Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم

2
By Mohammad Ashraf Balbaa, MD Associate Professor of Surgery
Venous Thrombosis By Mohammad Ashraf Balbaa, MD Associate Professor of Surgery

3
Intrinsic pathway XII XIIa Extrinsic pathway XI XIa IX IXa VIIa VII X
HMW kininogen Prekallikerin XII XIIa HMW kininogen Extrinsic pathway XI XIa TPL IX IXa VIIa VII PL Ca++ VIIIa VIII PL Ca++ TPL X Xa PL Ca++ Va V Prothrombin Thrombin Fibrinogen Fibrin Ca++ XIII XIIIa

4
Definition: A venous thrombus is the formation of a semi-solid coagulum within flowing blood in the venous system.

5
Venous Thrombosis Types: Superficial Thrombophlebitis
Deep vein thrombosis

7
SUPERFICIAL THROMBOPHLEBITIS
The term “Superficial Thrombophlebitis” is customarily applied to any kind of thrombotic process in the superficial venous system. However, it implies existence of an inflammatory component, which is not always present.

8
SUPERFICIAL THROMBOPHLEBITIS
Definition: Localized inflammation of the vein wall + thrombus formation in the lumen

9
SUPERFICIAL THROMBOPHLEBITIS
Etiology: Direct trauma. A direct blow over a superficial vein can result in phlebitis. Venous intimal damage Infusion of hypertonic solutions, injurious compounds as antibiotics & chemotherapeutic agents and I.V. drug abuse. Cannula insertion. N.B. Traumatic thrombophlebitis can be put to clinical use in the form of sclerotherapy.

10
SUPERFICIAL THROMBOPHLEBITIS

11
SUPERFICIAL THROMBOPHLEBITIS
Clinical Picture: The vein becomes painful, tender, firm & cord-like. The overlying skin becomes dusky & edematous.

12
SUPERFICIAL THROMBOPHLEBITIS
Clinical Picture: Embolization is rare as the thrombus is firmly adherent Sometimes, it is accompanied with DVT, especially if there is marked edema that can not be explained by simple or superficial phlebitis alone.

13
SUPERFICIAL THROMBOPHLEBITIS

14
SUPERFICIAL THROMBOPHLEBITIS

15
SUPERFICIAL THROMBOPHLEBITIS
Treatment: Prevention: The best R/ for traumatic thrombophlebitis is prevention by: Rotating IV sites every 3 days & changing IV tubing regularly under sterile conditions Diluting irritant infusions.

16
SUPERFICIAL THROMBOPHLEBITIS
Treatment: Conservative Measures : Rest & elevation + elastic bandage. Warm compresses + non-steroidal anti-inflammatory drugs (NSAIDs) or aspirin. antibiotics.
 or aspirin. antibiotics.")
17
SUPERFICIAL THROMBOPHLEBITIS
Treatment: Surgical Measures: If the thrombus propagates e.g. in the long saphenous vein above the knee ligation of the sapheno-femoral junction, under local anesthesia. Excision, in recurrent & symptomatizing phlebitis.

18
Venous Thrombosis Types: Superficial Thrombophlebitis
Deep vein thrombosis

19
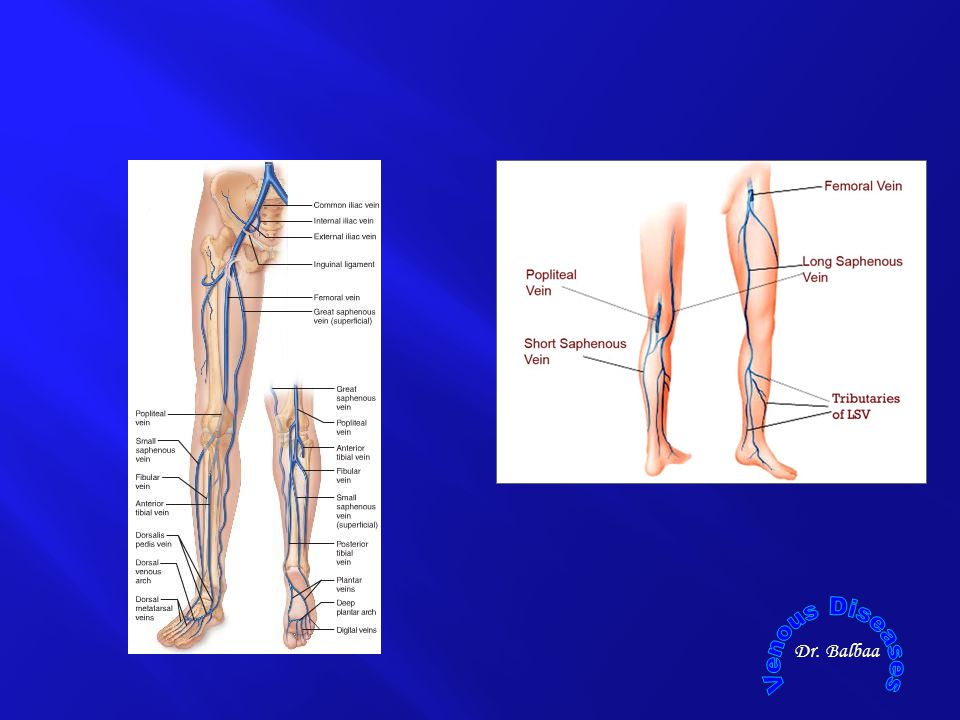
Deep Vein Thrombosis Incidence: Prevalence Site Side
Occurs for the first time in about 100 persons per 100,000 each year in the United States. This incidence increases with increasing age. The recurrence rate with anticoagulation has been noted to be 6% to 7% in the ensuing 6 months.

