Download presentation
Presentation is loading. Please wait.

1
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)
")
2
DEFINITION Inflammatory diseaseInflammatory disease Multi-system diseaseMulti-system disease Autoimmune diseaseAutoimmune disease

3
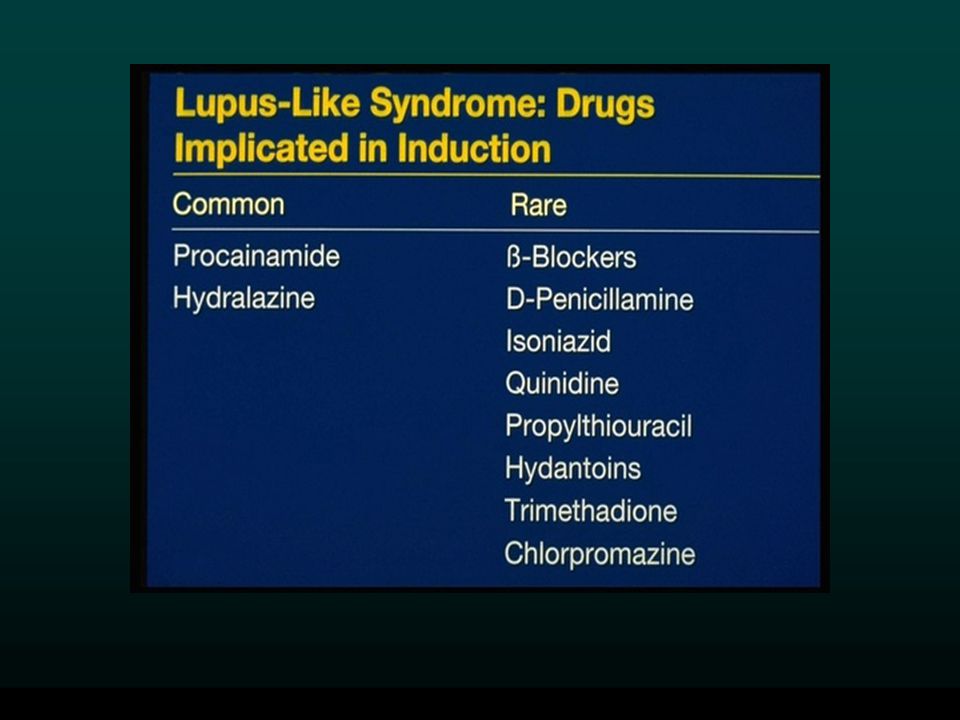
CAUSE OF SLE ??? Environmental (infections, ultraviolet light, extreme stress, certain drugs)Environmental (infections, ultraviolet light, extreme stress, certain drugs) Genetic (SLE in families, histocompatibility antigens HLA-DR2 and HLA-DR3 )Genetic (SLE in families, histocompatibility antigens HLA-DR2 and HLA-DR3 ) Hormonal states (females, pregnancy, delivery)Hormonal states (females, pregnancy, delivery) Drugs (Chlorpromazine, Methyldopa, Hydralazine, Procainamide, Isoniazid, Quinidine)Drugs (Chlorpromazine, Methyldopa, Hydralazine, Procainamide, Isoniazid, Quinidine)
Environmental (infections, ultraviolet light, extreme stress, certain drugs) Genetic (SLE in families, histocompatibility antigens HLA-DR2 and HLA-DR3 )Genetic (SLE in families, histocompatibility antigens HLA-DR2 and HLA-DR3 ) Hormonal states (females, pregnancy, delivery)Hormonal states (females, pregnancy, delivery) Drugs (Chlorpromazine, Methyldopa, Hydralazine, Procainamide, Isoniazid, Quinidine)Drugs (Chlorpromazine, Methyldopa, Hydralazine, Procainamide, Isoniazid, Quinidine).")
4
SLE - Pathogenesis Susceptibility genes (usually multiple) + Triggering factors (probably environmental) ABNORMAL IMMUNE RESPONSE
 + Triggering factors (probably environmental) ABNORMAL IMMUNE RESPONSE")
5
SLE - Pathogenesis ABNORMAL IMMUNE RESPONSE Hyperactive Hyperactive Inadequate T cells B cells regulatory mechanism Persistent pathogenic autoantibodies Persistent pathogenic immune complexes Persistent damaging autoreactive T cells

6
SLE - Pathogenesis Pathogenic autoantibodies: 1.Directed to a host of self molecules in the nucleus and cytoplasm of cells, as well as on the cell surface. 2.Able to fix complement. 3.High avidity for the autoantigen present in target tissue.

