Download presentation
Presentation is loading. Please wait.

1
Prevention Treatment of Osteoporosis in Geriaterics
Dr H. Soleimani Department of Rheumatology Shahid Sadughi Hospital

2
But, do I really have to take those medicines?
Will I end up like my mother? Fracture Risk Assessment Intervention Thresholds I saw on the News last night..... Treatment Follow-up

3
Leading the Effort to Help Prevent and Treat Osteoporosis
Pharmacotherapy (antiresorptives and anabolics) Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Pyramid for Osteoporosis Prevention and Treatment What does this mean for your patients? US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General; 2004.
 Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Pyramid for Osteoporosis Prevention and Treatment. What does this mean for your patients US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General;")
4
A Few Facts about Osteoporosis and Bone Density Measurement

5
Osteoporosis Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture NIH Consensus Development Conference, March 2000 Normal Bone Osteoporotic Bone

6
Fractures in Women Are Common: Incidence of Chronic Diseases
2.0 1,500,000 1.5 Annual Incidence, million 1.0 373,000 345,000 0.5 250,000 211,240 Fractures in Women Are Common: Incidence of Chronic Diseases This slide demonstrates that the incidence of new cases of osteoporotic fracture in women each year is far greater than the incidence of heart attack, stroke, and breast cancer combined.1–3 Hip fracture incidence alone exceeds that of breast cancer.1 This information, with the information on the previous slide, further emphasizes that osteoporosis should be considered a major health concern among postmenopausal women in the United States. The point is not to suggest that osteoporosis is more important than the other diseases but that it should be managed as routinely as are the other diseases. References: 1. Riggs BL, Melton LJ III. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone. 1995;17(suppl):505S–511S. 2. American Stroke Association. Heart disease and stroke statistics––2005 update. Available at: Accessed August 24, 2005. 3. American Cancer Society. Cancer facts & figures: Available at: Accessed August 24, 2005. Fracture1 Hip fracture1 Heart attack2 Stroke2 Breast cancer3 Women with osteoporosis All women Risk of osteoporotic fracture in 1 year is greater than combined risk of heart attack, stroke, and breast cancer. 1. Riggs BL, Melton LJ III. Bone. 1995;17(suppl):505S–511S. 2. American Stroke Association. Heart disease and stroke statistics––2005 update. Available at: Accessed August 24, 2005. 3. American Cancer Society. Cancer facts & figures; Available at: Accessed August 24, 2005.
:505S–511S. 2. American Stroke Association. Heart disease and stroke statistics––2005 update. Available at: Accessed. August 24, American Cancer Society. Cancer facts & figures: Available at: Accessed August 24, Fracture1. Hip fracture1. Heart attack2. Stroke2. Breast cancer3. Women with osteoporosis. All women. Risk of osteoporotic fracture in 1 year is greater than. combined risk of heart attack, stroke, and breast cancer. 1. Riggs BL, Melton LJ III. Bone. 1995;17(suppl):505S–511S. 2. American Stroke Association. Heart disease and stroke statistics––2005 update. Available at: Accessed August 24, American Cancer Society. Cancer facts & figures; Available at: Accessed August 24,")
8
Practical Definition of Osteoporosis
A fall from a sitting or standing height that causes a fracture

9
Bone Mineral Density Testing “Quantitating the Bone Mass”

10
Central Devices GE Lunar Prodigy Hologic Delphi

11
Central DXA Measures bone density at the hip and spine
DXA image of the hip DXA image of the lumbar spine

12
NOF 2008 Guidelines Who Should be Tested?
Women age 65 and older Men age 70 and older Women and men over 50 with risk factors Patients with a fracture after age 50

13
Vertebral Fracture Assessment
Lateral Spine Imaging with Fan-Array Dual Energy X-ray Absorptiometry

15
Surgeon General’s Report on Bone Health and Osteoporosis
Leading the Effort to Help Prevent and Treat Osteoporosis Pharmacotherapy (antiresorptives and anabolics) Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Surgeon General’s Report on Bone Health and Osteoporosis Pyramid for Osteoporosis Prevention and Treatment What does this mean for your patients? US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General; 2004.
 Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Surgeon General’s Report on Bone Health and Osteoporosis. Pyramid for Osteoporosis Prevention and Treatment. What does this mean for your patients US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General;")
16
Lifestyle Issues Tobacco- eliminate it Alcohol – moderate it
Food – eat it Exercise – do it Fall Prevention – work on it

17
Lifestyle Issues Tobacco - eliminate it Alcohol – moderate it
Nutrition - adequate weight, protein-- magnesium, trace elements....multivite Exercise – strength, aerobic, flexibility, balance Fall prevention- home safety, shoes, walking aids, glasses 17

18
Nutrition Appropriate Body Weight Adequate nutrition
BMI Adequate nutrition Protein Multi-vitamin daily C, D, K, Copper, Manganese, Zinc, Phosphorus Nutritional supplements Ensure, Boost

19
Nutrition Milk, Yogurt Calcium, magnesium, potassium, phosphorus, zinc, protein, vitamin A, vitamin D, vitamin B12, riboflavin Risk reduction for Osteoporosis, hypertension, obesity, colon cancer, diabetes, metabolic syndrome

20
What are the therapeutic options?
Exercise and prevention of falls improve quality of life improve muscle strength and balance moderate walking reduced risk of hip Fx* treat cataract Use of hip protectors*

21
Exercise Walking reduces hip fracture risk
4 hours per week reduced hip fracture by 41% in a study of 61,200 women JAMA 2002 Activity of any type reduces fracture risk Balance, Strength, Flexibility, Aerobic

22
Exersice 1. Exercises involving resistance training appropriate for the individual’s age and functional capacity and/or weightbearing aerobic exercises are recommended for those with osteoporosis or at risk for osteoporosis [grade B].

23
Exersice Exercises to enhance core stability and thus to compensate for weakness or postural abnormalities are recommended for individuals who have had vertebral fractures [grade B].

24
Exersice Exercises that focus on balance, such as tai chi, or on balance and gait training should be considered for those at risk of falls [grade A].
![Exersice Exercises that focus on balance, such as tai chi, or on balance and gait training should be considered for those at risk of falls [grade A].](http://slideplayer.com/slide/5739834/19/images/24/Exersice+Exercises+that+focus+on+balance%2C+such+as+tai+chi%2C+or+on+balance+and+gait+training+should+be+considered+for+those+at+risk+of+falls+%5Bgrade+A%5D..jpg "Exersice Exercises that focus on balance, such as tai chi, or on balance and gait training should be considered for those at risk of falls [grade A].")
25
Falling Medications, Alcohol Balance programs Strength training
Safety at home Hip protectors Walking aids

26
Hip Protectors

27
Hip Protector Use of hip protectors should be considered for older adults residing in long-term care facilities who are at high risk for fracture [grade B].

