Download presentation
Presentation is loading. Please wait.

1
This lecture was conducted during the Nephrology Unit Grand Ground by a Sub- intern under Nephrology Division, Department of Medicine in King Saud University. Nephrology Division is NOT responsible for the content of the presentation for it is intended for learning and /or education purpose only.

2
Light Chain- Associated Renal Disorders Ali Yousef AlGhar Resident R1 King Khalid University Hospital 27/may/2014

3
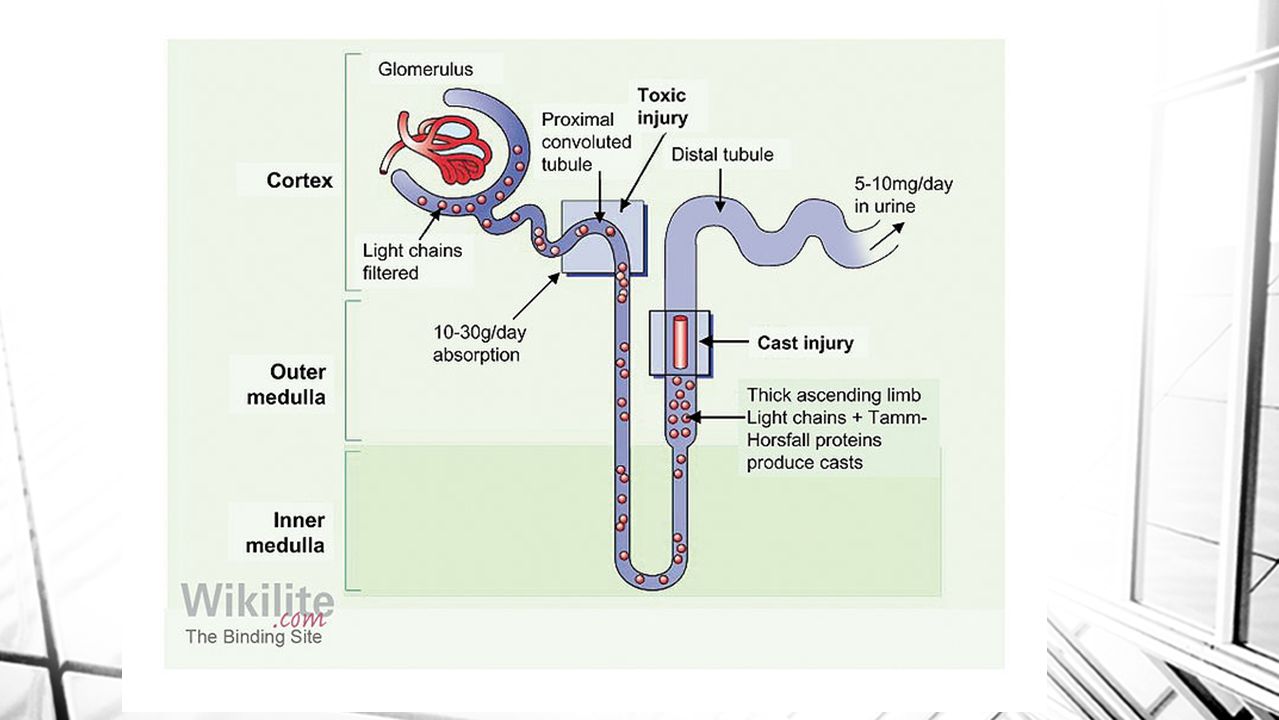
physiology Light chains (molecular weight 22,000 d) are polypeptides Light chains are divided into kappa and lambda. Kappa filtered through the glomerulus. Lambda are less likely to be filtered and appear in urine. At times, light chains of either kappa or lambda type may form tetramers (88,000 d), which are not filtered.
, which are not filtered..")
4
The kidney is the major site of metabolism of light- chain proteins. reabsorbed by the proximal tubular cells. light-chain proteins appear in urine in high concentration either when the production of light- chain proteins is markedly increased or when the ability of the proximal tubules to reabsorb all the filtered protein is exceeded.

6
MYELOMA CAST NEPHROPATHY over-production, filtration and overabundance of toxic light chains in the ascending loop of Henle, leading to both tubular injury and intratubular cast formation and obstruction. specific binding to Tamm-Horsfall mucoprotein, which have a specific binding site of nine amino acid segment binds to the complementary determining region 3 (CDR3) of immunoglobulin light chains
 of immunoglobulin light chains.")
11
Most patients present with an elevated creatinine and minimal proteinuria by urine dipstick. 24 hour urine electrophoresis studies, it will show monoclonal light chains, while in amyloidosis and MIDD, most of the proteinuria will consist of albumin and the monoclonal light chain component will be small.