20
Deep Vein Thrombosis Incidence: Prevalence Site Side Upper limb:
Axillary vein thrombosis. Lower limb: venous plexus calf vein thrombosis. Ilio-femoral thrombosis (phlegmasia alba dolens PAD). Ilio-frmoral thrombosis + deep pelvic vien thrombosis (phegmasia cerulae dolans PCD).
. Ilio-frmoral thrombosis + deep pelvic vien thrombosis (phegmasia cerulae dolans PCD).")
21
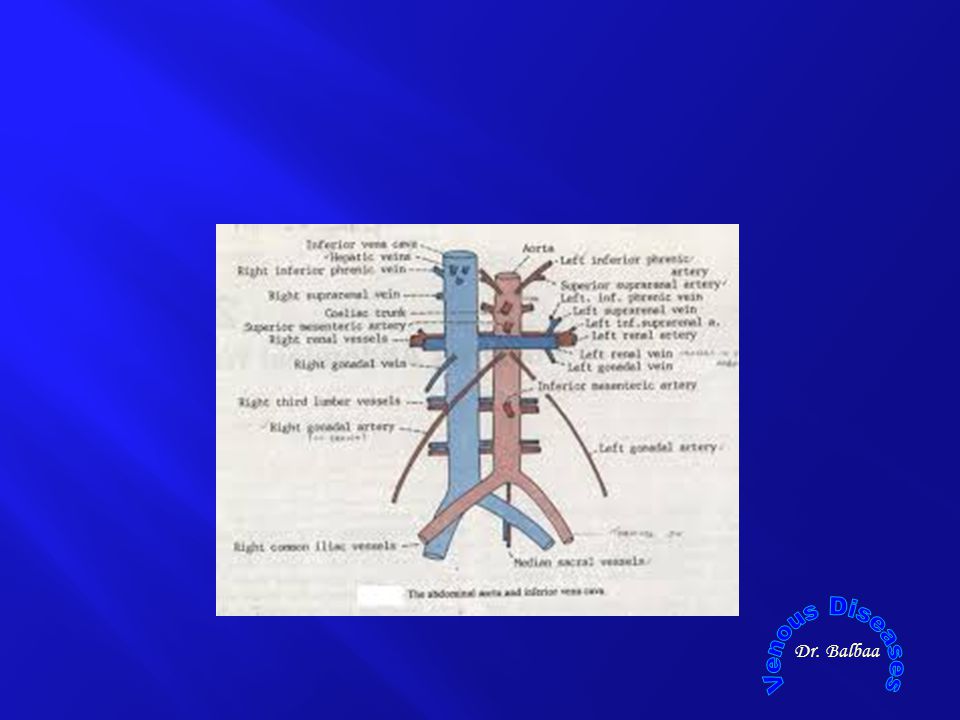
Deep Vein Thrombosis Incidence: Prevalence Site Side
Ilio-femoral thrombosis occurs on the left side > right (3:1) due to: It is more liable to be compressed by the overlying right common iliac artery against L5 Left iliac vein is longer than the right.
 due to: It is more liable to be compressed by the overlying right common iliac artery against L5. Left iliac vein is longer than the right.")
23
Deep Vein Thrombosis Etiology A triad (posited by Virchow in 1856):
Stasis Intimal damage Hypercoagulability 1821 -1902

