Download presentation
Presentation is loading. Please wait.

1
The Etiology of Human Congenital Heart Defects Literature Seminar Feb 19 2009 Bernard Thienpont

2
Congenital Heart Defect structural anomaly of the heart, present at birth not necessarily manifest in the neonatal period can remain benign throughout life

3
Congenital Heart Disease Congenital heart defect (Congenital) Cardiomyopathy(Congenital) Rhythm Disturbance
 Cardiomyopathy(Congenital) Rhythm Disturbance")
4
Congenital Heart Disease Congenital heart defect (Congenital) CardiomyopathyCongenital Rhythm Disturbance A = Secondary to B
 CardiomyopathyCongenital Rhythm Disturbance A = Secondary to B")
5
Congenital Heart Disease Congenital heart defect (Congenital) CardiomyopathyCongenital Rhythm Disturbance A & B share an underlying cause (same gene independently associated with both) NKX2.5 ACTC
 CardiomyopathyCongenital Rhythm Disturbance A & B share an underlying cause (same gene independently associated with both) NKX2.5 ACTC")
6
Heart formation 1. heart field specification

8
van Wijk, Moorman & van den Hoff, 2006

11
Heart formation 2. Heart tube formation

12
Moorman & VandenBerg, 2009

14
Concomitant neural crest induction

15
Heart formation 3. Heart chamber formation

16
Moorman & VandenBerg, 2009

17
Black, 2007

21
http://pie.med.utoronto.ca/HTBG/HTBG_content/HTBG_heartEmbryologyApp.html

22
Different chamber identities

23
Heart formation 4. Outflow tract septation

25
Black, 2007 Semin Cell Dev Biol. 2007 February; 18(1): 101–110
: 101–110")
26
Black, 2007 Semin Cell Dev Biol. 2007 February; 18(1): 101–110
: 101–110")
27
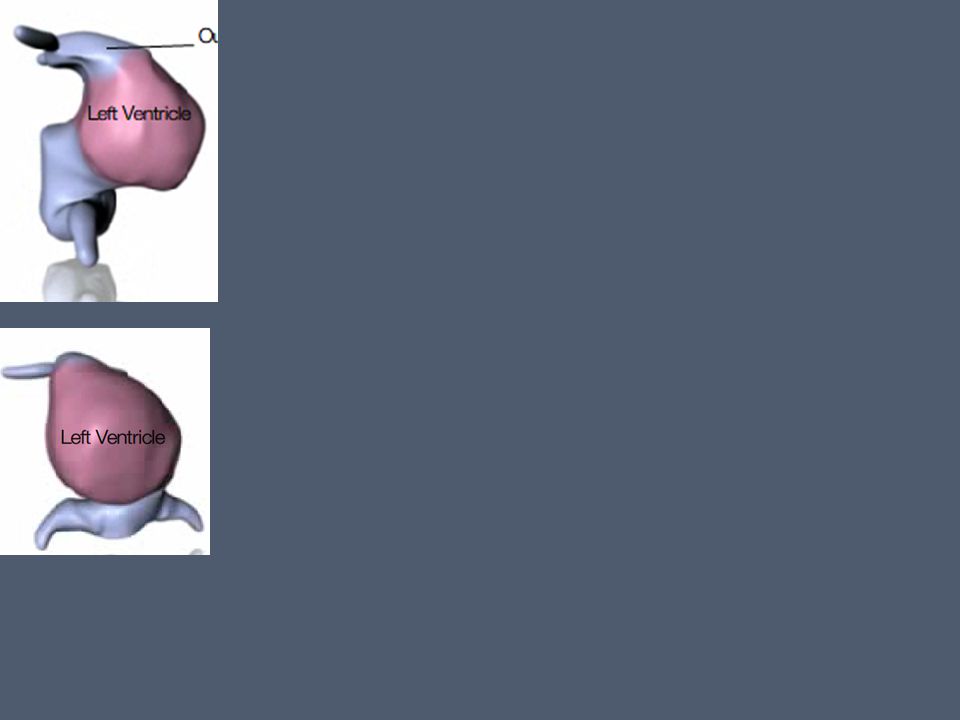
Heart formation 5. Ventricular septation

29
Cai et al, nature 2008

30
Heart formation 5. Atrial septation

33
CHDs: Classifications Why? Many CHDs are complex Different patients can have similar CHDs to a varying extent

34
CHDs: Classifications Anatomical: Group CHDs that affect the same cardiac structure e.g. AEPC Abnormalities of : Position and connection of heart Tetralogy of Fallot and variants Great veins atriums and atrial septum AV valves and AV septal defect Ventricles and ventricular septum VA valves and great arteries Coronary arteries, arterial duct and pericardium Embryological: Group CHDs that are caused by the same embryological problem e.g. Boughman et al., AJMG 1987 Abnormalities because of Cell migration problems Flow lesions Cell death Extracellular matrix Targeted growth defects other

35
e.g. VSD Anatomical: Group CHDs that affect the same cardiac structure e.g. AEPC Abnormalities of : Position and connection of heart Tetralogy of Fallot and variants Great veins atriums and atrial septum AV valves and AV septal defect Ventricles and ventricular septum VA valves and great arteries Coronary arteries, arterial duct and pericardium Embryological: Group CHDs that are caused by the same embryological problem e.g. Boughman et al., AJMG 1987 Abnormalities because of Cell migration problems VSD-I Flow lesions VSD-II Cell death VSD-III Extracellular matrix VSD-IV Targeted growth defects other

36
Frequency of CHDs Hoffman & Kaplan (2002)
")
37
Clinical classification Isolated vs syndromic CHDs ? Second major malformation ? Dysmorphism (3 or more minor malformations) Δ etiology: Mostly multifactorial vs single (genetic) cause
 Δ etiology: Mostly multifactorial vs single (genetic) cause.")
38
Syndromic vs isolated CHDs Greenwood (1975) & Pradat et al. (2003)
 & Pradat et al. (2003)")
39
Causes of CHDs Environmental or genetic?

