohol Narcotics Calcium channel blockers

19
Other factors for urinary incontinence
Sociocultural Psychological Muscle tone damage Fluid intake Diseases Surgery

20
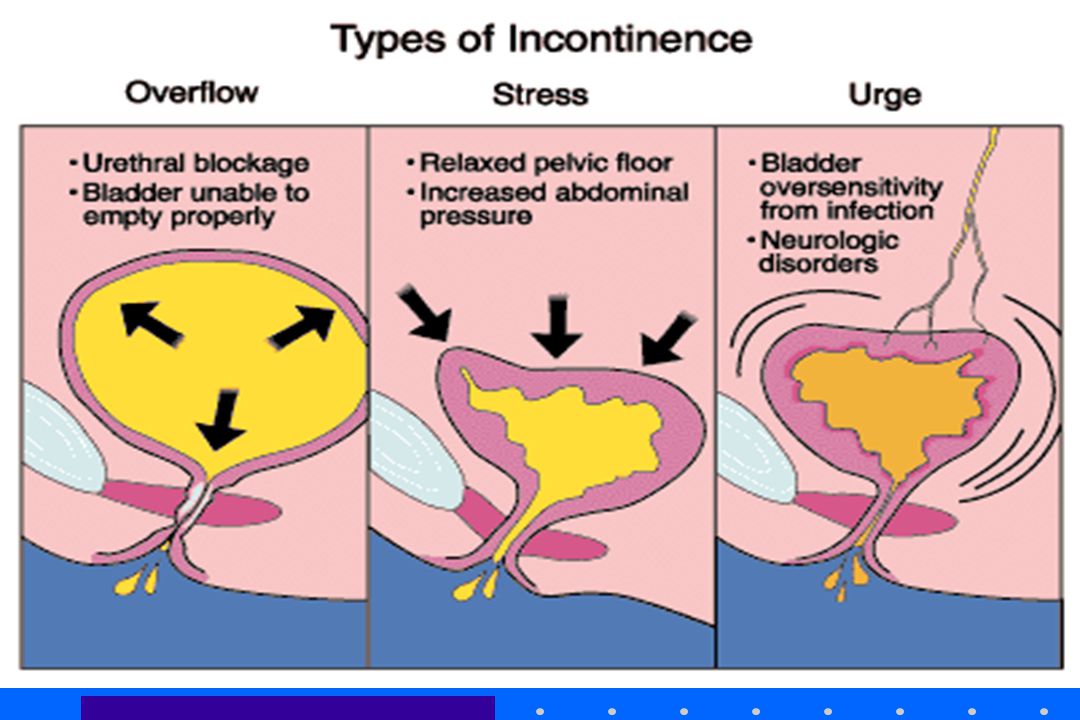
Categories of Incontinence
Urge incontinence Stress incontinence Overflow incontinence Functional incontinence

22
Incontinence In women 49% stress incontinence 22% urge incontinence
29% mixed stress & urge In men % urge incontinence

23
Urge Incontinence Most common cause of UI >75 years of age
Other Names: detrusor hyperactivity, detrusor instability, irritable bladder, spastic bladder Most common cause of UI >75 years of age Abrupt desire to void cannot be suppressed Usually idiopathic Causes: infection, tumor, stones, atrophic vaginitis or urethritis, stroke, Parkinson’s Disease, dementia

24
Stress Incontinence Most common type in women < 75 years old
Occurs with increase in abdominal pressure; cough, sneeze, laughing, etc. Hypermotility of bladder neck and urethra; associated with aging, hormonal changes, trauma of childbirth or pelvic surgery (85% of cases) Intrinsic sphincter problems; due to pelvic/incontinence surgery, pelvic radiation, trauma, neurogenic causes (15% of cases)
 Intrinsic sphincter problems; due to pelvic/incontinence surgery, pelvic radiation, trauma, neurogenic causes (15% of cases)")
25
Overflow Incontinence
Over distention of bladder Bladder outlet obstruction; stricture, BPH, cystocele, fecal impaction Non-contractile baldder (hypoactive detrusor or atonic bladder); diabetes, MS, spinal injury, medications
; diabetes, MS, spinal injury, medications.")
26
Functional Incontinence
Does not involve lower urinary tract Result of psychological, cognitive or physical impairment

27
Diagnostic Tests Stress test (diagnostic for stress incontinence; specificity >90%) Post-void residual Blood Tests (calcium, glucose, BUN, Cr) Urine Culture Simple (bedside) Cystometrics
 Urine Culture. Simple (bedside) Cystometrics.")
28
Urodynamics - Lower urinary tract
Uroflowmetry Cystometrography External sphincter electromyography Pressure flow study Videourodynamic study Urethral pressure profilometry

