Download presentation
Presentation is loading. Please wait.

1
BLA 99-0884: Enbrel for Early RA Jeffrey N. Siegel, M.D. Division of Clinical Trials Design and Analysis

2
Review committee u Jeffrey Siegel, M.D.Chair, Clinical u George Mills, M.D.Imaging u Boguang Zhen, Ph.D.Biostatistics u Susan Giuliani Project Manager u Debra Bower Bioresearch Monitoring u David Green, Ph.D.Pharm-tox u Lisa Rider, M.D.Consultant

3
Current indication u Enbrel is indicated for reduction in signs and symptoms of moderately to severely active rheumatoid arthritis in patients who have had an inadequate response to one or more disease-modifying antirheumatic drugs (DMARDs). Enbrel can be used in combination with methotrexate in patients who do not respond adequately to methotrexate alone.

4
Indications sought in current BLA u Extend indication to signs & symptoms in early RA patients u Seek general claim of prevention of structural damage

5
Outline of presentation u Trial design u Modifications to protocol u Background information on radiographic endpoints u Efficacy results u Safety data

6
Primary endpoints u Co-primary endpoints: –Clinical: ACR-N AUC at 6 mo –Radiographic: Improvement in erosion scores at 12 mo –Hochberg method of assessing statistical significance: both EPs must achieve statistical significance at 0.05 level OR either at 0.025 level

7
Additional endpoints u Disability based on Health Assessment Questionnaire (HAQ) u Health-related quality of life (HRQL) u Major clinical response
 u Health-related quality of life (HRQL) u Major clinical response")
8
Outline of presentation u Trial design u Modifications to protocol u Background information on radiographic endpoints u Efficacy results u Safety data

9
16.0012: Modifications u During trial, the agency discussed with Immunex evidence from recent reports that many patients with early RA treated with MTX developed few, if any, erosions u The agency asked Immunex if it would wish to seek an approval based on non-inferiority if the study did not demonstrate superiority to MTX. u The agency noted that the basis for a non- inferiority determination should be determined prospectively

10
Modifications (cont.) u Immunex revised analysis of radiographic endpoint to a demonstration of non- inferiority u Changed variable from erosion score to total Sharp score (erosion score + joint space narrowing score) –Reason: Data unavailable to establish effect size for erosion score
 u Immunex revised analysis of radiographic endpoint to a demonstration of non- inferiority u Changed variable from erosion score to total Sharp score (erosion score + joint space narrowing score) –Reason: Data unavailable to establish effect size for erosion score")
11
Outline of presentation u Trial design u Modifications to protocol u Background information on radiographic endpoints u Efficacy results u Safety data

12
Non-inferiority trials u In some clinical settings, efficacy may be demonstrated from a finding of non- inferiority in an active control trial: –Reproducible historical experience indicates that in a trial with a given design that the active control will reliably give a result of a given size

13
0 Progression Rate Margin active minus placebo (historical) Efficacy of active control New drug superior New drug meets non-inferiority std. No evidence of efficacy New drug minus Active

14
Steps to Establish Non-Inferiority Ê Determine from historical trials that active control reliably has an effect of at least a certain size Ë Plan trial design to be similar to that of prior trials (stage of disease, concomitant therapy, endpoint, etc.) Ì Set a non-inferiority margin to be excluded (smaller than the total active control effect) Í Ensure appropriate trial conduct (e.g., concomitant meds, study drug compliance)
 Ì Set a non-inferiority margin to be excluded (smaller than the total active control effect) Í Ensure appropriate trial conduct (e.g., concomitant meds, study drug compliance)")
15
Historical control data u Sponsor derived effect size of active control from several studies, including: –A multi-year observational study of recent- onset RA (Wolfe and Sharp, 1998) –A 3-arm, randomized, controlled study comparing placebo, MTX and ARAVA (MN301/303)
 –A 3-arm, randomized, controlled study comparing placebo, MTX and ARAVA (MN301/303)")
16
Non-inferiority: assumptions u Mean yearly progression rate ~6 u/year (Sharp score) in untreated patients u Mean progression rate on MTX ~2 u/yr u Preserving 70% of MTX benefit means ruling out a difference of 1.2 u [(4-1.20/4 = 0.70]
![Non-inferiority: assumptions u Mean yearly progression rate ~6 u/year (Sharp score) in untreated patients u Mean progression rate on MTX ~2 u/yr u Preserving 70% of MTX benefit means ruling out a difference of 1.2 u [(4-1.20/4 = 0.70]](http://images.slideplayer.com/19/5731187/slides/slide_16.jpg "Non-inferiority: assumptions u Mean yearly progression rate ~6 u/year (Sharp score) in untreated patients u Mean progression rate on MTX ~2 u/yr u Preserving 70% of MTX benefit means ruling out a difference of 1.2 u [(4-1.20/4 = 0.70]")
17
Limitations of non-inferiority trial design u Historical controls do not provide reproducible data to establish effect size for MTX u Effect size for MTX based on different patient population from current study: –shorter duration of disease –different MTX regimen