12
43 Vs 22% one-year patient survival was 80 percent in those with a plasma creatinine concentration 2.3 mg/dL (200 micromol/L) at disease presentation. renal functional recovery was seen in 26 percent of those with renal insufficiency at presentation. These patients had a median survival of 28 months, compared with 4 months in those with irreversible renal failure

13
Algorithm of diagnostic procedures in AL-amyloidosis and monoclonal Ig deposition disease. Ronco P et al. CJASN 2006;1:1342-1350 ©2006 by American Society of Nephrology

14
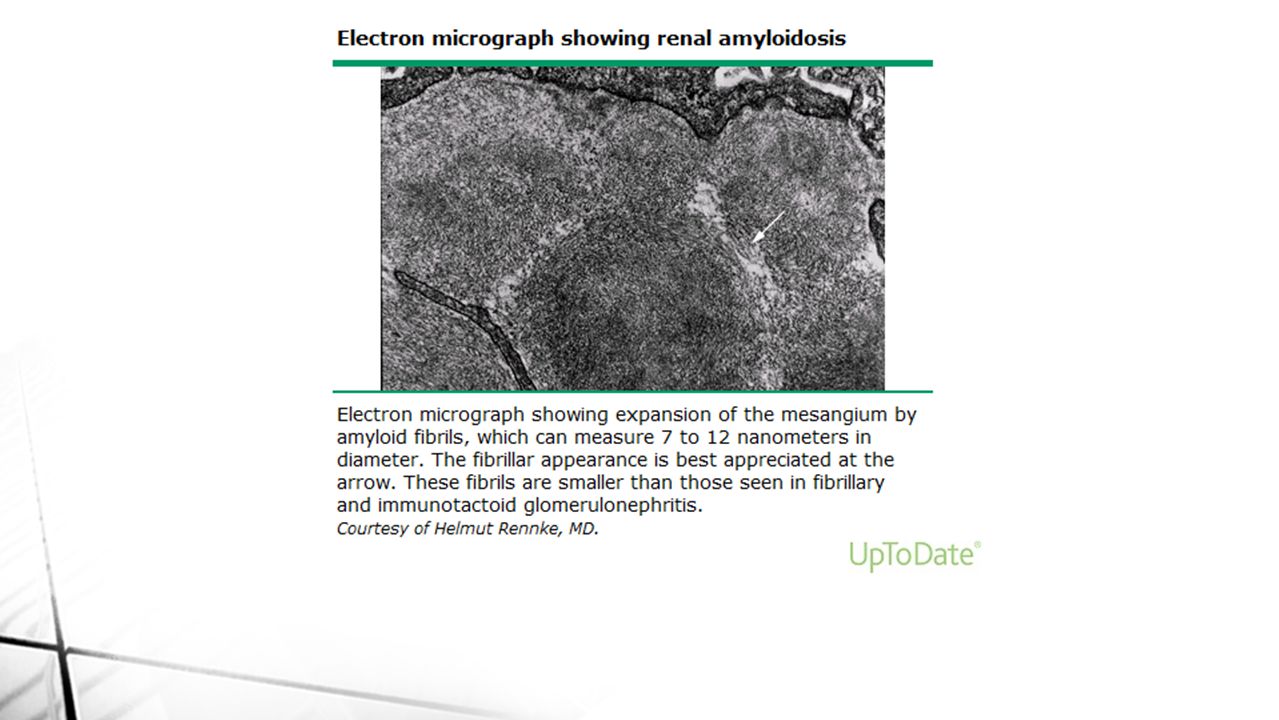
Amyloidosis Amyloidosis is a group of diseases characterized by extracellular deposition of beta-sheet fibrils. They include immunoglobulin (Ig) light chains in primary systemic amyloidosis (AL), Ig heavy chain (AH), amyloid A in secondary amyloidosis (AA), beta2-microglobulin in dialysis-associated arthropathy (Ab2M), amyloid beta protein (Ab) in Alzheimer disease and Down syndrome.
 light chains in primary systemic amyloidosis (AL), Ig heavy chain (AH), amyloid A in secondary amyloidosis (AA), beta2-microglobulin in dialysis-associated arthropathy (Ab2M), amyloid beta protein (Ab) in Alzheimer disease and Down syndrome..")
15
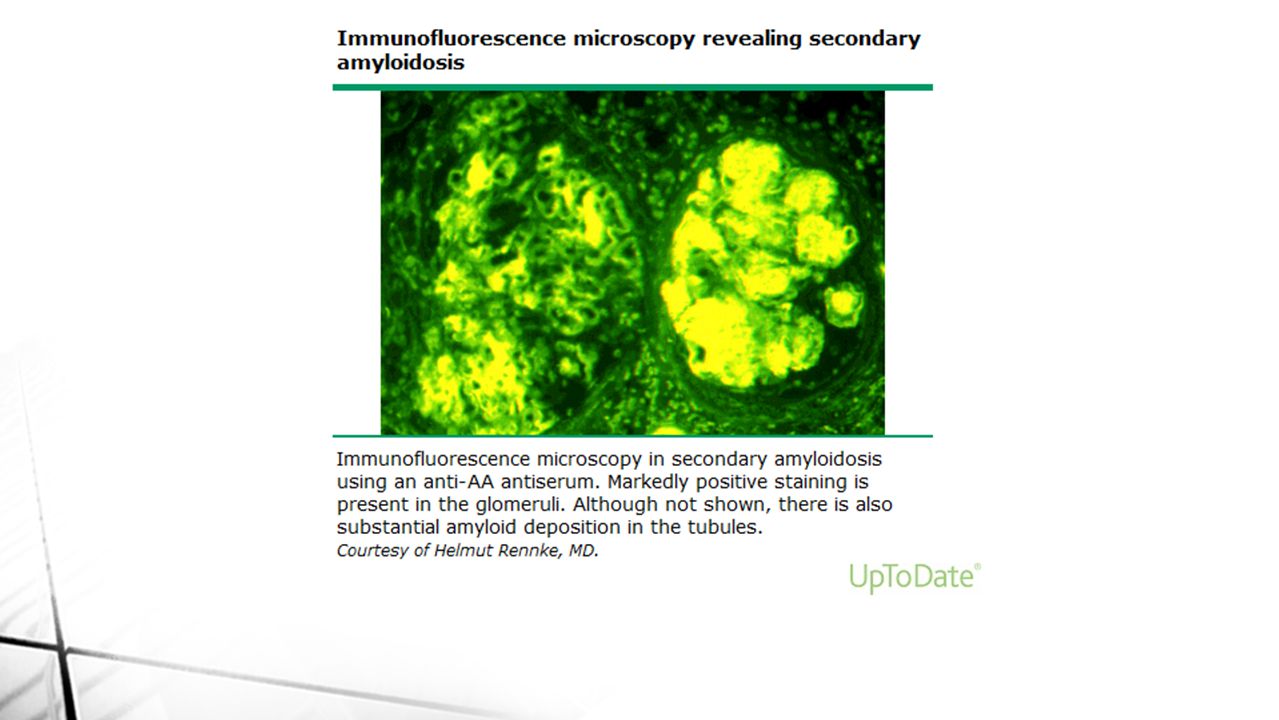
Glomerular deposits AL amyloidosis have predominant glomerular deposition. AL amyloidosis, 75 percent of patients present with proteinuria. End-stage renal disease develops in approximately 20 percent of those with the nephrotic syndrome, with poor patient survival overall. Glomerular deposits are more common and associated with a poor renal prognosis in patients with AA from rheumatoid arthritis (RA). 27 of 38 patients who had renal amyloidosis due to RA had glomerular deposits, and 85 percent of them progressed to end-stage renal disease during the five-year observation period
. 27 of 38 patients who had renal amyloidosis due to RA had glomerular deposits, and 85 percent of them progressed to end-stage renal disease during the five-year observation period.")
19
Vascular and tubular amyloid deposits These patients usually present with slowly progressive chronic kidney disease with little or no proteinuria. Why this occurs is unclear, but the site of deposition may be determined at least in part by the size of the amyloid A fragment that is formed. Prognosis in such patients appears to be more favorable. Even less common is heavy tubular deposition, potentially leading to signs of tubular dysfunction such as type 1 (distal) renal tubular acidosis or polyuria due to nephrogenic diabetes insipidus. Acquired Fanconi syndrome has been reported in rare cases
 renal tubular acidosis or polyuria due to nephrogenic diabetes insipidus. Acquired Fanconi syndrome has been reported in rare cases.")
23
Crescentic glomerulonephritis Although rare, Almost all reported patients have had AA amyloidosis due to rheumatoid arthritis or its variants. A possible mechanism is amyloid fibril-induced ruptures in the capillary loops, leading to fibrin entry into Bowman's space. Another possibility is that the glomerulonephritis is related to rheumatoid arthritis or its therapy. develops acute renal failure in association with an active urine sediment. Optimal therapy of this problem is not known