28
Calcium mg “Calcium has been singled out as a major health concern today because it is critically important to bone health and the average American consumes levels of calcium that are far below the amount recommended for optimal bone health.” General’s Report on Bone Health 2004

29
Calcium 1200 mg Dietary Fortified foods Calcium citrate
Taken with or without food Calcium carbonate Taken with food Divided doses

30
Calcium The total daily intake of elemental calcium (through diet and supplements) for individuals over age 50 should be 1200 mg [grade B].
![Calcium The total daily intake of elemental calcium (through diet and supplements) for individuals over age 50 should be 1200 mg [grade B].](http://slideplayer.com/slide/5739834/19/images/30/Calcium+The+total+daily+intake+of+elemental+calcium+%28through+diet+and+supplements%29+for+individuals+over+age+50+should+be+1200+mg+%5Bgrade+B%5D..jpg "Calcium The total daily intake of elemental calcium (through diet and supplements) for individuals over age 50 should be 1200 mg [grade B].")
31
Vitamin D IU ? “Vitamin D is important for good bone health because it aids in the absorption and utilization of calcium. There is a high prevalence of Vitamin D deficiency in nursing home residents, hospitalized patients, and adults with hip fractures.” …..and many others General’s Report on Bone Health 2004 31

32
Vitamin D Sufficiency > 32 ng/ml Comfort zone- 40s, 50s
Many wellness relationships Insufficiency < 32 ng/ml Disease states New England Journal of Medicine July Medical Progress: Vitamin D Deficiency M F Holick IU daily for patients 50 + ...although some elderly patients may require 2000 IU/day...... NOF Clinician’s Guide 2008 32

33
Vit D For healthy adults at low risk of vitamin D deficiency, routine supplementation with 400–1000 IU (10–25 μg) vitamin D3 daily is recommended [grade D].
 vitamin D3 daily is recommended [grade D].")
34
Vit D For adults over age 50 at moderate risk of vitamin D deficiency, supplementation with 800–1000 IU (20–25 μg) vita min D3 daily is recommended. To achieve optimal vitamin D status, daily supplementation with more than 1000 IU (25 μg) may be required. Daily doses up to 2000 IU (50 IU (25 μg) may be required. Daily doses up to 2000 IU (50 μg) are safe and do not necessitate monitoring [grade C].
 vita min D3 daily is recommended. To achieve optimal vitamin D status, daily supplementation with more than 1000 IU (25 μg) may be required. Daily doses up to 2000 IU (50 IU (25 μg) may be required. Daily doses up to 2000 IU (50 μg) are safe and do not necessitate monitoring [grade C].")
35
Vit D For individuals receiving pharmacologic therapy for osteoporosis, measurement of serum 25-hydroxyvitamin D should follow three to four months of adequate supplementation and should not be repeated if an optimal level (≥ 75 nmol/L) is achieved [grade D].
 is achieved [grade D].")
36
Vitamin D Improves calcium absorption
Direct action on building bone matrix Decreases FALLS Increases muscle mass and strength Etc etc

37
Leading the Effort to Help Prevent and Treat Osteoporosis
Pharmacotherapy (antiresorptives and anabolics) Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Pyramid for Osteoporosis Prevention and Treatment What does this mean for your patients? US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General; 2004.
 Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Pyramid for Osteoporosis Prevention and Treatment. What does this mean for your patients US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General;")
38
Kanis Osteoporos Int 2008;19:385-397
WHO Risk Factors Age (50-90), gender and clinical risk factors: BMI Prior fragility fracture Parental history of hip fracture Current tobacco smoking Ever long-term use of glucocorticoids Rheumatoid arthritis or other secondary causes Alcohol intake 3 or more units daily Kanis Osteoporos Int 2008;19: 38
, gender and clinical risk factors: BMI. Prior fragility fracture. Parental history of hip fracture. Current tobacco smoking. Ever long-term use of glucocorticoids. Rheumatoid arthritis or other secondary causes. Alcohol intake 3 or more units daily. Kanis Osteoporos Int 2008;19:")
39
39

40
Frailty Factor Acute Medical Illnesses Chronic Medical Illnesses
Inactivity Falling 40

41
Medication Check Corticosteroids DepoProvera Anticonvulsants Lupron
Aromatase inhibitors Thyroid hormone SSRIs DepoProvera Lupron Narcotics Cancer Chemo Lithium Thiazolidinediones 41

42
Check Lab Tests

43
Check Lab Tests “Secondary Cause Work Up”
Blood count (CBC) Chemistries (CMP) Calcium, Phosphorus Kidney tests Liver tests Alk Phos Vitamin D (25hydroxyD) Thyroid (TSH) Parathyroid (intact PTH) Celiac (IgA anti-t-TGase antibody) Malabsorption/Hypercalciuria (24 hr Urine Calcium) Myeloma (SPIEP) Arthritis (ESR etc.) Hormones (Testosterone) Bone Turnover markers (NTX,CTX) 43
 Chemistries (CMP) Calcium, Phosphorus. Kidney tests. Liver tests. Alk Phos. Vitamin D (25hydroxyD) Thyroid (TSH) Parathyroid (intact PTH) Celiac (IgA anti-t-TGase antibody) Malabsorption/Hypercalciuria. (24 hr Urine Calcium) Myeloma (SPIEP) Arthritis (ESR etc.) Hormones (Testosterone) Bone Turnover markers (NTX,CTX) 43.")
44
Leading the Effort to Help Prevent and Treat Osteoporosis
Pharmacotherapy (antiresorptives and anabolics) Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Pyramid for Osteoporosis Prevention and Treatment What does this mean for your patients? US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General; 2004.
 Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Pyramid for Osteoporosis Prevention and Treatment. What does this mean for your patients US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General;")
45
“Pharmacotherapy” (Medications)
")
46
Medications Prevent and Treat Thresholds
1. The Fracture Patient or < or = -2.5 T score 2. Bone density = or < - 2.0 3. Bone density = or < with risk factors Guidelines for post menopausal women And men over 50

47
2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary Alexandra Papaioannou MD MSc, Suzanne Morin MD MSc, Angela M. Cheung MD PhD, Stephanie Atkinson PhD, Jacques P. Brown MD, Sidney Feldman MD, David A. Hanley MD, Anthony Hodsman MD, Sophie A. Jamal MD PhD, Stephanie M. Kaiser MD, Brent Kvern MD, Kerry Siminoski MD, William D. Leslie MD MSc; for the Scientific Advisory Council of Osteoporosis Canada

48
2008 NOF Clinician’s Guide & FRAX
48

49
NOF 2008 Guidelines Who Should Be Treated?
Fragility fracture- hip or spine T-score ≤ -2.5 T-score -1.0 to -2.5 (osteopenia) and 10-year all major osteoporosis-related fracture probability of ≥ 20% or a 10-year hip fracture probability ≥ 3% (FRAX)
 and. 10-year all major osteoporosis-related fracture probability of ≥ 20% or a. 10-year hip fracture probability ≥ 3% (FRAX)")
50
Kanis Osteoporos Int 2008;19:385-397
WHO Risk Factors Age (50-90), gender and clinical risk factors: BMI Prior fragility fracture Parental history of hip fracture Current tobacco smoking Ever long-term use of glucocorticoids Rheumatoid arthritis or other secondary causes Alcohol intake 3 or more units daily Kanis Osteoporos Int 2008;19: 50
, gender and clinical risk factors: BMI. Prior fragility fracture. Parental history of hip fracture. Current tobacco smoking. Ever long-term use of glucocorticoids. Rheumatoid arthritis or other secondary causes. Alcohol intake 3 or more units daily. Kanis Osteoporos Int 2008;19:")
51
(>1 million person years)
Fracture probability calculated from 12 world-wide cohorts (59,232 individuals, 250K person-years), validated in 11 independent cohorts (>1 million person years) 51
, validated in 11 independent cohorts. (>1 million person years) 51.")
53
Advantages of 2008 Guidelines
Includes men and other ethnic groups Guides treatment decisions in the osteopenic patient where most fractures occur FRAX Utilizes absolute fracture risk assessment