29
In-Hospital Use of Continence Aids and New-Onset Urinary Incontinence in Adults Aged 70 and Older Zisberg, A, Sinoff, G, Gur-Yaish, N, Admi, E, Shadmi, E OBJECTIVES: To describe the types of continence aids that older adults hospitalized in acute medical units use and to test the association between use of continence aids and development of new urinary incontinence (UI) at discharge. DESIGN: Prospective cohort study. SETTING: A 900-bed teaching hospital in Israel. PARTICIPANTS: Three hundred fifty-two acute medical patients aged 70 and older who were continent before admission. MEASUREMENTS: In-hospital use of continence aids was assessed according to participant self-report on use of urinary catheters (UCs) or adult diapers o of self-toileting. The development of new UI was defined as participant report of inability to control voiding at discharge. Multivariate analyses mode led the association between use of continence aids (vs self-toileting) and the development of new UI, controlling for baseline functional and cognitive status, disease severity, age, and length of stay.
 at discharge. DESIGN: Prospective cohort study. SETTING: A 900-bed teaching hospital in Israel. PARTICIPANTS: Three hundred fifty-two acute medical patients aged 70 and older who were continent before admission. MEASUREMENTS: In-hospital use of continence aids was assessed according to participant self-report on use of urinary catheters (UCs) or adult diapers o of self-toileting. The development of new UI was defined as participant report of inability to control voiding at discharge. Multivariate analyses mode led the association between use of continence aids (vs self-toileting) and the development of new UI, controlling for baseline functional and cognitive status, disease severity, age, and length of stay.")
30
New Onset Incontinence
RESULTS: Of the 352 participants, 58 (16.5%) used adult diapers, and 27 (7.7%) had a UC during most of the hospital stay. Sixty (17.1%) participants developed new UI at discharge. The odds of developing new UI were 4.26 (95% confidence interval (CI)51.53–11.83) times higher for UC users and 2.62 (95% CI51.17–5.87) times higher for adult diaper users than for the self-toileting group, controlling for the above risk factors. CONCLUSION: The use of adult diapers and UCs during acute hospitalization is associated with the development of new UI at discharge. The management of continence in hospitalized older adults requires more diligence, and further investigation is needed to devise continence promotion methods in hospital settings. J Am Geriatr Soc 2011
 used adult diapers, and 27 (7.7%) had a UC during most of the hospital stay. Sixty (17.1%) participants developed new UI at discharge. The odds of developing new UI were 4.26 (95% confidence interval (CI)51.53–11.83) times higher for UC users and 2.62 (95% CI51.17–5.87) times higher for adult diaper users than for the self-toileting group, controlling for the above risk factors. CONCLUSION: The use of adult diapers and UCs during acute hospitalization is associated with the development of new UI at discharge. The management of continence in hospitalized older adults requires more diligence, and further investigation is needed to devise continence promotion methods in hospital settings. J Am Geriatr Soc")
31
Treatment Options 1

32
Lifestyle choices Reduce or eliminate caffeine
Reduce or eliminate alcohol Drink 6 to 8 glasses of water daily Quit smoking Weight control Follow a healthy diet high in fiber Reduce physical barriers to toilet (use bedside commode)
")
33
Timed Voiding Regular scheduled pattern of voiding where the intervals between voiding are gradually increased. It reduces irritability of the bladder Reverses bad habits No longer needing to camp out by the bathroom promotes freedom and independence once again.

34
Treatment Options Bladder training
Patient education Scheduled voiding Positive reinforcement Pelvic floor exercises (Kegel Exercises) Biofeedback Caregiver interventions Scheduled toileting Habit training Prompted voiding 2
 Biofeedback. Caregiver interventions. Scheduled toileting. Habit training. Prompted voiding. 2.")
35
Treatment for Detrusor Overactivity
Behavioral therapy Bladder drill Timed/prompted toileting Medical therapy Anticholinergic Tricyclic antidepressants Neurotoxins Estrogens Electrical therapy Vaginal or anal electrical stimulation Trancutaneous electrical simulation Surgical therapy Partial detrusor myomectomy Augmentation cystoplasty Urinary diversion