28
Pathogenesis of immunoglobulin light chain (AL) amyloidosis and light and heavy chain deposition diseases Clinical features, laboratory manifestations, and diagnosis of multiple myeloma Renal amyloidosis Pathogenesis and diagnosis of myeloma cast nephropathy (myeloma kidney) Light Chain-Associated Renal Disorders Workup ( Medscape ) http://www.uptodate.com/contents/pathogenesis-of-immunoglobulin-light- chain-al-amyloidosis-and-light-and-heavy-chain-deposition-diseases#H2 http://www.uptodate.com/contents/pathogenesis-of-immunoglobulin-light- chain-al-amyloidosis-and-light-and-heavy-chain-deposition-diseases#H2 http://www.pathologyoutlines.com/topic/kidneylightchaindepositiondisease.ht ml http://www.pathologyoutlines.com/topic/kidneylightchaindepositiondisease.ht ml http://cjasn.asnjournals.org/content/1/6/1342.full
 amyloidosis and light and heavy chain deposition diseases Clinical features, laboratory manifestations, and diagnosis of multiple myeloma Renal amyloidosis Pathogenesis and diagnosis of myeloma cast nephropathy (myeloma kidney) Light Chain-Associated Renal Disorders Workup ( Medscape ) chain-al-amyloidosis-and-light-and-heavy-chain-deposition-diseases#H2 chain-al-amyloidosis-and-light-and-heavy-chain-deposition-diseases#H2 ml ml")
Similar presentations






















 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")