18
Non-inferiority design: conclusions u Because cannot formally establish a minimal effect size, non-inferiority cannot per se be taken as evidence of efficacy u Therefore, interpretation of the trial must be based on totality of the data, including additional analyses

19
Outline of presentation u Trial design u Modifications to protocol u Background information on radiographic endpoints u Efficacy results u Safety data

20
Disposition of subjects

21
Radiographic procedures u Hand, foot films obtained: baseline, 6, 12 mo u Read: 6 trained readers, blinded, random order u Inter--reader correlation coefficient 0.8 u Agency review of radiographs: –Data complete, of uniformly good quality –Readings generally consistent and accurate

22
Primary endpoint analysis u Primary analysis specified a mixed model estimating annual x-ray progression rates using 0, 6 & 12 month films and baseline covariates u Non-inferiority analysis to exclude margin of 1.2 u/year u Protocol specified sequential test of: –non-inferiority –if non-inferiority demonstrated, test superiority

23
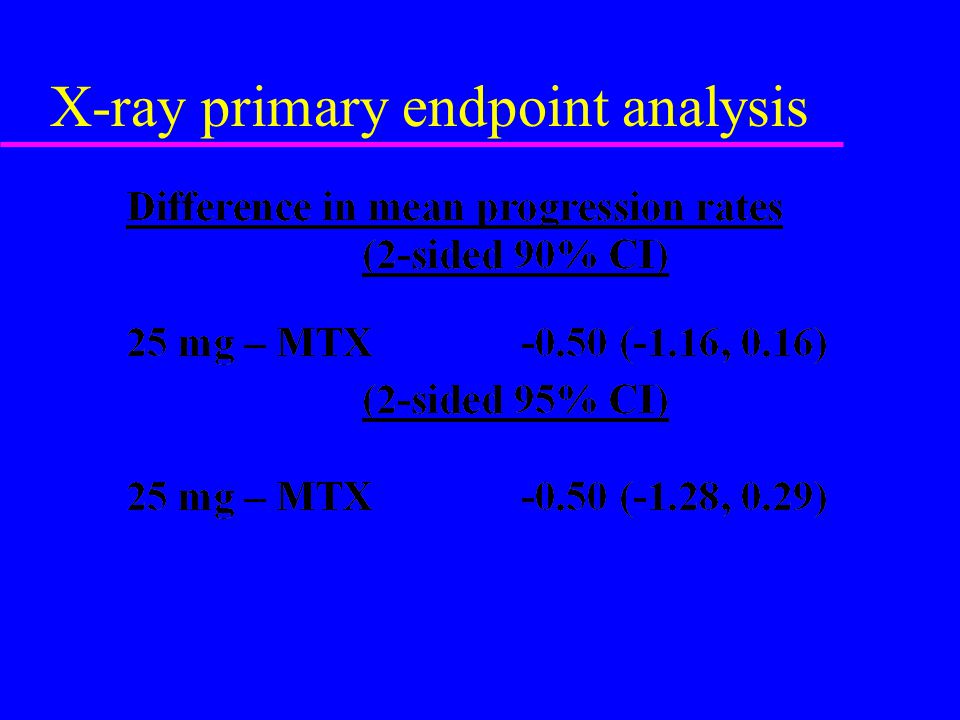
X-ray primary endpoint analysis

25
Primary endpoint u Test of non-inferiority excluded margin of greater than 1.2 u/yr (max. outer bound 0.29) u Test of superiority of Enbrel 25 mg to MTX does not reach statistical significance (p=.21)
 u Test of superiority of Enbrel 25 mg to MTX does not reach statistical significance (p=.21).")
26
Additional analyses u Prespecified stratification by disease duration u Components of Sharp score: erosion scores u 6 month vs. 12 month data u Subjects w/ no radiographic progression