54
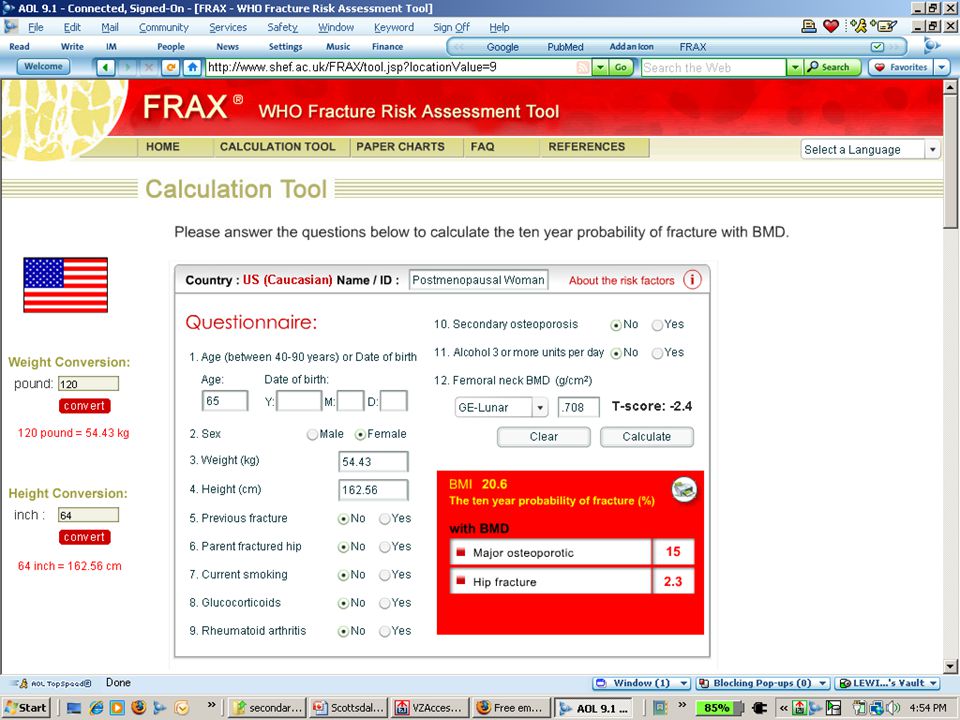
CASES 1 and 2 75 y/o caucasian female, h/o hip fracture- father
T-score femoral neck = -2.4 spine +1.1 FRAX- 10 year fracture probability = 30% & 20% 52 y/o 1 yr postmenopausal, h/o hip fracture- mother spine L1-L4 = -1.0 FRAX- 10 year fracture probability = 14% & 1.5%

55
CASES 3 and 4 75 y/o caucasian female, h/o hip fracture in father
T-score femoral neck = -1.7 spine +1.1 FRAX- 10 year fracture probability = 20% & 11% 63 y/o, h/o hip fracture & 3 spine fractures in mother T-score femoral neck = -2.3 spine L1-L4 = -2.4 FRAX- 10 year fracture probability = 19% & 1.8%

56
CASE 5 86 y/o caucasian female, h/o proximal humerus fx, sacral fx, distal radius fx with minor falls T-score femoral neck = -0.4 spine doesn’t matter unless < -2.5 FRAX- 10 year fracture probability = 14% & 2.5%

57
FRAX Benefits BMD + CRFs predict fracture risk better than BMD or CRFs alone Can be used without BMD when DXA is not available Quantitative assessment of fracture risk Can be used with cost-utility analysis

58
FRAX Limitations Does not apply to premenopausal patients
Does not apply to treated patients Does not include all risk factors Important risk factors not considered (falls, BTMs, rare diseases, etc.) Yes or No response to CRFs does not consider range of risk May underestimate or overestimate fracture risk Does not quantify risk factors; ie: 3 personal pelvis fractures = 1 ankle fracture 5 mg prednisone for 3 months 2 years ago = mg prednisone daily now BMD input limited to femoral neck Cannot use BMD of the spine .... or forearm 58 58
 Yes or No response to CRFs does not consider range of risk. May underestimate or overestimate fracture risk. Does not quantify risk factors; ie: 3 personal pelvis fractures = 1 ankle fracture. 5 mg prednisone for 3 months 2 years ago = 60 mg prednisone daily now. BMD input limited to femoral neck. Cannot use BMD of the spine .... or forearm")
59
Surgeon General’s Report on Bone Health and Osteoporosis
Leading the Effort to Help Prevent and Treat Osteoporosis Pharmacotherapy (antiresorptives and anabolics) Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Surgeon General’s Report on Bone Health and Osteoporosis Pyramid for Osteoporosis Prevention and Treatment What does this mean for your patients? US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General; 2004.
 Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Surgeon General’s Report on Bone Health and Osteoporosis. Pyramid for Osteoporosis Prevention and Treatment. What does this mean for your patients US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General;")
61
Anti-Resorptives (Anti-Catabolics)
Bisphosphonates Estrogens SERMs Raloxifene (Evista) Calcitonin (Miacalcin, Fortical, Calcimar)
 Calcitonin. (Miacalcin, Fortical, Calcimar)")
62
Anti-Resorptives (Anti-Catabolics)
Bisphosphonates Estrogens SERMs Raloxifene (Evista) Calcitonin (Miacalcin, Fortical, Calcimar)
 Calcitonin. (Miacalcin, Fortical, Calcimar)")
63
Bisphosphonates Approved for Treating Postmenopausal Osteoporosis
Fosamax Plus D (alendronate sodium/ cholecalciferol) Tablets and Fosamax (alendronate sodium) Tablets INDICATION Increases BMD Reduces incidence of hip and spine fractures GENERIC Alendronate Actonel and calcium the other six days (risedronate sodium tablets/calcium 500mg ) Actonel (risedronate sodium) INDICATION Reduces incidence of vertebral fracture and a composite end point of nonvertebral fracture Boniva (ibandronate sodium) tablets Boniva IV infusion Reduces incidence of vertebral fracture Reclast IV 5 mg/year DOSING & 10 mg daily Fosamax plus D 70 mg/2800 IU once weekly 70 mg/5600 IU once weekly Fosamax 35 mg once weekly or 5mg/day 70 mg once weekly or 10 mg/day Fosamax Liquid 70 mg bottle once weekly DOSING Actonel 5 mg/day or 35 mg once weekly Or with Calcium 75mg 2 days/month 150mgonce a month ADMINISTRATION Take at least 30 min before first food of the day. Do not lie down for at least 30 min after dosing. Boniva 2.5 mg/day or 150 mg once monthly ADMINISTRATION Take at least 60 min before first food of the day. Do not lie down for at least 60 min after dosing. Boniva 3 mg IV every 3 mos Bisphosphonates Approved for Treating Postmenopausal Osteoporosis There are at least 7 bisphosphonate products commercially available in the US, but only 4 are currently indicated for the treatment of postmenopausal osteoporosis. The other 3— pamidronate, etidronate, and tiludronate—are primarily indicated for Paget’s disease of bone. Bisphosphonates currently approved for the treatment of postmenopausal osteoporosis include risedronate sodium, which is marketed as Actonel by Proctor and Gamble and Sanofi-Aventis; ibandronate, marketed as Boniva by Roche and GlaxoSmithKline; alendronate sodium/cholecalciferol, marketed as FOSAMAX PLUS D by Merck & Co., Inc.; and alendronate, marketed as FOSAMAX by Merck & Co., Inc. The recommended dosing regimen of alendronate for osteoporosis treatment is 70 mg once weekly or 10 mg/day. The recommended dosing regimen of alendronate plus cholecalciferol for osteoporosis treatment is one tablet containing 70 mg alendronate and 2,800 IU vitamin D once weekly. The recommended regimen of risedronate for treatment is 35 mg once weekly or 5 mg/day. The recommended regimen of ibandronate for treatment is 2.5 mg/day or 150 mg once monthly.1 Well-designed, placebo-controlled trials have established the efficacy of these drugs in the treatment of postmenopausal osteoporosis. However, alendronate has an indication to reduce the risk of vertebral and hip fracture. Risedronate is indicated to reduce the risk of vertebral fracture and a composite end point of nonvertebral fracture. Ibandronate is indicated for the treatment and prevention of osteoporosis in postmenopausal women and is indicated to reduce the risk of vertebral fracture. The pivotal trials supporting the indications in the ibandronate package insert looked for but failed to find a significant difference between ibandronate and placebo in nonvertebral fracture rates, including the hip.2 According to the prescribing information for ibandronate, at 3 years with 2.5 mg daily, the proportion of ibandronate-treated patients with nonvertebral fractures was 9.1% (95% confidence interval [CI]: 7.1%–11.1%) vs 8.2% among placebo-treated patients (95% CI: 6.3%–10.2%).2 Ibandronate produced statistically significant 3-year increases in BMD at the lumbar spine (6.4% vs 1.4%) and hip (3.1% vs –0.7%), compared with placebo.2 It should also be noted that, compared with alendronate and risedronate, ibandronate administration requires twice the waiting time before breakfast (60 minutes vs 30 minutes), and the patient must remain standing or sit upright twice as long (60 minutes vs 30 minutes).2,3 References: 1. US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, Md: US Dept of Health and Human Services, Office of the Surgeon General; 2004. 2. Boniva (ibandronate sodium) Tablets, Full Prescribing Information (NDA21-455). Available at: Accessed on March 31, 2005. 3. Actonel [package insert]. Cincinnati, Ohio: Procter & Gamble Pharmaceuticals; 2003.
 Tablets. and. Fosamax (alendronate sodium) Tablets INDICATION. Increases BMD. Reduces incidence of hip and spine fractures. GENERIC Alendronate. Actonel and calcium the other six days. (risedronate sodium tablets/calcium 500mg ) Actonel (risedronate sodium) INDICATION. Reduces incidence of vertebral fracture and a composite end point of nonvertebral fracture. Boniva. (ibandronate sodium) tablets. Boniva IV infusion. Reduces incidence of vertebral fracture. Reclast IV 5 mg/year. DOSING 5 & 10 mg daily. Fosamax plus D. 70 mg/2800 IU once weekly. 70 mg/5600 IU once weekly Fosamax. 35 mg once weekly or 5mg/day. 70 mg once weekly or 10 mg/day Fosamax Liquid. 70 mg bottle once weekly. DOSING. Actonel 5 mg/day or 35 mg once weekly. Or with Calcium. 75mg 2 days/month. 150mgonce a month ADMINISTRATION. Take at least 30 min before first food of the day. Do not lie down for at least 30 min after dosing. Boniva 2.5 mg/day or. 150 mg once monthly. ADMINISTRATION. Take at least 60 min before first food of the day. Do not lie down for at least 60 min after dosing. Boniva 3 mg IV every 3 mos. Bisphosphonates Approved for Treating Postmenopausal Osteoporosis. There are at least 7 bisphosphonate products commercially available in the US, but only 4. are currently indicated for the treatment of postmenopausal osteoporosis. The other 3— pamidronate, etidronate, and tiludronate—are primarily indicated for Paget’s disease of bone. Bisphosphonates currently approved for the treatment of postmenopausal osteoporosis include risedronate sodium, which is marketed as Actonel by Proctor and Gamble and Sanofi-Aventis; ibandronate, marketed as Boniva by Roche and GlaxoSmithKline; alendronate sodium/cholecalciferol, marketed as FOSAMAX PLUS D by Merck & Co., Inc.; and alendronate, marketed as FOSAMAX by Merck & Co., Inc. The recommended dosing regimen of alendronate for osteoporosis treatment is 70 mg once weekly or 10 mg/day. The recommended dosing regimen of alendronate plus cholecalciferol for osteoporosis treatment is one tablet containing 70 mg alendronate and 2,800 IU vitamin D once weekly. The recommended regimen of risedronate for treatment is 35 mg once weekly or 5 mg/day. The recommended regimen of ibandronate for treatment is 2.5 mg/day or 150 mg once monthly.1. Well-designed, placebo-controlled trials have established the efficacy of these drugs in the treatment of postmenopausal osteoporosis. However, alendronate has an indication to reduce the risk of vertebral and hip fracture. Risedronate is indicated to reduce the risk of vertebral fracture and a composite end point of nonvertebral fracture. Ibandronate is indicated for the treatment and prevention of osteoporosis in postmenopausal women and is indicated to reduce the risk of vertebral fracture. The pivotal trials supporting the indications in the ibandronate package insert looked for but failed to find a significant difference between ibandronate and placebo in nonvertebral fracture rates, including the hip.2. According to the prescribing information for ibandronate, at 3 years with 2.5 mg daily, the proportion of ibandronate-treated patients with nonvertebral fractures was 9.1% (95% confidence interval [CI]: 7.1%–11.1%) vs 8.2% among placebo-treated patients (95% CI: 6.3%–10.2%).2. Ibandronate produced statistically significant 3-year increases in BMD at the lumbar spine (6.4% vs 1.4%) and hip (3.1% vs –0.7%), compared with placebo.2. It should also be noted that, compared with alendronate and risedronate, ibandronate administration requires twice the waiting time before breakfast (60 minutes vs 30 minutes), and the patient must remain standing or sit upright twice as long (60 minutes vs 30 minutes).2,3. References: 1. US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon. General. Rockville, Md: US Dept of Health and Human Services, Office of the Surgeon General; Boniva (ibandronate sodium) Tablets, Full Prescribing Information (NDA21-455). Available at: Accessed on March 31, Actonel [package insert]. Cincinnati, Ohio: Procter & Gamble Pharmaceuticals;")
64
Fosamax (alendronate)
Cuts fracture risk by ~50% Formulations: 5mg, 10mg, 35mg, 70mg 70mg IU D, 70mg IU D 70mg Liquid GENERIC alendronate 70mg weekly

