Download presentation
Presentation is loading. Please wait.

1
INTRODUCTION, JAUNDICE, CHOLESTASIS, LIVER FAILURE, CIRRHOSIS.
LIVER DISEASE INTRODUCTION, JAUNDICE, CHOLESTASIS, LIVER FAILURE, CIRRHOSIS.

3
INTRODUCTION Liver weight 1400 - 1600gm.
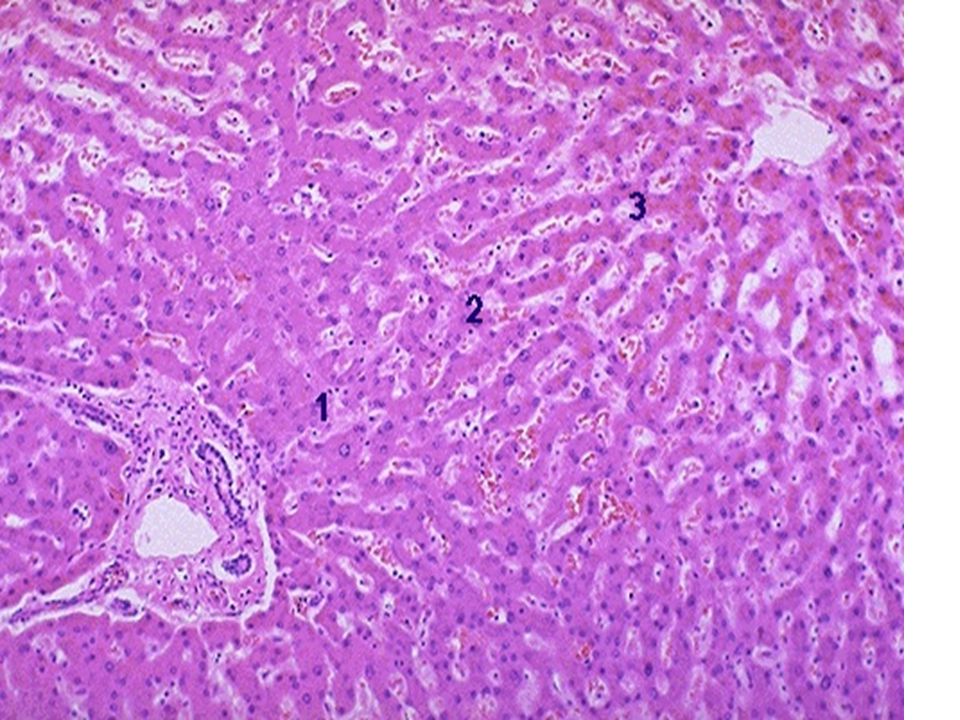
Parenchyma - liver cells (hepatocytes) trabeculae 1 cell thick in adults Kupffer cells in sinusoids are phagocytes hepatic stellate cells in space of Disse, store vitamin A, transform into collagen-producing myofibroblasts, regulate blood flow in sinusoids liver-associated lymphocytes. Biliary drainage system - canaliculi (in centre of liver cell plates) canals of Hering & cholangioles intra-hepatic bile ducts extra-hepatic bile ducts. Vasculature - portal vein supplies 70% of the blood flow hepatic artery supplies 30% of the blood flow sinusoids lined by fenestrated endothelium hepatic venules, hepatic veins drain into the IVC.
 trabeculae 1 cell thick in adults. - Kupffer cells in sinusoids are phagocytes. - hepatic stellate cells in space of Disse, store vitamin A, transform into collagen-producing myofibroblasts, regulate blood flow in sinusoids. - liver-associated lymphocytes. Biliary drainage system - canaliculi (in centre of liver cell plates). - canals of Hering & cholangioles. - intra-hepatic bile ducts. - extra-hepatic bile ducts. Vasculature - portal vein supplies 70% of the blood flow. - hepatic artery supplies 30% of the blood flow. - sinusoids lined by fenestrated endothelium. - hepatic venules, hepatic veins drain into the IVC.")