27
Analysis by disease duration: TSS N=478N=154

28
Components of total Sharp score u Total Sharp score (TSS) is summation of: –erosion score –joint space narrowing u Enbrel 25 mg showed decrease in erosion score compared to MTX (0.9 vs. 0.4 u/yr, p =.047) u No difference in joint space narrowing (0.4 u/yr)
 u No difference in joint space narrowing (0.4 u/yr).")
29
Time course of x-ray changes u Analyze 0-6, 6-12 mo rate of change u Agency observed substantial skewing of data, violating assumptions of mixed model. Therefore non-parametric test more appropriate u For its analysis, agency used raw data for last observation and first observation adjusting for time interval

30
12 mo change in erosion scores P=0.001

31
Changes over time: erosions P = 0.0006P = NS

32
Changes over time: TSS P = 0.0006P = NS

33
Patients w/ no radiographic progression P = 0.004P = 0.174

34
Subset analysis u Based subset analysis on 12-month change in erosion scores u No important differences based on age, ethnicity, gender, duration of disease (0-18 mo vs. 18-36 mo) u Also assess baseline prognostic variables: – ESR, erosions at baseline
 u Also assess baseline prognostic variables: – ESR, erosions at baseline.")
35
Erosion score/Baseline ESR > 30 N=115 N=121 N=92 N=96

36
Erosions/baseline erosions N=137 N=145 N=69 N=72

37
Radiographic EP u Although the trial excluded pre-specified margin for non-inferiority, there are limitations to the interpretation of these data u Meaningful secondary endpoints showed a difference compared to active control, e.g. erosion scores, 6 month data, patients with no radiographic progression

38
Clinical EP: Summary u 1 0 endpoint of 6 month AUC showed statistically significant difference between Enbrel 25 mg and MTX u Landmark analysis of proportion of subjects achieving ACR20 and 50 at 6 and 12 months not statistically significant

39
Additional endpoints u Disability (HAQ) u Health-related quality of life u Major clinical response
 u Health-related quality of life u Major clinical response")
40
Disability

41
Health related Quality of life u Physical summary score: –Same across trial arms at baseline, ~ 2 SD below US norms –Improved in all arms at 12 months »Less improvement in 10 mg arm than 25 mg Enbrel arm u Mental health summary score: –Similar to US norms at baseline –Higher in all arms at 12 months

42
Major Clinical Response (MCR) u Rationale for criteria of ACR70: –Represents a degree of improvement rarely seen in placebo arms of controlled studies of DMARDs: »Placebo (MTX vs. placebo): 0% »Placebo (CsA vs pl/background MTX): 0% u Definition: –6 consecutive months of an ACR70
: 0% »Placebo (CsA vs pl/background MTX): 0% u Definition: –6 consecutive months of an ACR70.")
43
Major Clinical Response (MCR) P = 0.06
 P = 0.06")
44
Safety u Serious AEs, deaths u Drop-out for adverse events u Other AEs u Long-term safety u Post-marketing reports

45
Deaths in trial 16.0012 u 2 observed during 12 month study period –10 mg: Lung ca, dx month 2 –25 mg: non-infectious complications of an aortic aneurysm repair

46
SAEs

47
Infectious SAEs

48
Malignancies u 25 mg –Prostate, carcinoid (lung), Hodgkin’s u 10 mg –breast, lung u MTX –colon –1 additional ca, at beginning of second year: bladder
, Hodgkin’s u 10 mg –breast, lung u MTX –colon –1 additional ca, at beginning of second year: bladder")
49
Thrombotic SAEs u 25 mg: –DVT (2): »3 mo on study. Risk factor: OCP »1 week on study. Risk factor: Baker’s cyst u 10 mg: –DVT: 2 weeks on study. No risk factors –Massive PE associated with dx of lung ca u MTX: none