65
Actonel (risedronate)
Cuts fracture risk ~50% Formulations: 5mg, 35mg, 35mg + 6 day calcium packet 75mg two consecutive days monthly 150mg once monthly

66
Boniva (ibandronate) Cuts fracture risk ~50% Formulations:
2.5mg, 150mg PO monthly IV 3mg q 3 months

67
August 17th 2007 New ? Antiresorptive Therapies
Zoledronate (Aclasta)- 5 mg IV annually
- 5 mg IV annually.")
68
Zoledronate (Reclast) 5 mg IV annually
Will this change the way we view pharmacological treatment of osteoporosis? It has.

69
HORIZON Pivotal Fracture Trial: Effect on Vertebral Fractures
Slide ID: 18509 HORIZON Pivotal Fracture Trial: Effect on Vertebral Fractures The figure shows that over 3 years, treatment with Reclast 5 mg significantly reduced the incidence of new vertebral fractures in the study group Reclast significantly decreased the incidence of new vertebral fractures over 1, 2, and 3 years Reclast significantly decreased the risk of at least one new moderate or severe vertebral fracture at 1 year (60%), 2 years (71%) and 3 years (70%) (all P < .0001) The reductions in vertebral fractures over 3 years were consistent (including new/worsening and multiple vertebral fractures) and significantly greater than placebo regardless of age, geographical region, baseline body mass index, number of baseline vertebral fractures, femoral neck BMD T-score, or prior bisphosphonate usage
, 2 years (71%) and 3 years (70%) (all P < .0001) The reductions in vertebral fractures over 3 years were consistent (including new/worsening and multiple vertebral fractures) and significantly greater than placebo regardless of age, geographical region, baseline body mass index, number of baseline vertebral fractures, femoral neck BMD T-score, or prior bisphosphonate usage.")
70
HORIZON Pivotal Fracture Trial: Effect on Hip Fractures Over 3 Years
Slide ID: 18510 HORIZON Pivotal Fracture Trial: Effect on Hip Fractures Over 3 Years This figure depicts the cumulative incidence of hip fractures over the 3-year study period. As seen in the graph, treatment with Reclast significantly reduced the risk of fracture Reclast demonstrated a 1.1% absolute reduction and 41% relative reduction in the risk of hip fractures over a median duration of follow-up of 3 years The hip fracture event rate was 1.4% for Reclast-treated patients compared to 2.5% for placebo-treated patients In patients who did not take concomitant osteoporosis therapy, Reclast demonstrated a 41% reduction in the risk of hip fractures over this time period The reductions in hip fractures over 3 years were greater for Reclast than placebo regardless of femoral neck BMD T-score