6
The functional unit of the liver parenchyma is the hepatic acinus with zones 1,2 & 3. Zone 1 is periportal, zone 3 is perivenular, zone 2 intermediate. Portal tracts composed of fibrous tissue ramify in the liver and contain 3 structures, portal vein, hepatic artery, bile duct (portal triad). The liver is important for - metabolism of carbohydrate, protein,lipids protein synthesis, albumin, coagulation factors, complement factors etc storage of iron, copper, vitamins A,D,B detoxification/drug metabolism bile production. Investigation of liver diseases Biochemical - enzymes, proteins, bilirubin. Haematological - coagulation factors among others. Immunological - antibodies (viruses, autoimmune). Imaging - ultrasound,CT,MRI,ERCP,MRCP. Liver biopsy - percutaneous needle biopsy, transjugular biopsy, wedge biopsy at laparoscopy or open surgery. Useful in providing information as to the aetiology and severity of the liver disease, ruling out the presence of other concomitant disease, monitoring response to therapy. Focal lesions require US or CT guidance.
. The liver is important for - metabolism of carbohydrate, protein,lipids. - protein synthesis, albumin, coagulation factors, complement factors etc. - storage of iron, copper, vitamins A,D,B12. - detoxification/drug metabolism. - bile production. Investigation of liver diseases. Biochemical - enzymes, proteins, bilirubin. Haematological - coagulation factors among others. Immunological - antibodies (viruses, autoimmune). Imaging - ultrasound,CT,MRI,ERCP,MRCP. Liver biopsy - percutaneous needle biopsy, transjugular biopsy, wedge biopsy at laparoscopy or open surgery. Useful in providing information as to the aetiology and severity of the liver disease, ruling out the presence of other concomitant disease, monitoring response to therapy. Focal lesions require US or CT guidance.")
7
Morphological patterns of liver injury. 1
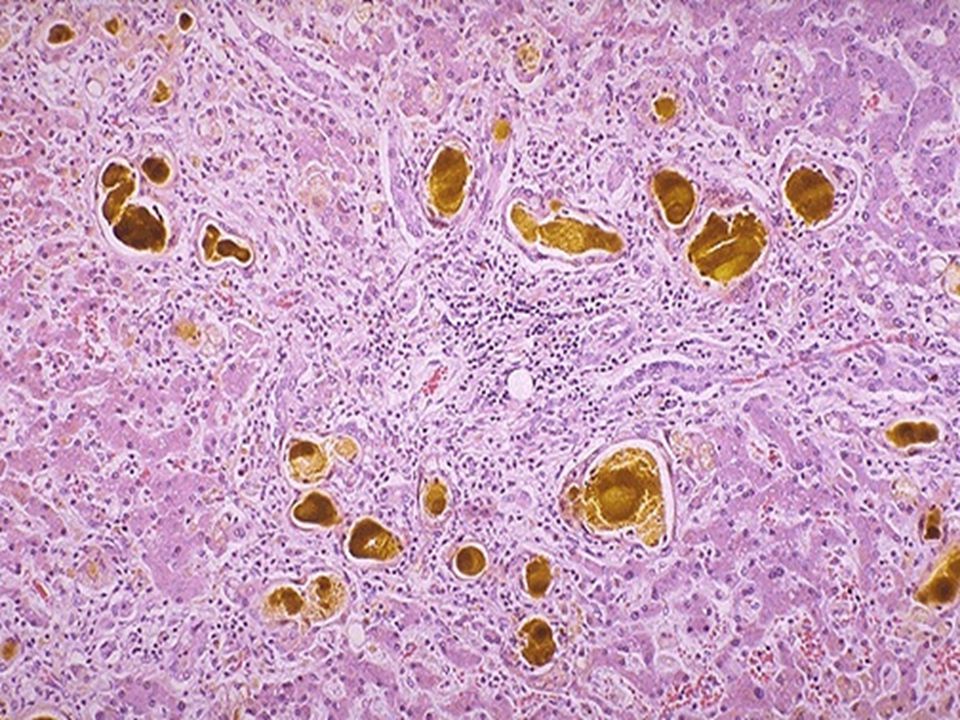
Morphological patterns of liver injury Degeneration - ballooning degeneration (hydropic change); feathery degeneration (bile-induced damage) Intracellular accumulations - fat (steatosis), iron, copper, bile, Mallory’s hyaline Necrosis - (coagulative or lytic) and apoptosis. Necrosis may be randomly focal (spotty necrosis), zonal eg zone 3, bridging (bridging hepatic necrosis, eg portal to venular), involve most or almost all of the liver (submassive and massive respectively). Zone 3 is most prone to injury as it is farthest from the blood supply and is the area containing most drug- metabolising enzymes Inflammation - acute, chronic or granulomatous. May be portal, periportal (interface hepatitis) or acinar (focal, or panacinar) Regeneration - hepatocytes have great ability to regenerate. The reserve compartment is the canal of Hering/bile ductule compartment. Activation is described as the ductular reaction Fibrosis forms in response to inflammation or direct toxic injury. Can be portal, perivenular, form bridging fibrosis, finally cirrhosis. The great variety of liver diseases and the liver’s limited patterns of response means that close clinicopathological correlation is required for their diagnosis.