7
EPIDEMIOLOGY OF SLE Frequency: 14.6/100,000 to 50.8/100,000Frequency: 14.6/100,000 to 50.8/100,000 Incidence: 1.8-7.6/100,000 per yearIncidence: 1.8-7.6/100,000 per year Internationally: worldwideInternationally: worldwide Age: 15-45 yearsAge: 15-45 years Gender: F/M = 9/1Gender: F/M = 9/1 Race: blacks/ whites = 1/4Race: blacks/ whites = 1/4

8
TYPES OF LUPUS Discoid LE/Subacute cutaneous LEDiscoid LE/Subacute cutaneous LE Systemic LESystemic LE Drug-induced LEDrug-induced LE

9
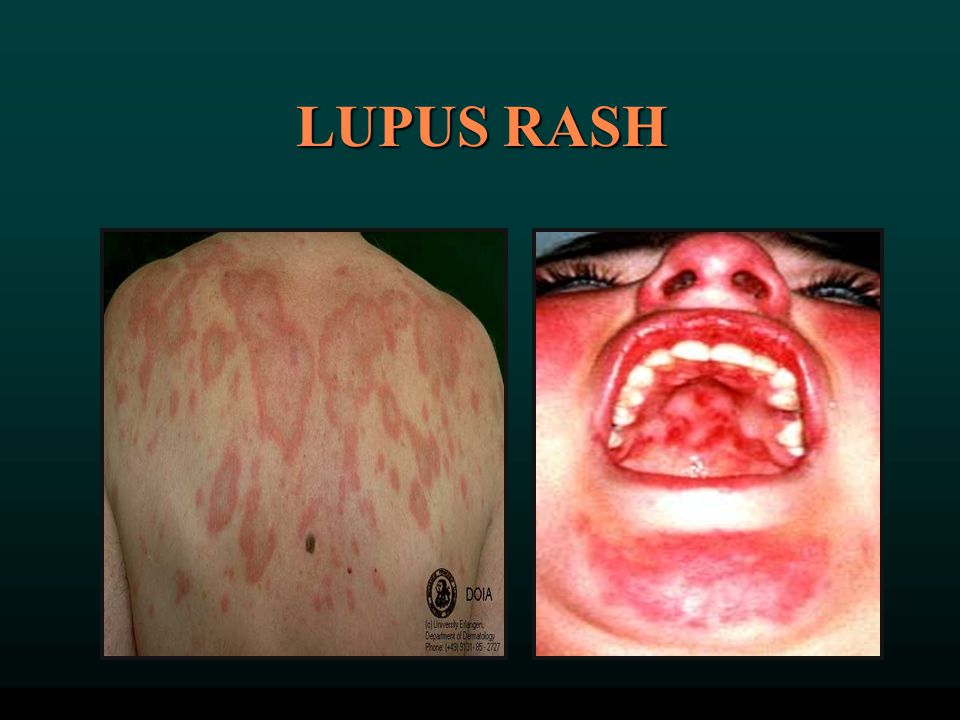
SYMPTOMS OF LUPUS (1) Fever (about 38° C), fatigue, weight loss - 90%Fever (about 38° C), fatigue, weight loss - 90% Arthritis (swollen joints) - 90%Arthritis (swollen joints) - 90% Skin rashes - 74%Skin rashes - 74% Anemia - 71%Anemia - 71% Kidney involvement - 50%Kidney involvement - 50% Pain in the chest on deep breathing (pleurisy) - 45%Pain in the chest on deep breathing (pleurisy) - 45% “Butterfly” rash across the cheeks and nose - 42%“Butterfly” rash across the cheeks and nose - 42%
 Fever (about 38° C), fatigue, weight loss - 90%Fever (about 38° C), fatigue, weight loss - 90% Arthritis (swollen joints) - 90%Arthritis (swollen joints) - 90% Skin rashes - 74%Skin rashes - 74% Anemia - 71%Anemia - 71% Kidney involvement - 50%Kidney involvement - 50% Pain in the chest on deep breathing (pleurisy) - 45%Pain in the chest on deep breathing (pleurisy) - 45% Butterfly rash across the cheeks and nose - 42% Butterfly rash across the cheeks and nose - 42%")
10
SYMPTOMS OF LUPUS (2) Sun sensitivity (photosensitivity) - 30%Sun sensitivity (photosensitivity) - 30% Hair loss - 27%Hair loss - 27% Abnormal blood clotting problems - 20%Abnormal blood clotting problems - 20% Raynaud's phenomenon - 17%Raynaud's phenomenon - 17% Seizures - 15%Seizures - 15% Mouth or nose ulcers - 12%Mouth or nose ulcers - 12%
 Sun sensitivity (photosensitivity) - 30%Sun sensitivity (photosensitivity) - 30% Hair loss - 27%Hair loss - 27% Abnormal blood clotting problems - 20%Abnormal blood clotting problems - 20% Raynaud s phenomenon - 17%Raynaud s phenomenon - 17% Seizures - 15%Seizures - 15% Mouth or nose ulcers - 12%Mouth or nose ulcers - 12%")
11
MALAR RASH