71
HORIZON Pivotal Fracture Trial: Effects on All Clinical Fractures Over 3 Years
Slide ID: 18511 HORIZON Pivotal Fracture Trial: Effects on All Clinical Fractures Over 3 Years Reclast demonstrated superiority to placebo in reducing the incidence of all clinical fractures, clinical (symptomatic) vertebral, and non-vertebral fractures (excluding finger, toe, facial, and clinical thoracic and lumber vertebral fractures) All clinical fractures were verified based on the radiographic and/or clinical evidence
 vertebral, and non-vertebral fractures (excluding finger, toe, facial, and clinical thoracic and lumber vertebral fractures) All clinical fractures were verified based on the radiographic and/or clinical evidence.")
72
HORIZON Pivotal Fracture Trial: Effect on Bone Mineral Density (BMD)
Slide ID: 18512 HORIZON Pivotal Fracture Trial: Effect on Bone Mineral Density (BMD) Reclast significantly increased BMD at the lumbar spine, total hip, and femoral neck, relative to treatment with placebo at time points 12, 24, and 36 months Treatment with Reclast resulted in a 6.7% increase in BMD at the lumbar spine, 6.0% at the total hip, and 5.1% at the femoral neck, over 3 years as compared to placebo
 Reclast significantly increased BMD at the lumbar spine, total hip, and femoral neck, relative to treatment with placebo at time points 12, 24, and 36 months. Treatment with Reclast resulted in a 6.7% increase in BMD at the lumbar spine, 6.0% at the total hip, and 5.1% at the femoral neck, over 3 years as compared to placebo.")
73
Zoledronate (Reclast) 5 mg IV annually
Given within 90 days of Hip Fracture with a D3 load, and FU Calcium and D Increase BMD FN and TH Reduction Spine & non spine fractures 35% Mortality 28% Lyles NEJM : 73

74
Zoledronate (Aclasta) 5 mg IV annually
Approved for Use in Men Approved for GIO 2009 Approved for Prevention 2009 (2 year dosing regimen) 74
 74.")
75
Bisphosphonates Adverse events GI (same as placebo in studies)
Flu-like “Acute Phase Reaction” Bone pain Hypocalcemia Iritis/Uveitis ONJ Unusual subtrochanteric fractures 75

76
Comparative Risks (1) Women age (from Swedish National Bureau of Statistics and database of Olmsted County, MN, USA.) Kanis JA et al. Osteoporos Int. 2001;12: Pharmcoepidemiol Drug Saf. 2003;12: National Center for Health Statistics. JADA. 2006;137:

77
Comparative Risks Data so far
Subtrochanteric fractures comprise 2-4% of all “Hip Fractures” (fairly uncommon) “Unusual or atypical Subtroch femur fractures” Bisphosphonate associated fractures comprise 1/3 of those- criteria are: Thigh pain prodrome, “pseudo-fracture appearance”, lateral “beaking”, transverse fracture pattern
 Unusual or atypical Subtroch femur fractures Bisphosphonate associated fractures comprise 1/3 of those- criteria are: Thigh pain prodrome, pseudo-fracture appearance , lateral beaking , transverse fracture pattern.")
78
Trabecular Bone Showed No Qualitative or Quantitative Abnormalities in FLEX*
Alendronate/Placebo Group: Average bone volume fraction, 16.5% Alendronate/Alendronate Group: Average bone volume fraction, 16.6% Trabecular Bone Showed No Qualitative or Quantitative Abnormalities in FLEX Representative 3-dimensional samples from alendronate/placebo and alendronate/alendronate specimens, after 10 years of follow-up, are shown in this slide, which depicts an on-edge view. Trabecular bone shows no qualitative or quantitative abnormalities. Six samples, which had an average bone volume fraction of 16.5%, were analyzed from the alendronate/placebo group; 8 samples, which had an average bone volume fraction of 16.6%, were analyzed from the alendronate/alendronate group.1 In FLEX, after 5 years of alendronate treatment (alendronate/placebo group) or 10 years of alendronate treatment (alendronate/alendronate group), biopsy results showed that trabecular bone tissue from both groups appeared normal. The on-edge view is shown above. Two other views are available, en face and oblique. As for the on-edge view, there were no differences in bone quality between the alendronate/placebo or alendronate/alendronate treatment groups for the en face or oblique views. There were no abnormalities such as woven bone, osteitis fibrosa, defective mineralization, and nonlamellar bone.1,2 References: 1. Recker R, Ensrud K, Diem S, et al. Normal bone histomorphometry and 3D microachitecture after 10 years alendronate treatment of postmenopausal women. J Bone Miner Res. 2004;19(suppl 1):S45. 2. Data available on request from Merck & Co., Inc., Professional Services-DAP, WP1-27, PO Box 4, West Point, PA Please specify information package (1)–FOS. * On-edge view is depicted. 1. Recker R et al. J Bone Miner Res. 2004;19(suppl 1):S Data available on request from Merck & Co., Inc. Please specify (1)–FOS.
 or 10 years of alendronate treatment (alendronate/alendronate group), biopsy results showed that trabecular bone tissue from both groups appeared normal. The on-edge view is shown above. Two other views are available, en face and oblique. As for the on-edge view, there were no differences in bone quality between the alendronate/placebo or alendronate/alendronate treatment groups for the en face or oblique views. There were no abnormalities such as woven bone, osteitis fibrosa, defective mineralization, and nonlamellar bone.1,2. References: 1. Recker R, Ensrud K, Diem S, et al. Normal bone histomorphometry and 3D microachitecture after 10 years alendronate treatment of postmenopausal women. J Bone Miner Res. 2004;19(suppl 1):S Data available on request from Merck & Co., Inc., Professional Services-DAP, WP1-27, PO Box 4, West Point, PA Please specify information package (1)–FOS. * On-edge view is depicted. 1. Recker R et al. J Bone Miner Res. 2004;19(suppl 1):S Data available on request from Merck & Co., Inc. Please specify (1)–FOS.")
79
Alendronate Improved Cortical Thickness in Hip
Placebo Alendronate *,† 5 4 *,† *,† 3 2 Change, % Alendronate Improves Cortical Thickness Alendronate significantly improves cortical thickness. Changes in structural geometry of the hip were evaluated in 373 postmenopausal women receiving hormone replacement therapy (n = 93), alendronate (n = 93), combination therapy (n = 94) or placebo (n = 93) for 3 years. BMD measurement of the hip by dual energy x-ray absorptiometry (DXA) scanning at baseline and at 3 years was used to derive hip structural geometry data using the hip structural analysis (HSA) program. The HSA program uses conventional DXA mineral mass and dimensional data to determine structural dimensions corresponding to the narrow neck, the intertrochanteric region, and the femoral shaft. Measured parameters included cortical thickness, bone cross-sectional area, section modulus, buckling ratio, and HSA BMD.1 Cortical thickness data for the narrow neck, trochanteric, and femoral shaft regions from the placebo and alendronate groups are shown above. After 3 years, alendronate 10 mg/day significantly improved cortical thickness compared with baseline and placebo (P<0.05 for both comparisons).1 These findings suggest that treatment with alendronate 10 mg had positive effects on cortical thickness. Although not shown above, treatment with alendronate also was associated with improved cross-sectional area, section modulus, buckling ratio, and HSA BMD compared with baseline and placebo in the narrow neck, intertrochanteric, and femoral shaft regions. Improvements were significant vs placebo and/or baseline (P<0.05). Reference: 1. Greenspan SL, Beck TJ, Resnick NM, Bhattacharya R, Parker, RA. Effect of hormone replacement, alendronate, or combination therapy on hip structural geometry: a 3-year, double-blind, placebo-controlled clinical trial. J Bone Miner Res. 2005;20:1525–1532. 1 –1 –2 –3 Narrow Neck Intertrochanteric Femoral Shaft Region Region Region *P<0.05 vs baseline; †P<0.05 vs placebo. Greenspan SL et al. J Bone Miner Res. 2005;20:1525–1532.
, alendronate (n = 93), combination therapy (n = 94) or placebo (n = 93) for 3 years. BMD measurement of the hip by dual energy x-ray absorptiometry (DXA) scanning at baseline and at 3 years was used to derive hip structural geometry data using the hip structural analysis (HSA) program. The HSA program uses conventional DXA mineral mass and dimensional data to determine structural dimensions corresponding to the narrow neck, the intertrochanteric region, and the femoral shaft. Measured parameters included cortical thickness, bone cross-sectional area, section modulus, buckling ratio, and HSA BMD.1. Cortical thickness data for the narrow neck, trochanteric, and femoral shaft regions from the placebo and alendronate groups are shown above. After 3 years, alendronate 10 mg/day significantly improved cortical thickness compared with baseline and placebo (P<0.05 for both comparisons).1. These findings suggest that treatment with alendronate 10 mg had positive effects on cortical thickness. Although not shown above, treatment with alendronate also was associated with improved cross-sectional area, section modulus, buckling ratio, and HSA BMD compared with baseline and placebo in the narrow neck, intertrochanteric, and femoral shaft regions. Improvements were significant vs placebo and/or baseline (P<0.05). Reference: 1. Greenspan SL, Beck TJ, Resnick NM, Bhattacharya R, Parker, RA. Effect of hormone replacement, alendronate, or. combination therapy on hip structural geometry: a 3-year, double-blind, placebo-controlled clinical trial. J Bone Miner. Res. 2005;20:1525– –1. –2. –3. Narrow Neck. Intertrochanteric. Femoral Shaft. Region. Region. Region. *P<0.05 vs baseline; †P<0.05 vs placebo. Greenspan SL et al. J Bone Miner Res. 2005;20:1525–1532.")
80
Current Thought Long term continuation: > 5 years
+ Reduction in clinical vertebral fracture with long-term ALN (10 years) Suggests most benefit from continuing ALN in those at high risk of new vertebral fracture Others might be discontinued No clinical evidence for compromise in bone quality with long-term treatment (any bisphosphonates) Little guidance for long term continuation of bisphosphonates other than ALN (6 year trial of ZOL coming—study end 12/09) Black 2010
 Suggests most benefit from continuing ALN in those at high risk of new vertebral fracture Others might be discontinued. No clinical evidence for compromise in bone quality with. long-term treatment (any bisphosphonates) Little guidance for long term continuation of bisphosphonates other than ALN. (6 year trial of ZOL coming—study end 12/09) Black")
81
Current Thought Continuing ALN for 10 years instead of stopping after 5 years Reduces NVF risk in women even without prevalent vertebral fracture, whose FN T-scores, achieved after 5 years of ALN, are < or = -2.5 But does not reduce risk of NVF in women whose T-scores are > -2. Schwartz JBMR