; - feathery degeneration (bile-induced damage). Intracellular accumulations - fat (steatosis), iron, copper, bile, Mallory’s hyaline. 2. Necrosis - (coagulative or lytic) and apoptosis. Necrosis may be randomly focal (spotty necrosis), zonal eg zone 3, bridging (bridging hepatic necrosis, eg portal to venular), involve most or almost all of the liver (submassive and massive respectively). Zone 3 is most prone to injury as it is farthest from the blood supply and is the area containing most drug- metabolising enzymes. 3. Inflammation - acute, chronic or granulomatous. May be portal, periportal (interface hepatitis) or acinar (focal, or panacinar). 4. Regeneration - hepatocytes have great ability to regenerate. The reserve compartment is the canal of Hering/bile ductule compartment. Activation is described as the ductular reaction. 5. Fibrosis forms in response to inflammation or direct toxic injury. Can be portal, perivenular, form bridging fibrosis, finally cirrhosis. The great variety of liver diseases and the liver’s limited patterns of response means that close clinicopathological correlation is required for their diagnosis.")
8
JAUNDICE AND CHOLESTASIS
Jaundice (or icterus) - yellow discolouration of the skin, sclerae and mucous membranes due to excess plasma bilirubin (hyperbilirubinemia) Jaundice appears when plasma bilirubin exceeds 50umol/l (Normal umol/l) Liver disease is not the only cause of jaundice and many patients with significant liver disease do not have jaundice (are anicteric). Cholestasis - arrest of bile flow. A failure of adequate amounts of bile to reach the duodenum - due to interference anywhere from liver cell microsomes to the duodenum.
 - yellow discolouration of the skin, sclerae and mucous membranes due to excess plasma bilirubin (hyperbilirubinemia). Jaundice appears when plasma bilirubin exceeds 50umol/l. (Normal umol/l) Liver disease is not the only cause of jaundice and many patients with significant liver disease do not have jaundice (are anicteric). Cholestasis - arrest of bile flow. A failure of adequate amounts of bile to reach the duodenum - due to interference anywhere from liver cell microsomes to the duodenum.")
11
MECHANISMS AND CLASSIFICATION OF JAUNDICE
Mechanisms - Increased bilirubin production Decreased uptake by hepatocytes Impaired conjugation Impaired excretion - intrahepatic extrahepatic. Classification Pre-hepatic - haemolysis most important of several causes. Unconjugated bilirubin insoluble in water, not excreted in urine. Risk of brain damage in neonates (kernicterus); pigment gallstones in adults Hepatic - eg hepatitis,intra-hepatic bile duct damage, congenital hyperbilirubinemias eg Gilbert’s syndrome. Mainly conjugated (except Gilbert’s syndrome) so soluble in water resulting in dark urine. Post-hepatic - obstruction to extra-hepatic bile ducts by gallstone, stricture, tumour, or congenital biliary atresia. Conjugated bilirubin.
; pigment gallstones in adults. Hepatic - eg hepatitis,intra-hepatic bile duct damage, congenital hyperbilirubinemias eg Gilbert’s syndrome. Mainly conjugated (except Gilbert’s syndrome) so soluble in water resulting in dark urine. Post-hepatic - obstruction to extra-hepatic bile ducts by gallstone, stricture, tumour, or congenital biliary atresia. Conjugated bilirubin.")
12
In cases of hepatic jaundice, when there is predominantly hepatocyte damage, the patient is often very symptomatic and raised serum transaminases are the predominant biochemical finding. This is sometimes called “hepatocellular jaundice.” In cases where there is biliary obstruction, whether intra- or extra-hepatic, the patient has what is called “cholestatic jaundice” with pruritis, dark urine and pale stools, and with time may develop skin xanthelasmas and steatorrhoea. Serum alkaline phosphatase is raised. Mixed patterns occur. Distinction between intra-hepatic and extra-hepatic obstruction requires imaging. This should be done urgently and the obstruction relieved where at all possible.

13
LIVER FAILURE Classification. Acute - no pre-existing liver disease Chronic - pre-existing liver disease. Causes. Acute - viral hepatitis, drugs, toxins, severe fatty change (eg fatty liver of pregnancy, Reye syndrome), vascular Chronic - cirrhosis, chronic hepatitis. Morphology. Acute - varying degrees of necrosis up to massive liver necrosis (zonal to panacinar histologically). Chronic - that of cirrhosis or chronic hepatitis Chronic liver failure is more common than acute liver failure. Mortality from liver failure without liver transplantation is 75% to 90%. Drugs and viruses account for about 80% & 15% of cases of acute liver failure respectively; figures vary according to geographical area.