15
DISCOID LUPUS

16
LUPUS RASH

18
VASCULAR SKIN CHANGES RAYNAUD’S PHENOMENON LIVEDO RETICULARIS

19
SLE SKIN PATHOLOGY

21
SEROSITIS IN SLE PLEURITISPERICARDITIS

22
ECHO IN PEICARDITIS PERICARDIAL EFFUSION

23
Lupus Nephritis Word Health Organization (WHO) Classification – based on histology and location of immune complexes. 1.Class I: Normal 2.Class II: Mesangial 3.Class III: Focal and segmental proliferative 4.Class IV: Diffuse proliferative 5.Class V : Membranous 6.Class VI: Sclerosing

24
NEPHRITIS IN SLE

25
EM IN SLE NEPHRITIS

28
LUPUS DIAGNOSTIC CRITERIA (4/11) Malar rashMalar rash Discoid rashDiscoid rash PhotosensitivityPhotosensitivity Oral ulcersOral ulcers Arthritis ( Nonerosive arthritis involving two or more peripheral joints)Arthritis ( Nonerosive arthritis involving two or more peripheral joints) Serositis (Pleuritis or pericarditis )Serositis (Pleuritis or pericarditis ) Renal disorder ( Urine protein > 0.5 gm/day and/or cellular casts)Renal disorder ( Urine protein > 0.5 gm/day and/or cellular casts) Neurologic disorder (Seizures and/or psychosis)Neurologic disorder (Seizures and/or psychosis) Hematologic disorder (Hemolytic anemia or leukopenia (<4000)or lymphopenia (<1500) or thrombocytopenia (< 100,000)Hematologic disorder (Hemolytic anemia or leukopenia (<4000)or lymphopenia (<1500) or thrombocytopenia (< 100,000) Antinuclear antibodyAntinuclear antibody Immunologic disorder (Positive anti ds-DNA test, positiveImmunologic disorder (Positive anti ds-DNA test, positive anti-Sm test, positive anticardiolipin or LAC) anti-Sm test, positive anticardiolipin or LAC)