50
Safety u Serious AEs, deaths u Drop-out for adverse events u Other AEs u Long-term safety u Post-marketing reports

51
Subjects not completing 52 weeks dosing

52
AEs causing dropouts

53
Safety u Serious AEs, deaths u Drop-out for adverse events u Other AEs u Long-term safety u Post-marketing reports

54
Other adverse events u Overall adverse event rate higher in MTX arm than with Enbrel: –MTX 95% vs. Enbrel 90% u Rate of ISR (37% vs. 7%), bleeding at injection site (14% vs. 10%) higher in Enbrel arm than MTX u No other pattern of increased adverse events observed with Enbrel
, bleeding at injection site (14% vs. 10%) higher in Enbrel arm than MTX u No other pattern of increased adverse events observed with Enbrel.")
55
Safety u Serious AEs, deaths u Drop-out for adverse events u Other AEs u Long-term safety u Post-marketing reports

56
Safety in other clinical trials u In previous controlled trials, saw higher incidence of: –injection site reactions –infections u Upper respiratory infections (URIs) were major contributor to higher rate of infection u Serious infections seen in long-term extension studies
 were major contributor to higher rate of infection u Serious infections seen in long-term extension studies")
57
Phase 4 safety study: 16.0018 u 3-year, open-label study of 1200 subjects receiving Enbrel u 638 enrolled at time of BLA submission u Goals: –Assess long-term safety, including mortality rate, incidence of malignancy and autoimmune disease compared to historical control databases

58
Long-term safety in DMARD- refractory RA u Size of database –782 patients overall (16.0018 and others) »2-3 years: 71 patients »1-2 years: 502 patients u AE rate: –None occurred with an incidence higher than in controlled studies –No AE with pattern of increased incidence with longer duration of exposure
 »2-3 years: 71 patients »1-2 years: 502 patients u AE rate: –None occurred with an incidence higher than in controlled studies –No AE with pattern of increased incidence with longer duration of exposure")
59
Long-term safety u Infections –Types of infection similar to that seen in controlled trials –No infection with a higher incidence with long- term treatment

60
Long-term safety: serious infections u Infections assoc with hospitalization or IV antibiotics –Incidence of 5.5/100 patient-years –Types of infections expected for patients with RA in their age group u No increase in rate with longer duration of exposure

61
Safety u Serious AEs, deaths u Drop-out for adverse events u Other AEs u Long-term safety u Post-marketing reports

62
Post-marketing reports u Post approval of Enbrel, there were reports of deaths from serious infection and sepsis –Associated risk factors: diabetes, active infection, h/o recurrent infection u Actions taken: –Issue dear doctor letter with warning about use of Enbrel in patients with DM, active infections or a history of chronic infections –Agency asked sponsor to initiate clinical trial to assess degree of risk

63
Safety study of Enbrel in patients at risk of infection u Since clinical trials excluded patients at higher risk for infection, it is unknown whether Enbrel may predispose certain subgroups of patients to serious infection

64
Safety study in at-risk patients u 1000-patient, randomized, 4-month, double- blind, placebo-controlled trial of Enbrel u Inclusion criteria: –RA by ARA criteria –At increased risk for infection: »DM requiring insulin or oral hypoglycemics »Chronic pulmonary disease (COPD or asthma) »h/o pneumonia in past year »Recurrent bronchitis, sinusitis or UTI (at least 2 episodes in past year)
 »h/o pneumonia in past year »Recurrent bronchitis, sinusitis or UTI (at least 2 episodes in past year)")
65
Safety study in at-risk patients u Sample size calculations: –Assumes event rate of 10% in control –94% power to exclude a 2x relative risk for Enbrel (95% CI) –Power of study would be lower if event rate below 10%
 –Power of study would be lower if event rate below 10%")
66
Conclusions u For x-ray data, 95% CI excluded inferiority of 1.2 u/yr –Secondary endpoints suggest superiority of Enbrel in preventing erosions u Primary signs & symptoms endpoint showed superiority for Enbrel 25 mg –Landmark 6, 12 month ACR 20/50 higher for Enbrel 25 mg, but not statistically significant u Overall AE/SAE rate not higher with Enbrel

Similar presentations

















 for Rheumatoid Arthritis Biological License Application Arthritis Advisory Committee September 6, 2005.>")