82
Current Thought 5 year plan 10 year plan

83
Anabolic Therapy Action on the Osteoblast rather than the Osteoclast

84
Forteo Teriparitide (PTH 1-34)
The only anabolic agent for osteoporosis Acts on the osteoblast Given SubQ daily Approved November 2002 Indications- severe osteoporosis, GIO, men Given for months Followed with an antiresorptive agent

85
New Vertebral Fracture
FORTEO® (teriparatide [rDNA origin] injection) Reduces the Risk of 1 New Vertebral Fractures Relative Risk 0.35 95% CI, 0.22 to 0.551 16 14 64 Risk Reduction Relative: 65%* Absolute: 9.3%* 12 10 New Vertebral Fracture % of Women With 8 6 4 22 2 Placebo (n=448) FORTEO (n=444) *p <.001 1. N Engl J Med. 2001;344: See Black Box Warning (slide 32) and Important Safety Information for FORTEO (slides 1, 16, 34-36). Full Prescribing Information for FORTEO is available at this presentation.
 Reduces the Risk of 1 New Vertebral Fractures. Relative Risk % CI, 0.22 to Risk Reduction. Relative: 65%* Absolute: 9.3%* New Vertebral Fracture. % of Women With Placebo. (n=448) FORTEO. (n=444) *p < N Engl J Med. 2001;344: See Black Box Warning (slide 32) and Important Safety Information for FORTEO (slides 1, 16, 34-36). Full Prescribing Information for FORTEO is available at this presentation.")
86
FORTEO® (teriparatide [rDNA origin] injection) Increased Lumbar Spine BMD in Postmenopausal Women With Osteoporosis*,1 FORTEO (N=129) 2 4 6 8 10 12 14 Placebo (N=137) BMD (Mean % Change ± SE) *266 subjects treated for 18 months and with data available at all time points †p<0.001 for FORTEO vs. placebo at each post-baseline time point 11.8%† 6.9%† 9.4%† 3.9%† 3 6 9 12 15 18 Months since randomization 1. Data on file, Lilly Research Laboratories. See Black Box Warning (slide 32) and Important Safety Information for FORTEO (slides 1, 16, 34-36). Full Prescribing Information for FORTEO is available at this presentation.
![FORTEO® (teriparatide [rDNA origin] injection) Increased Lumbar Spine BMD in Postmenopausal Women With Osteoporosis*,1](http://slideplayer.com/slide/5739834/19/images/86/FORTEO%C2%AE+%28teriparatide+%5BrDNA+origin%5D+injection%29+Increased+Lumbar+Spine+BMD+in+Postmenopausal+Women+With+Osteoporosis%2A%2C1.jpg "FORTEO (N=129) Placebo (N=137) BMD (Mean % Change ± SE) *266 subjects treated for 18 months and with data available at all time points †p<0.001 for FORTEO vs. placebo at each post-baseline time point. 11.8%† 6.9%† 9.4%† 3.9%† Months since randomization. 1. Data on file, Lilly Research Laboratories. See Black Box Warning (slide 32) and Important Safety Information for FORTEO (slides 1, 16, 34-36). Full Prescribing Information for FORTEO is available at this presentation.")
87
Teriparatide Adverse events Osteosarcoma in rats
Hypercalcemia 11% vs 1% Dizziness 2.6% vs 1.4% Leg cramps 2.6% vs 1.3%

88
FDA Indications for Osteoporosis
Drug PMO GIO (Women, Men) Men Prevention Treatment Estrogen Alendronate PO (Fosamax®) Risedronate PO (Actonel®) Ibandronate PO (Boniva®) Ibandronate IV (Boniva®) Zoledronate IV (Reclast®) Calcitonin IN (Miacalcin®, Fortical®) Raloxifene PO (Evista®) Teriparatide SC (Forteo®) Paget’s dose: Fosamax 40 mg/day x 6 mo., Actonel 30 mg/day x 2 mo. Launch Dates: Fosamax 10/95, Miacalcin 1/96, Evista 1/98, Actonel 5/00, Weekly Fosamax 11/00 88
 Men. Prevention. Treatment. Estrogen. Alendronate PO (Fosamax®) Risedronate PO (Actonel®) Ibandronate PO (Boniva®) Ibandronate IV (Boniva®) Zoledronate IV (Reclast®) Calcitonin IN (Miacalcin®, Fortical®) Raloxifene PO (Evista®) Teriparatide SC (Forteo®) Paget’s dose: Fosamax 40 mg/day x 6 mo., Actonel 30 mg/day x 2 mo. Launch Dates: Fosamax 10/95, Miacalcin 1/96, Evista 1/98, Actonel 5/00, Weekly Fosamax 11/")
89
BMD Response to Therapy
Medication Spine Hip Estrogen Alendronate (Fosamax®) Risedronate (Actonel®) Ibandronate (Boniva®) Zoledronate (Reclast®) Salmon Calcitonin (Miacalcin®, Fortical®) - Raloxifene (Evista®) Teriparatide (Forteo®)
 Risedronate (Actonel®) Ibandronate (Boniva®) Zoledronate (Reclast®) Salmon Calcitonin. (Miacalcin®, Fortical®) - Raloxifene (Evista®) Teriparatide (Forteo®)")
90
Fracture Risk Reduction in RCTs
Medication Spine Nonvertebral Hip Estrogen Alendronate (Fosamax®) Risedronate (Actonel®) Ibandronate (Boniva®) Zoledronate (Reclast®) Calcitonin (Miacalcin®, Fortical®) Raloxifene (Evista®) Teriparatide (Forteo®)
 Risedronate (Actonel®) Ibandronate (Boniva®) Zoledronate (Reclast®) Calcitonin. (Miacalcin®, Fortical®) Raloxifene (Evista®) Teriparatide (Forteo®)")
91
New and Emerging Treatments
Antiresorptive (anti-catabolic) Denosumab (Prolia) Odanacatib Lasofoxifene Bazedoxifene CE/bazedoxifene New delivery systems - oral salmon calcitonin Osteo-anabolic (bone-forming) Sclerostin inhibitor Variations of PTH Endogenous PTH stimulation - calcium sensing receptor antagonist (calcilytic) New delivery systems – transdermal PTH Strontium ranelate Combinations of antiresorptive and anabolic
 Denosumab (Prolia) Odanacatib. Lasofoxifene. Bazedoxifene. CE/bazedoxifene. New delivery systems - oral salmon calcitonin. Osteo-anabolic (bone-forming) Sclerostin inhibitor. Variations of PTH. Endogenous PTH stimulation - calcium sensing receptor antagonist (calcilytic) New delivery systems – transdermal PTH. Strontium ranelate Combinations of antiresorptive and anabolic.")
92
Denosumab (Prolia) (Anti-resorptive agent)
Approved June 1, 2010 Made by Amgen A fully human monoclonal antibody that binds with high affinity to, and inhibits the activity of, human RANK ligand, a key mediator of osteoclast activity