 Malar rashMalar rash Discoid rashDiscoid rash PhotosensitivityPhotosensitivity Oral ulcersOral ulcers Arthritis ( Nonerosive arthritis involving two or more peripheral joints)Arthritis ( Nonerosive arthritis involving two or more peripheral joints) Serositis (Pleuritis or pericarditis )Serositis (Pleuritis or pericarditis ) Renal disorder ( Urine protein > 0.5 gm/day and/or cellular casts)Renal disorder ( Urine protein > 0.5 gm/day and/or cellular casts) Neurologic disorder (Seizures and/or psychosis)Neurologic disorder (Seizures and/or psychosis) Hematologic disorder (Hemolytic anemia or leukopenia (<4000)or lymphopenia (<1500) or thrombocytopenia (< 100,000)Hematologic disorder (Hemolytic anemia or leukopenia (<4000)or lymphopenia (<1500) or thrombocytopenia (< 100,000) Antinuclear antibodyAntinuclear antibody Immunologic disorder (Positive anti ds-DNA test, positiveImmunologic disorder (Positive anti ds-DNA test, positive anti-Sm test, positive anticardiolipin or LAC) anti-Sm test, positive anticardiolipin or LAC)")
29
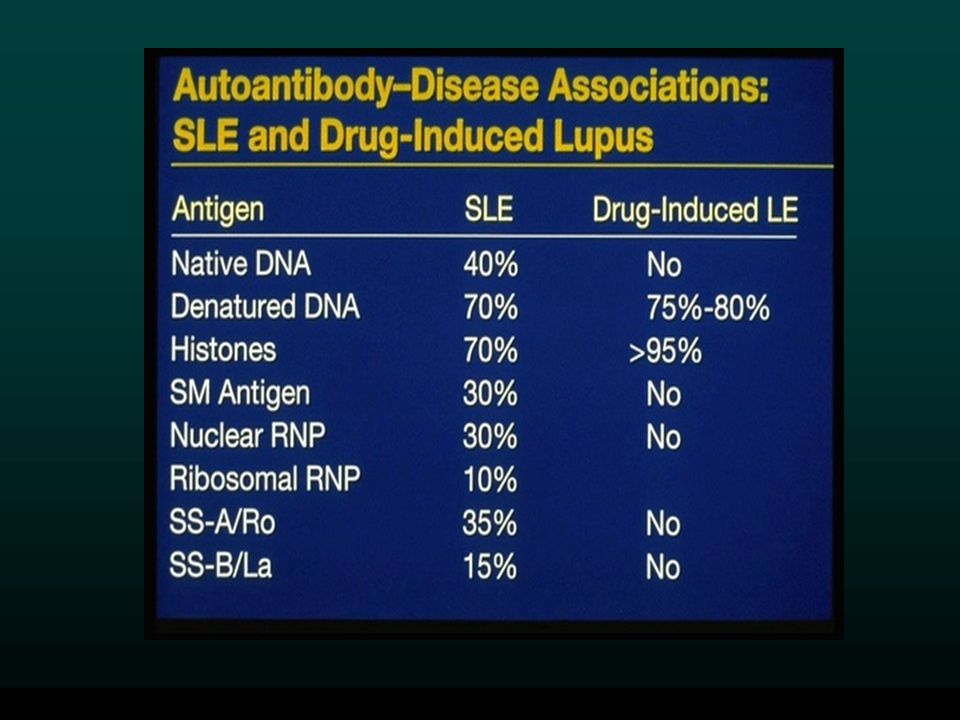
LABORATORY TESTS IN SLE Antinuclear factorAntinuclear factor –Anti ds DNA –Anti Sm –Anti Ro (SS-A) –Anti La (SS-B) False positive VDRLFalse positive VDRL LAC (aPTT)LAC (aPTT) Anticardiolipin (ELISA test of anticardiolipin antibody for IgG, IgM, IgAAnticardiolipin (ELISA test of anticardiolipin antibody for IgG, IgM, IgA
 –Anti La (SS-B) False positive VDRLFalse positive VDRL LAC (aPTT)LAC (aPTT) Anticardiolipin (ELISA test of anticardiolipin antibody for IgG, IgM, IgAAnticardiolipin (ELISA test of anticardiolipin antibody for IgG, IgM, IgA")
30
ANTINUCLEAR ANIBODIES HOMOGENOUS PATTERN SPECKLED PATTERN