, vascular. Chronic - cirrhosis, chronic hepatitis. Morphology. Acute - varying degrees of necrosis up to massive liver necrosis (zonal to panacinar histologically). Chronic - that of cirrhosis or chronic hepatitis. Chronic liver failure is more common than acute liver failure. Mortality from liver failure without liver transplantation is 75% to 90%. Drugs and viruses account for about 80% & 15% of cases of acute liver failure respectively; figures vary according to geographical area.")
14
FEATURES OF LIVER FAILURE
Hepatic encephalopathy - a neuropsychiatric disturbance leading to coma. The cardinal feature of acute liver failure, progressing over hours to days. More insidious in chronic liver failure when it is a sign of worsening liver failure Pathogenesis:- nitrogenous compounds derived from bacterial action in the colon are not metabolised in the failing liver; in addition shunting of portal blood to systemic circulation by-passes the liver Compounds involved - ammonia and derivatives of aromatic amino acids (eg mercaptans, a cause of foetor hepaticus) false neurotransmitters (eg octopamine) neuroinhibitors, eg gamma-aminobutyric acid (GABA), endogenous benzodiazepines Morphology of brain - oedema; Alzheimer type 2 astrocytic reaction.
 - false neurotransmitters (eg octopamine) - neuroinhibitors, eg gamma-aminobutyric acid (GABA), endogenous benzodiazepines. Morphology of brain - oedema; Alzheimer type 2 astrocytic reaction.")
15
Jaundice - hyperbilirubinaemia; deep jaundice = worse prognosis.
Haematological - decreased clotting factors (II,VII,IX,X) results in a bleeding tendency. Cardiovascular - hyperkinetic circulation. Respiratory - hepatopulmonary syndrome. Renal - hepatorenal syndrome. Endocrine - in chronic failure - gonadal atrophy, gynaecomastia, amenorrhoea. Skin changes - in chronic failure - spider naevi, palmer erythema. Others - impaired metabolism of amino acids, carbohydrates (hypoglycaemia) and drugs; impaired protein synthesis (low albumin), systemic infections and endotoxaemia Laboratory investigations - bilirubin (>300umol/l = poor prognosis) prothrombin (>50sec.= poor prognosis) transaminases albumin Possible factors precipitating liver failure in chronic liver disease:- increase in liver injury due to virus or alcoholic binge, infection, GIT haemorrhage (which can precipitate encephalopathy, as can excess dietary protein,constipation, drugs, uraemia, hypokalaemia).
 results in a bleeding tendency. Cardiovascular - hyperkinetic circulation. Respiratory - hepatopulmonary syndrome. Renal - hepatorenal syndrome. Endocrine - in chronic failure - gonadal atrophy, gynaecomastia, amenorrhoea. Skin changes - in chronic failure - spider naevi, palmer erythema. Others - impaired metabolism of amino acids, carbohydrates (hypoglycaemia) and drugs; impaired protein synthesis (low albumin), systemic infections and endotoxaemia. Laboratory investigations - bilirubin (>300umol/l = poor prognosis). - prothrombin (>50sec.= poor prognosis). - transaminases. - albumin. Possible factors precipitating liver failure in chronic liver disease:- increase in liver injury due to virus or alcoholic binge, infection, GIT haemorrhage (which can precipitate encephalopathy, as can excess dietary protein,constipation, drugs, uraemia, hypokalaemia).")