36
Pharmacological Interventions
Urge Incontinence Oxybutynin (Novitropan) Imipramine (Tofranil) Stress Incontinence Phenylpropanolamine (Alcinal) Pseudo-Ephedrine (Histafed, etc.) Estrogen (orally, transdermally or transvaginally)
 Imipramine (Tofranil) Stress Incontinence. Phenylpropanolamine (Alcinal) Pseudo-Ephedrine (Histafed, etc.) Estrogen (orally, transdermally or transvaginally)")
37
Surgical Interventions
Surgery is reported to “cure” 4 out of 5 cases, but success rate drops to 50% after 10 years. Urethral Hypermotility Marshall-Marchetti-Kantz procedure Needle neck suspension Intrinsic sphincter deficiency Sling procedure

38
Other Interventions Pessaries
Periurethral bulking agents (periurethral injection of collagen, fat or silicone) Diapers or pads Chronic catheterization Periurethral or suprapubic Indwelling or intermittant
 Diapers or pads. Chronic catheterization. Periurethral or suprapubic. Indwelling or intermittant.")
39
Leg Bags

40
Designer Diapers

41
Pessaries

42
Indwelling Catheter

43
Fecal Incontinence

44
Fecal Incontinence “The inability to control the passage of flatus, liquid or solid stool” 2% prevalence community, increases in NH Profoundly disabling, also on body image Number of different etiologies Variety of medical and surgical treatments available

45
Normal continence mechanism
Internal sphincter (smooth muscle involuntary): maintains high resting tone External sphincter (skeletal muscle voluntary): important in the voluntary inhibition of the defaecatory reflex
: maintains high resting tone. External sphincter (skeletal muscle voluntary): important in the voluntary inhibition of the defaecatory reflex.")
46
Factors Affecting GIT Elimination
Physiological changes with age Physical Activity Diet Psychological Factors Surgical

47
Classification of Incontinence
Pseudoincontinence soiling, urgency, frequency Overflow incontinence Incontinence with abnormal pelvic floor

48
Pseudo-incontinence Perineal soiling Urgency Frequency
hemorrhoidal prolapse fistula en ano incomplete defecation perianal dermatoses Urgency non compliant rectum (radiation) IBD absent rectal reservoir Frequency diarrheal states ie IBD, autonomic neuropathy, parasites, toxins
 IBD. absent rectal reservoir. Frequency. diarrheal states ie IBD, autonomic neuropathy, parasites, toxins.")
49
Overflow Incontinence
Rectal fecal impaction decreased rectal sensation obtuse anorectal angle chronic stimulation of rectoanal inhibitory reflex Neoplasm

50
Abnormal pelvic floor Neurogenic/Infiltrative Sphincter disruption
pudendal neuropathy generalized neuropathy or cord lesion Diabetes Mellitus and Scleroderma Sphincter disruption Obstetric Surgical Trauma

51
Cause of Incontinence Sphincter degeneration (internal)
Sphincter damage (external) Nerve damage (central or peripheral) Rectal causes – (changes in rectal capacity, elasticity or function) Faecal impaction - (chronically distended rectum - chronically relaxed internal sphincter)
 Nerve damage (central or peripheral) Rectal causes – (changes in rectal capacity, elasticity or function) Faecal impaction - (chronically distended rectum - chronically relaxed internal sphincter)")
52
Examination PR examination – tone, contractile strength, perineal descent on straining Impacted and overflow incontinence Anal Fistula Haemorrhoids Rectocele

53
Anorectal physiology laboratory
Functional - Manometric studies, Dynamic Fluoroscopy Anatomical - Endoanal ultrasound, MRI Neurological - Pudendal nerve latency tests

54
Manometry Voluntary anal squeeze pressure
Low resting pressure: internal sphincter abnormality Reduced squeeze pressures: external sphincter problem Fatigueability of the external sphincter: relevance in urge incontinence

55
Endoanal ultrasound Anatomical information
Likely be of benefit post obstetrics or surgical trauma After first vaginal delivery 30% have demonstrated sphincter defects 1/3 of these develops symptoms incontinence/ urgency

56
Normal Endo anal ultrasound
Internal sphincter external sphincter Figure 12. Transverse endoanal US image obtained with a 10-MHz transducer shows normal sphincter anatomy in a 37-year-old asymptomatic male volunteer. Subepithelial tissues (SE), the internal sphincter (IS), the intersphincteric space and longitudinal muscle (IL), and the external sphincter (ES) are visible.
, the internal sphincter (IS), the intersphincteric space and longitudinal muscle (IL), and the external sphincter (ES) are visible.")
57
Managing Bowel Incontinence:
Note when incontinence is likely to occur and put patient on bedpan at that time. Keep the skin clean and dry by using proper hygienic measures. Change bed linens and clothing as necessary. Confer with the physician about using a suppository or daily cleansing enema. Repeated rectal examinations

58
Next Week Iatrogenic Damage

Similar presentations






>")












,MRCGP,MRCPE.>")