24
Deep Vein Thrombosis Etiology A triad (posited by Virchow in 1856):
STASIS Intimal damage Hypercoagulability

25
Virchow Triad STASIS: Stasis in the lower limb is associated with:
Immobilization during anesthesia, after trauma and fractures, post operative recumbency & serious illness. Diminished cardiac function (heart failure). Previous DVT: cannot maintain uni-directional venous flow due to valvular incompetence.
. Previous DVT: cannot maintain uni-directional venous flow due to valvular incompetence.")
26
Deep Vein Thrombosis Etiology A triad (posited by Virchow in 1856):
Stasis INTIMAL DAMAGE Hypercoagulability

27
Virchow Triad INTIMAL DAMAGE It caused by: Trauma & fractures.
Infusions. Infection & toxemia.

28
Deep Vein Thrombosis Etiology A triad (posited by Virchow in 1856):
Stasis Intimal damage HYPERCOAGULABILITY

29
Virchow Triad HYPERCOAGULABILITY 1ry or familial causes:
Anti-thrombin III deficiency Protein S or C deficiency

30
Virchow Triad HYPERCOAGULABILITY 2ry or acquired causes:
Malignancy, dehydration, toxemia and sepsis, polycythemia, D.M., smoking, pregnancy & post partum state.

31
Deep Vein Thrombosis RISK FACTORS Patient factors
Disease or surgical procedure Age ≥ 60 yr Obesity Immobility Pregnancy Puerperium High-dose estrogen therapy Previous deep vein thrombosis or pulmonary embolism

32
Deep Vein Thrombosis RISK FACTORS Patient factors
Disease or surgical procedure Trauma or surgery, especially of procedure pelvis, hip and lower limb Malignancy, Heart failure Paralysis of lower limb(s) Polycythaemia
 Polycythaemia.")
33
Deep Vein Thrombosis PATHOGENESIS 1ry platelet thrombus
Mural Coralline thrombus Occluding thrombus Consecutive clot Propagated clot coralline

34
Deep Vein Thrombosis PATHOGENESIS 1ry platelet thrombus
Mural Coralline thrombus Occluded thrombus Consecutive clot Propagated clot

35
Deep Vein Thrombosis Pathophysiology

36
Pathophysiology Point of Difference Thrombophlebitis Phlebothrombosis
Major cause: Clinical Presentation: Size of propagated clot: Emboli: Inflammation of the vein wall Pain + signs of inflammation Short & fixed Less liable to embolization. Stasis & hypercoagulability Silent few signs & symptoms Large & easy detachable More liable to embolization.

37
Deep Vein Thrombosis CONSEQUENCES OF THROMBOSIS

38
CONSEQUENCES OF THROMBOSIS
Locally Distally Proximally

39
CONSEQUENCES OF THROMBOSIS
LOCALLY Lysis: Results from fibrinolytic action of blood Organization and fibrosis: → retraction post-phlebitic leg (CVI), i.e. recanalization with valve destruction Infection: High virulence organisms → septic emboli.
, i.e. recanalization with valve destruction. Infection: High virulence organisms → septic emboli.")
40
CONSEQUENCES OF THROMBOSIS
Distally: A varying degree of edema after which venous collateral circulation soon opens up tortuous superficial veins, i.e. 2ry VV. Phlegmasia alba and cerula. Post-phlebetic syndrome

41
CONSEQUENCES OF THROMBOSIS
Proximally: Detachment pulmonary embolism pulmonary infarction up to death.

42
Deep Vein Thrombosis CLINICAL PICTURE

43
CLINICAL PICTURE CLINICAL PRESENTATION
DVT can be completely asymptomatic in about 30-50% of cases. Passed unnoticed Detectable PE, which may be sometimes fatal. Low grade fever which fails to settle after operation. By the occurrence of local signs of in the limb.

44
CLINICAL PICTURE Swelling the extent of which depends on the site of the thrombus → (frog-leg position): Leg is externally rotated The knee is flexed)
")
45
CLINICAL PICTURE Aching pain and heaviness on moving the calf and thigh. Tenderness on pressure on the instep of the sole of the foot and along the affected veins.

46
CLINICAL PICTURE Increase warmth of the affected limb.
Varicose veins due to distension of the superficial veins (late sign).
.")
47
CLINICAL PICTURE Certain tests: Homan's sign:
Dorsiflexion of the foot → resistance or pain of the calf muscles to forcible dorsiflexion – is not discriminatory and should be abandoned.

48
CLINICAL PICTURE Certain tests: Pratt's sign: Moses's sign:
Compression of the calf against tibia → pain. Moses's sign: Compression of the calf from side to side → pain.