16
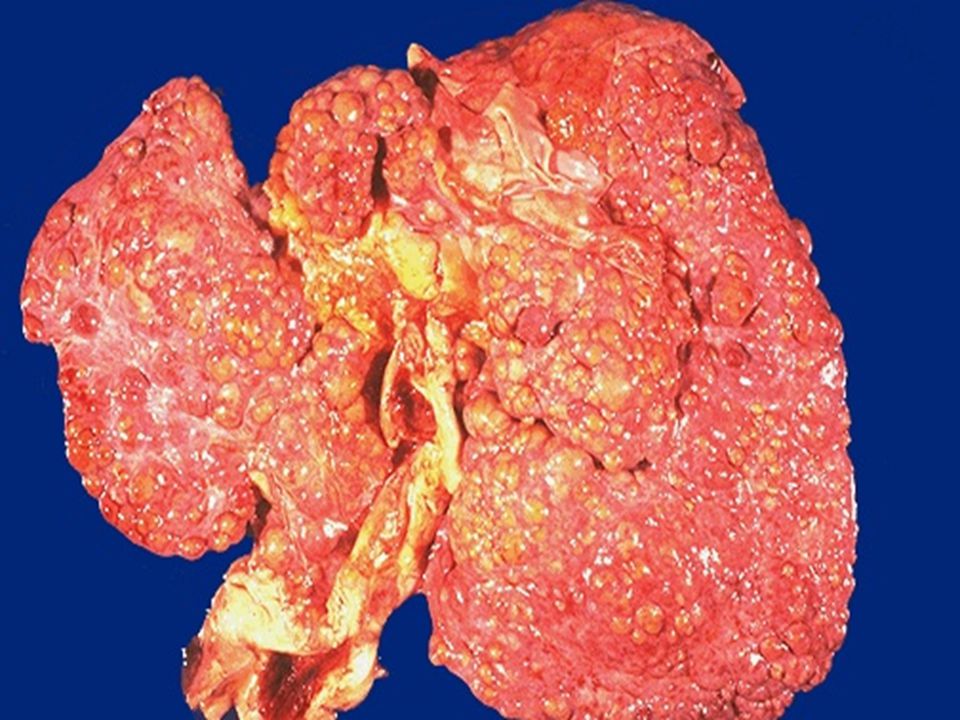
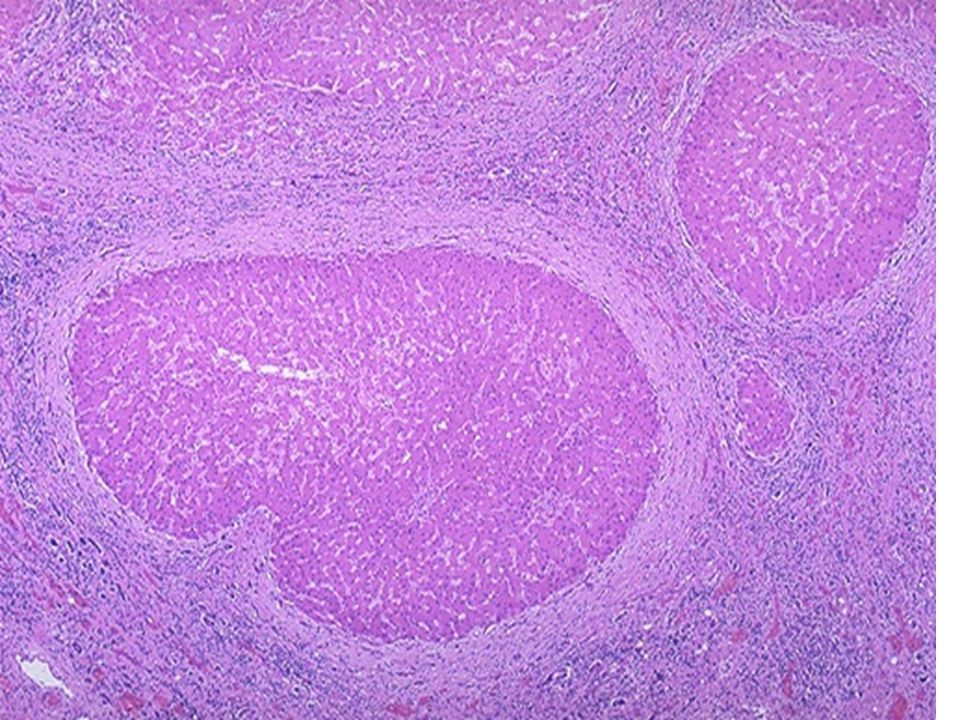
CIRRHOSIS Definition. Cirrhosis is a diffuse process in which bridging fibrosis and regenerative parenchymal nodules result in disruption of the architecture Regenerative nodules surrounded by fibrosis are necessary for the diagnosis. These may be <3mm (micronodular cirrhosis) or >3mm (macronodular cirrhosis). A micronodular cirrhosis can transform into a macronodular cirrhosis The microvasculature of the liver is markedly altered Cirrhosis is the end stage of chronic liver disease It is best classified according to aetiology.
 or >3mm (macronodular cirrhosis). A micronodular cirrhosis can transform into a macronodular cirrhosis. The microvasculature of the liver is markedly altered. Cirrhosis is the end stage of chronic liver disease. It is best classified according to aetiology.")