40
Environmental causes Teratogens – Alcohol – α-epileptica PKU

41
Environmental causes Teratogens PKU Viral infections?

42
Environmental causes Teratogens PKU Viral infections Pregestational diabetes DiabeticNon-diabetic CVM221417 Normal587190592 3.61%0.74% Major CHDs: TGA PTA AVSD

43
Environmental causes Teratogens PKU Viral infections Pregestational diabetes Twinning

44
~ chorionic & amniotic structures: DC/DA 1%

45
Twinning ~ chorionic & amniotic structures: DC/DA 1% MC/DA 5-7% (concordance = 25-50%) TTT: 8% vs 3.4%
 TTT: 8% vs 3.4%")
46
Twinning ~ chorionic & amniotic structures: DC/DA 1% MC/DA 5-7% (concordance = 25-50%) MC/MA 28% (often right atrial isomerism)
 MC/MA 28% (often right atrial isomerism)")
47
Twin studies Problematic MZ : 25-50% concordance DZ : 13% concordance discordance? – Postzygotic mutations – Epigenetic Δ (e.g. X inactivation) – Stochastic factors Catastrophic Chance – …
 – Stochastic factors Catastrophic Chance – ….")
48
Genetic causes x1.3 x4.3 x5 Population risk = 0.8% Relative risk:

49
Genetic causes Familial aggregation Excluding BAV

50
Genetic causes CHD Frequency in parents of CHD children

51
Genetic causes CHD frequency in children of CHD parents

52
Genetic causes Familial aggregation: caveats – Ascertainment bias – Mailing questionairs – Inclusion criteria – Classification differences

53
Genetic causes Increased transmission of CHD via mother > Male susceptibility Mitochondrial? Imprinting

54
Classification of genetic causes genetic lesion small mutations ↔ chromosomal aberrations inheritance pattern AD, AR, XL, other pathogenic mechanism of the mutation Loss-of-function, gain-of-function, dominant-negative number of loci involved: monogenic, oligogenic, polygenic

55
genetic lesion small mutations ↔ chromosomal aberrations Based on detection technique Distinction = blurring

56
genetic lesion small mutations Syndromic / isolated De novo / familial Monogenic Frequent SNPs – ELN – CREBBP – NKX2-5 chromosomal aberrations Syndromic (± 55% of sCHD) de novo Often contiguous gene syndromes ID = diagnosis – AVSD in T21 – ASD, VSD, PS in 4p- – aortic abnormalities in 45,X
 de novo Often contiguous gene syndromes ID = diagnosis – AVSD in T21 – ASD, VSD, PS in 4p- – aortic abnormalities in 45,X")
57
Inheritance pattern: AD 37/51 genes that are associated with CHDs – 22/37 loss of function signaling molecules transcription factors Transcription modulators – Dominant-negative Alagille (JAGGED1) Structural proteins (MYH6, MYH11, ACTC1, …) – Gain-of-function Noonan/CFC/Costello Rarely: TBX5, TBX1
 Structural proteins (MYH6, MYH11, ACTC1, …) – Gain-of-function Noonan/CFC/Costello Rarely: TBX5, TBX1")
58
Inheritance pattern: XL 6/51: XL All but ZIC3: syndromic Turner (45,X) 40%: CVM (L-OFT abn: Coarc, AS, HLH) Etiology? Pre-X-inactivation? Unlikely PAR? 10% of genes escape X-inactivation

59
Inheritance pattern: XL male preponderance:

60
The number of loci relative risk & effect size population frequency monogenic oligogenic polygenic

61
Monogenic Most mutations causing iCHDs high penetrance ascertainment bias !! most genes: linkage studies (necessarily high penetrance)
.")
62
Monogenic Variable penetrance & expressivity Due to Type of mutation (eg TBX5) Modifiers eg VEGF polymorphisms in del22q11 + CHD CRELD1 mutations in T21 + AVSD
 Modifiers eg VEGF polymorphisms in del22q11 + CHD CRELD1 mutations in T21 + AVSD")
63
Monogenic Variable penetrance & expressivity YET: Typical CHDs eg AVSD in T21 conotruncul malformations in del22q11 Familial CHDs: high concordance

64
Oligogenic No segregation of mutation with phenotype Rare & unique mutations Gene ID: candidate gene approach Sequencing patients and normal controls Functional studies

65
Oligogenic e.g. FOXH1, GDF1, CFC1 and TDGF1: 27/375 patients carry a mutation vs 0/125 control

66
Oligogenic Functional studies

67
Polygenic SNPs that predispose to CHDs Different constellations: – Polymorphism in cis on same allele eg T21 – Polymorphism in cis on other allele eg del22q11: no SNPs in TBX1 are associated with CHDs (Rauch 2004) – Polymorphism in trans VEGF in 22q11
 – Polymorphism in trans VEGF in 22q11")
68
Polygenic Low effect size likely environmental contribution Multifactorial (genes + environment) e.g. SNP in NNMT risk does not increase significantly low Nicotamide intake risk does not increase significantly SNP in NNMT + low Nicotamide intake significantly increased risk

69
Gene identification: Challenges Large cohort of different types of CHD Sequence patients and controls (1000 genomes) Include CNV analysis Functional studies to prove pathogenic nature Link between CHD and defect in heart formation is often unclear
 Include CNV analysis Functional studies to prove pathogenic nature Link between CHD and defect in heart formation is often unclear")
Similar presentations














>")