49
CLINICAL PICTURE Phlegmasia alba (white) dolens (pain)
(White Leg; Milk Leg) Phlegmasia cerulae (blue) dolens
 Phlegmasia cerulae (blue) dolens.")
50
Phlegmasia Cerulae Dolens

51
Venous gangarene

52
DEEP VEIN THROMBOSIS COMPLICATIONS

53
COMPLICATIONS 2ry varicose veins: Venous gangrene: Pulmonary embolism:
2ry collaterals develop when the deep system is occluded. Venous gangrene: In PCD. Pulmonary embolism: When a thrombus becomes dislodged form its attachment to the venous wall & is carried into the pulmonary arteries

54
DEEP VEIN THROMBOSIS INVESTIGATIONS:

55
INVESTIGATIONS NON INVASIVE INVESTIGATIONS Doppler Ultrasonography
Duplex Imaging Doppler Color Flow. Magnetic Resonance Venography (MRV) Magnetic Resonance Venography (MRV): It has demonstrated excellent sensitivity in the diagnosis of proximal venous thrombosis. It has the disadvantage of availability, cost, metallic implants, claustrophobia.
 Magnetic Resonance Venography (MRV): It has demonstrated excellent sensitivity in the diagnosis of proximal venous thrombosis. It has the disadvantage of availability, cost, metallic implants, claustrophobia.")
56
INVESTIGATIONS NON INVASIVE INVESTIGATIONS Blood Tests
Breakdown products of complexed fibrin (fibrin acted on by factor XIII) generated during physiologic fibrinolysis (D-Dimer). A negative D-dimer test in patients with suspected DVT has a high negative predictive value. A normal D-dimer reliably excludes DVT.
 generated during physiologic fibrinolysis (D-Dimer). A negative D-dimer test in patients with suspected DVT has a high negative predictive value. A normal D-dimer reliably excludes DVT.")
57
DEEP VEIN THROMBOSIS MANAGEMENT : Prophylaxis of DVT
Treatment of established DVT Conservative (non-operative) treatment Operative surgical treatment
 treatment. Operative surgical treatment.")
58
MANAGEMENT PROPHYLAXIS OF DVT Preoperative measures:
Mechanical prophylaxis: Elastic compression stockings. Intermittent pneumatic compression (IPC) devices:
 devices:")
59
MANAGEMENT PROPHYLAXIS OF DVT Preoperative measures:
Pharmacologic prophylaxis: Low-dose unfractionated heparin: 5000 unites, CS, beginning 2 hours preoperatively Low-molecular weight heparin (LMWH): Dose is drug dependent, SC, twice daily, no monitoring or dose adjustment.
: Dose is drug dependent, SC, twice daily, no monitoring or dose adjustment.")
61
MANAGEMENT PROPHYLAXIS OF DVT Operative measures:
Reduction of trauma to the calf muscles during surgery; the operating table should be well padded to decrease the pressure on the buttocks, calves and heel. Elevation and massage of the leg at the end of the operation is a good plan.

62
MANAGEMENT PROPHYLAXIS OF DVT Postoperative measures:
Early ambulation after surgery. Maintenance of adequate hydration. Pharmacologic prophylaxis. Daily examination of the calves & feet for local signs of thrombosis & on suspicion or history, anticoagulants should be considered.

63
DEEP VEIN THROMBOSIS MANAGEMENT : Prophylaxis of DVT
Treatment of established DVT Conservative (non-operative) treatment Operative surgical treatment
 treatment. Operative surgical treatment.")
64
Non-operative Treatment
Bed rest and foot elevation Anti-coagulants Thrombolytic (fibrinolytic) & defibrinating agents Post treatment compression to control leg edema:
 & defibrinating agents. Post treatment compression to control leg edema:")
65
Anticoagulants 1. Parentral (Heparin) 2. Oral (Dendivan)
Dose and duration ,000 units/6 hours, 7 days, in calf thrombosis and for 14 days in Iliofemoral thrombosis. Low dose MW: 1 mg/kg/12 hrs. 3 tablets/day reduced to 2 tabs, then one tab for 6 months, started before we stop heparin by 3 days (as it takes 3 days to start its action)
")
66
Non-operative Treatment
Bed rest and foot elevation Anti-coagulants Thrombolytic (fibrinolytic) & defibrinating agents Post treatment compression to control leg edema:
 & defibrinating agents. Post treatment compression to control leg edema:")
67
Thrombolytic Treatment
Tissue palsmingen activators : streptokinase & human urokinase.

68
Thrombolytic Treatment
Indications: Most effective when given to thrombi of 5-7 days duration. For patients whose clot extends proximally beyond the origin of the deep femoral vein.

69
THANK YOU

Similar presentations





 in a deep vein, usually in the legs, which partially or completely.>")





 around valves propagation Virchow’s triad.>")