21
Infections. Viral hepatitis.
Toxins and drugs. Alcohol Therapeutic drugs. Autoimmune. Hepatitis Primary biliary cirrhosis. Metabolic. Haemochromatosis Wilson disease Alpha-1-antitrypsin deficiency Glycogen storage disease and many others. Biliary obstruction. Congenital atresia Sclerosing cholangitis. Hepatic outflow obstruction. Cryptogenic The aetiology of cirrhosis varies throughout the world. In the Western world, alcohol is the most common factor at 60% and viral hepatitis 10%. Viral hepatitis is the most common factor in Asia and Africa. Cryptogenic cirrhosis (cause unknown) forms 10%. Once cirrhosis has developed, it is usually not possible to determine the aetiology by morphology alone and results of other investigations are required.
 forms 10%. Once cirrhosis has developed, it is usually not possible to determine the aetiology by morphology alone and results of other investigations are required.")
22
Pathogenesis Liver injury results in chronic inflammation and activation of Kupffer cell, and other endogenous liver cells with the production of cytokines. These, together with disruption of the extracellular matrix activates hepatic stellate cells (HSC). Toxins may activate HSCs. These transform into myofibroblasts which produce collagen and constrict sinusoids Collagen in the space of Disse leads to “capillarisation” of the sinusoids and loss of endothelial fenestrations, hindering exchange of solutes New vascular channels in fibrous bands link inflow of blood (venous & arterial) with outflow (hepatic venules) thus by- passing parenchyma. Existing vascular channels and biliary channels may be obliterated. The results are internal vascular shunts and portal hypertension The hepatocytes in the regenerative nodules may appear normal microscopically but are unable to adequately fulfill their functions. Function will be further reduced if there is continuing liver cell damage.
. Toxins may activate HSCs. These transform into myofibroblasts which produce collagen and constrict sinusoids. Collagen in the space of Disse leads to capillarisation of the sinusoids and loss of endothelial fenestrations, hindering exchange of solutes. New vascular channels in fibrous bands link inflow of blood (venous & arterial) with outflow (hepatic venules) thus by- passing parenchyma. Existing vascular channels and biliary channels may be obliterated. The results are internal vascular shunts and portal hypertension. The hepatocytes in the regenerative nodules may appear normal microscopically but are unable to adequately fulfill their functions. Function will be further reduced if there is continuing liver cell damage..")
23
CLINICAL FEATURES Cirrhosis may be asymptomatic.
When symptomatic, the features are nonspecific - weakness, fatigue, weight loss, anorexia, nausea, gaseous abdominal distension, upper abdominal discomfort. The liver may be enlarged, hard and irregular or smaller than normal. At this stage the patient is said to have compensated cirrhosis. Decompensated cirrhosis manifests as signs of liver failure or complications of portal hypertension. Deterioration in liver function can be an indication of the development of hepatocellular carcinoma. Death is usually due to one of these 3 conditions.

24
COMPLICATIONS OF CIRRHOSIS
Liver failure. Portal hypertension. Portal venous pressure >10mmHg. Splenomegaly - hypersplenism leading to thrombocytopenia. Portal-systemic shunts where portal venous system anastomoses with the systemic venous system Lower end of oesophagus leading to oesophageal varices and risk of massive GIT haemorrhage. Periumbilical (“caput medusae”), lower rectum (haemorrhoids), posterior abdominal wall. Ascites, ie excess fluid in the peritoneal cavity. A transudate (<3gm/dL protein),straw coloured or pale green, a few mononuclear cells. Risk of spontaneous infection when polymorphs predominate. Is due to aldosterone-induced retention of Na & water, low oncotic pressure (low albumin), and portal hypertension. Excess hepatic lymph and intestinal fluid leakage also contributes to ascites. Hepatocellular carcinoma.
, lower rectum (haemorrhoids), posterior abdominal wall. Ascites, ie excess fluid in the peritoneal cavity. A transudate (<3gm/dL protein),straw coloured or pale green, a few mononuclear cells. Risk of spontaneous infection when polymorphs predominate. Is due to aldosterone-induced retention of Na & water, low oncotic pressure (low albumin), and portal hypertension. Excess hepatic lymph and intestinal fluid leakage also contributes to ascites. Hepatocellular carcinoma.")
Similar presentations











>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE THREE Dr. Essam H. Aljiffri.>")
 that progresses to cirrhosis Replacement of liver tissue.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")
 2. Portal area (vessels,>")