93
RANKL is Implicated in Bone Loss Across a Broad Range of Conditions
Postmenopausal osteoporosis Male osteoporosis Disuse osteoporosis Transplantation osteoporosis Inflammatory arthritis Periprosthetic osteolysis Hyperparathyroidism Cancer-induced bone loss Bone metastases, multiple myeloma Treatment-induced bone loss Glucocorticoids, aromatase inhibitors, androgen deprivation therapy Unopposed RANK Ligand (i.e., an elevated RANK Ligand/OPG ratio) has been implicated in bone destruction across the spectrum of bone loss pathology. The effects of RANK Ligand are physiologically counterbalanced by the soluble receptor OPG. Estrogen deficiency, glucocorticoid exposure, T cell activation (e.g., rheumatoid arthritis), and skeletal malignancies (e.g., myeloma, metastases) enhance the ratio of RANK Ligand to OPG and, thus, promote osteoclastogenesis, accelerate bone resorption, and induce bone loss.1-2 Hofbauer LC, et al. Clinical Implications of the Osteoprotegerin/RANKL/RANK System for Bone and Vascular Diseases. JAMA. 2004;292:490-5. Boyle WJ, et al. Osteoclast Differentiation and Activation. Nature. 2003;423: 93
 has been implicated in bone destruction across the spectrum of bone loss pathology. The effects of RANK Ligand are physiologically counterbalanced by the soluble receptor OPG. Estrogen deficiency, glucocorticoid exposure, T cell activation (e.g., rheumatoid arthritis), and skeletal malignancies (e.g., myeloma, metastases) enhance the ratio of RANK Ligand to OPG and, thus, promote osteoclastogenesis, accelerate bone resorption, and induce bone loss.1-2. Hofbauer LC, et al. Clinical Implications of the Osteoprotegerin/RANKL/RANK System for Bone and Vascular Diseases. JAMA. 2004;292: Boyle WJ, et al. Osteoclast Differentiation and Activation. Nature. 2003;423:")
94
RANKL Stimulates Bone Resorption
RANK Ligand Is Essential for Osteoclast Formation, Function, and Survival RANKL CFU-M RANK Pre-Fusion Osteoclast Growth Factors Hormones Cytokines Multinucleated Osteoclast Receptor Activator of Nuclear Factor-kappa B (RANK) Ligand is essential for osteoclast formation, function, and survival.1-5 In the presence of low levels of macrophage colony-stimulating factor (M-CSF), RANK Ligand is essential for osteoclast formation, function, and survival.1-5 Osteoclasts are the cells responsible for resorbing bone. Many different factors (e.g., PTH, TNF, IL-1) can lead to bone loss. These stimulate the expression of RANK Ligand by cells of the osteoblast lineage and other cells (e.g., activated T cells).2,5 The RANK Ligand polypeptide is a type II transmembrane protein found on the surface of expressing cells as well as in a proteolytically released (cleaved) soluble form.3 RANK Ligand is expressed (both in a transmembrane and soluble form) from the osteoblast lineage cells.4 In addition, RANK Ligand is expressed in various cell types including, but not limited to: lymphoid cells,6 basal epithelial, luminal epithelial and stromal cells from normal prostate7 and non-malignant breast tissue,8 including mammary epithelial cells,9 tumor cells including breast cancer cells,8 prostate cancer cells and subsequent bone metastases;7 dendritic cells, activated T-cells and B-cells,10 osteoblasts5 and osteoclasts, mesenchymal cells, proliferative chondrocytes, early osteocytes and periosteal cells; synovial tissue,11 cardiomyocytes, vascular smooth muscle cells, endothelial cells,12 and the GI tract.13 The clinical significance of these findings is unknown. RANK Ligand subsequently binds to its receptor, RANK, on immature and mature osteoclasts, which leads to maturation of pre-fusion osteoclasts to multinucleated osteoclasts and finally to activated osteoclasts.5 RANK is expressed on osteoclasts and osteoclast progenitors. In addition, RANK has been observed on cartilage cells (chondrocytes), mammary gland epithelial cells, and trophoblast cells.5,6,7 1. Yasuda H, et al. Proc Natl Acad Sci USA. 1998;95: 2. Fuller K, et al. J Exp Med. 1998;188: 3. Lacey DL, et al. Cell. 1998;93: 4. Lacey DL, et al. Am J Pathol. 2000;157: 5. Boyle WJ, et al. Nature. 2003;423: 6. Kong Y-Y, et al. Nature. 1999;397: 7. Brown JM, et al. Urology. 2001;57: 8. Van Poznak C, et al. J Clin Pathol. 2006;59:56-63. 9. Fata JE, et al. Cell :103:41-50. 10. Anderson DM, et al. Nature. 1997;390: 11. Crotti TN, et al. Ann Rheum Dis. 2002;61: 12. Ueland T, et al. Circulation. 2005;111: 13. Moschen AR, et al. Gut. 2005;54: 14. Hsu H, et al. Proc Natl Acad Sci USA. 1999:96: Activated Osteoclast Osteoblast Lineage CFU-M = colony forming unit macrophage Bone Adapted from Boyle WJ, et al. Nature. 2003;423: 94
 Ligand is essential for osteoclast formation, function, and survival.1-5. In the presence of low levels of macrophage colony-stimulating factor (M-CSF), RANK Ligand is essential for osteoclast formation, function, and survival.1-5. Osteoclasts are the cells responsible for resorbing bone. Many different factors (e.g., PTH, TNF, IL-1) can lead to bone loss. These stimulate the expression of RANK Ligand by cells of the osteoblast lineage and other cells (e.g., activated T cells).2,5. The RANK Ligand polypeptide is a type II transmembrane protein found on the surface of expressing cells as well as in a proteolytically released (cleaved) soluble form.3. RANK Ligand is expressed (both in a transmembrane and soluble form) from the osteoblast lineage cells.4. In addition, RANK Ligand is expressed in various cell types including, but not limited to: lymphoid cells,6 basal epithelial, luminal epithelial and stromal cells from normal prostate7 and non-malignant breast tissue,8 including mammary epithelial cells,9 tumor cells including breast cancer cells,8 prostate cancer cells and subsequent bone metastases;7 dendritic cells, activated T-cells and B-cells,10 osteoblasts5 and osteoclasts, mesenchymal cells, proliferative chondrocytes, early osteocytes and periosteal cells; synovial tissue,11 cardiomyocytes, vascular smooth muscle cells, endothelial cells,12 and the GI tract.13 The clinical significance of these findings is unknown. RANK Ligand subsequently binds to its receptor, RANK, on immature and mature osteoclasts, which leads to maturation of pre-fusion osteoclasts to multinucleated osteoclasts and finally to activated osteoclasts.5. RANK is expressed on osteoclasts and osteoclast progenitors. In addition, RANK has been observed on cartilage cells (chondrocytes), mammary gland epithelial cells, and trophoblast cells.5,6,7. 1. Yasuda H, et al. Proc Natl Acad Sci USA. 1998;95: Fuller K, et al. J Exp Med. 1998;188: Lacey DL, et al. Cell. 1998;93: Lacey DL, et al. Am J Pathol. 2000;157: Boyle WJ, et al. Nature. 2003;423: Kong Y-Y, et al. Nature. 1999;397: Brown JM, et al. Urology. 2001;57: Van Poznak C, et al. J Clin Pathol. 2006;59: Fata JE, et al. Cell. 2000:103: Anderson DM, et al. Nature. 1997;390: Crotti TN, et al. Ann Rheum Dis. 2002;61: Ueland T, et al. Circulation. 2005;111: Moschen AR, et al. Gut. 2005;54: Hsu H, et al. Proc Natl Acad Sci USA. 1999:96: Activated. Osteoclast. Osteoblast. Lineage. CFU-M = colony forming unit macrophage. Bone. Adapted from Boyle WJ, et al. Nature. 2003;423:")
95
Denosumab Mechanism of Action
RANKL RANK OPG CFU-M Dmab Pre-Fusion Osteoclast Growth Factors Hormones Cytokines Multinucleated Osteoclast Denosumab is an investigational, fully human monoclonal antibody that binds with high affinity to, and inhibits the activity of human RANK (receptor activator of nuclear factor kappa B) ligand, a key mediator of osteoclast activity1. RANK Ligand is an essential pathway in the formation, activation, and survival of osteoclasts1,2. Denosumab does not bind to other TNF receptors.1 The pharmacokinetics (SC administration) of denosumab in postmenopausal women were nonlinear with dose. The serum profiles were characterized by three distinct phases: 1) a prolonged absorption phase: maximum serum concentrations increased disproportionately greater (2.6-fold) than the increase in dose and were observed between 5 and 21 days after administration; 2) a prolonged -phase: half-lives that increased with dose to a maximum of 32 days; and 3) a more rapid terminal phase observed at concentrations <1,000 ng/mL with a half-life that increased from 5 to 10 days as dose increased from 0.01 to 3.0 mg/kg. The mean serum residence time increased with dose from 12 to 46 days.1 1. Bekker PJ, et al. A single-dose placebo-controlled study of AMG-162, a fully human monoclonal antibody to RANKL, in postmenopausal women. J Bone Miner Res. 2004;19: 2. Boyle WJ, et al. Osteoclast differentiation and activation. Nature. 2003;423: 3. Peterson MC, et al. AMG 162 maintains serum concentrations for up to 9 months following a single subcutaneous dose in healthy postmenopausal women. J. Bone Miner. Res. 2003; 18(Suppl 2):S166. Abstract SA393 and poster. RANKL Osteoclast Osteoblast Lineage CFU-M = colony forming unit macrophage Bone 95
 ligand, a key mediator of osteoclast activity1. RANK Ligand is an essential pathway in the formation, activation, and survival of osteoclasts1,2. Denosumab does not bind to other TNF receptors.1. The pharmacokinetics (SC administration) of denosumab in postmenopausal women were nonlinear with dose. The serum profiles were characterized by three distinct phases: 1) a prolonged absorption phase: maximum serum concentrations increased disproportionately greater (2.6-fold) than the increase in dose and were observed between 5 and 21 days after administration; 2) a prolonged -phase: half-lives that increased with dose to a maximum of 32 days; and 3) a more rapid terminal phase observed at concentrations <1,000 ng/mL with a half-life that increased from 5 to 10 days as dose increased from 0.01 to 3.0 mg/kg. The mean serum residence time increased with dose from 12 to 46 days Bekker PJ, et al. A single-dose placebo-controlled study of AMG-162, a fully human monoclonal antibody to RANKL, in postmenopausal women. J Bone Miner Res. 2004;19: Boyle WJ, et al. Osteoclast differentiation and activation. Nature. 2003;423: Peterson MC, et al. AMG 162 maintains serum concentrations for up to 9 months following a single subcutaneous dose in healthy postmenopausal women. J. Bone Miner. Res. 2003; 18(Suppl 2):S166. Abstract SA393 and poster. RANKL. Osteoclast. Osteoblast. Lineage. CFU-M = colony forming unit macrophage. Bone. 95.")
96
Dmab-FREEDOM Results 68% decrease in vertebral fractures
2.3% vs 7.2%, P<0.0001 40% decrease in hip fractures 0.7% vs. 1.2%, P=0.036 20% decrease in non-vertebral fractures 6.5% vs. 8.0%, P=0.011 Dmab increased BMD and reduced BTMs compared to placebo AEs and SAEs generally similar to placebo No increased risk of cancer, infection, CV disease, delayed fracture healing, hypocalcemia, no ONJ Increased risk of cellulitis, eczema, flatulence Decreased risk of falls, concussion Cummings SR et al. N Engl J Med. 2009;361:1-10.