31
TREATMENT Non-steroidal Anti-inflammatory Drugs (NSAIDs) including COX 2Non-steroidal Anti-inflammatory Drugs (NSAIDs) including COX 2 Corticosteroids (Prednisone, Solomedrol)Corticosteroids (Prednisone, Solomedrol) Antimalarials (Hydroxychloroquine)Antimalarials (Hydroxychloroquine) Immunomodulating Drugs (Imuran, Endoxan, Methotrexate)Immunomodulating Drugs (Imuran, Endoxan, Methotrexate) Anticoagulants (Aspirin, Coumadine)Anticoagulants (Aspirin, Coumadine)
 including COX 2Non-steroidal Anti-inflammatory Drugs (NSAIDs) including COX 2 Corticosteroids (Prednisone, Solomedrol)Corticosteroids (Prednisone, Solomedrol) Antimalarials (Hydroxychloroquine)Antimalarials (Hydroxychloroquine) Immunomodulating Drugs (Imuran, Endoxan, Methotrexate)Immunomodulating Drugs (Imuran, Endoxan, Methotrexate) Anticoagulants (Aspirin, Coumadine)Anticoagulants (Aspirin, Coumadine)")
32
PREGNANCY AND LUPUS Increased risk of disease activity during or immediately after (3 to 4 weeks) pregnancyIncreased risk of disease activity during or immediately after (3 to 4 weeks) pregnancy Antiphospholipid antibodies pose a particular risk of miscarriagesAntiphospholipid antibodies pose a particular risk of miscarriages Congenital SLE (positive aRo/aLa mothers):Congenital SLE (positive aRo/aLa mothers): –Congenital heart block –Rash/photosensitivity –Thrombocytopenia
 pregnancyIncreased risk of disease activity during or immediately after (3 to 4 weeks) pregnancy Antiphospholipid antibodies pose a particular risk of miscarriagesAntiphospholipid antibodies pose a particular risk of miscarriages Congenital SLE (positive aRo/aLa mothers):Congenital SLE (positive aRo/aLa mothers): –Congenital heart block –Rash/photosensitivity –Thrombocytopenia")
33
PROGNOSIS Mortality:Mortality: –10-year survival rates ranging from 75-85% –> 90% of patients surviving more than 5 years Early deaths:Early deaths: –Infection –Active disease –Thrombosis –Renal failure Late complications:Late complications: –Atherosclerosis –Osteoporosis –Avascular bone necrosis –Dementia

34
Drug induced lupus More common in men than women. Fatigue, fever, arthralgia and pleuropericardial disease are common. CNS and renal disease are very rare. The clinical disease disappears after withdrawal of the drug. Anti-histone antibodies are found in 95% of cases.

37
ANTI-PHOSPHOLIPID SYNDROME Thrombotic complications: deep venous thrombosis, stroke, gangrene, heart attack, Libman-Sacks’ endocarditisThrombotic complications: deep venous thrombosis, stroke, gangrene, heart attack, Libman-Sacks’ endocarditis MiscarriagesMiscarriages Thrombocytopenia (low platelets count)Thrombocytopenia (low platelets count) Blood clotting abnormalities (lupus anticoagulant and anticardiolipin antibody)Blood clotting abnormalities (lupus anticoagulant and anticardiolipin antibody) 8 to 65 percent of people with lupus have the lupus anticoagulant, and 25 to 61 percent have anticardiolipin antibody
Thrombocytopenia (low platelets count) Blood clotting abnormalities (lupus anticoagulant and anticardiolipin antibody)Blood clotting abnormalities (lupus anticoagulant and anticardiolipin antibody) 8 to 65 percent of people with lupus have the lupus anticoagulant, and 25 to 61 percent have anticardiolipin antibody")
Similar presentations








>")
. Definition Epidemiology Pathophysiology Clinical features Classification and diagnosis Treatment Prognosis Lupus related syndromes.>")


>")