97
Choosing Therapy Deciding who to treat Deciding how to treat
Utility of DXA and VFA Using NOF 2008 & FRAX to guide clinical decisions Deciding how to treat Non-pharmacologic therapy Pharmacologic therapy Initial choice of therapy- Anticatabolic or Anabolic agent Prevention vs Treatment Dosing Sequential therapy- Forteo Repeat therapy- Forteo 97

98
Clinical Challenges after Starting Treatment
Motivating the patient to fill the prescription, take it correctly, regularly, for a length of time to benefit- Cost? Determining how, when, (or if) to follow and monitor the patient to assure that benefit is achieved Managing Nonresponders? Suboptimal Responders? Deciding when (if ever) to stop or change therapy Knowing when (if ever) to restart, if treatment is stopped The Drug Holiday Managing side effects, perceived side effects, and fear of side effects 98
 to follow and monitor the patient to assure that benefit is achieved. Managing Nonresponders Suboptimal Responders Deciding when (if ever) to stop or change therapy. Knowing when (if ever) to restart, if treatment is stopped- The Drug Holiday. Managing side effects, perceived side effects, and fear of side effects. 98.")
99
Surgeon General’s Report on Bone Health and Osteoporosis
Leading the Effort to Help Prevent and Treat Osteoporosis Pharmacotherapy (antiresorptives and anabolics) Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Surgeon General’s Report on Bone Health and Osteoporosis Pyramid for Osteoporosis Prevention and Treatment What does this mean for your patients? US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General; 2004.
 Address Secondary Factors (drugs and diseases) Lifestyle Changes (nutrition, physical activity, and fall prevention) Surgeon General’s Report on Bone Health and Osteoporosis. Pyramid for Osteoporosis Prevention and Treatment. What does this mean for your patients US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General;")
100
2008 NOF Clinician’s Guide & FRAX
100 100

101
NOF 2008 Treatment Guidelines
Postmenopausal women and men age 50 and older with the following should be considered for treatment, after evaluation for secondary causes of osteoporosis: Osteoporosis T-score -2.5 or less at FN or LS after evaluation for secondary causes, or Hip or vertebral (clinical or morphometric) fracture Osteopenia T-score between -1.0 and -2.5 at FN or LS, and FRAX 10-year probability of major osteoporotic fracture ≥20% or hip fracture ≥3% National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis 101
 fracture. Osteopenia. T-score between -1.0 and -2.5 at FN or LS, and. FRAX 10-year probability of major osteoporotic fracture ≥20% or hip fracture ≥3% National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis")
102
Conclusions Exercise, Fall Risk Nutrition No smoking, minimal drinking
Calcium per day Vitamin D ~ per day Central bone density test - DXA & VFA Secondary Cause Review-Imaging & Lab workup Medications Anti-resorptives, Anabolics 102

103
But, do I really have to take those medicines?
Will I end up like my mother? Fracture Risk Assessment Intervention Thresholds I saw on the News last night..... Treatment Follow-up 103

104
Thank You Portland Headlight

Similar presentations



>")


>")













