Download presentation
Presentation is loading. Please wait.

1
Pulmonary Embolism & Pulmonary Infarction
Dr. Muhammad Atif Qureshi MBBS, FCPS Associate Professor - Medicine

3
Pulmonary Embolism, Infarction
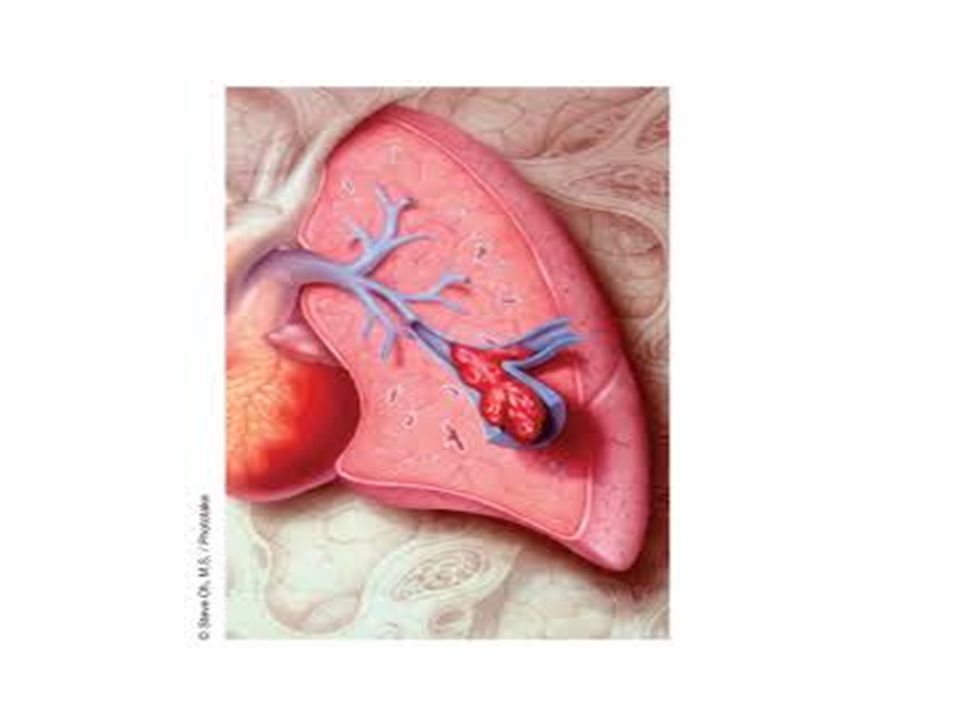
Embolism : Impaction of a thrombus or foreign matter in the pulmonary vascular bed. Infarction : The pathological changes which develop in the lung as a result of pulmonary embolism.

4
Pulmonary Embolism, Infarction
Thrombosis of peripheral veins , embolization of pulmonary arteries , and pulmonary infarction. Primary thrombosis in pulmonary arteries and veins

5
EMBOLISM Thrombotic Non-thrombotic : Fat, Air, Tumour , Amniotic fluid, IV Drug abusers.

6
Risks Decrease in blood flow below a certain critical level.
Increase in coagulability of blood. Damage of the vessel wall.

7
RISK FACTORS Bed rest Post-operative
After severe blood loss and trauma CCP CHF Varicose veins Advancing age Obesity Post-partum Malignancy DM Pneumonia Debilitating diseases 1ry polycythemia Race, Diet

8
Clinical features Depends on :
Size of the embolus and blood vessel occluded. State of the lung. Associated disease(s).
.")
9
Massive PE CLINICAL SETTING ELDERLY,POSSIBLY OBESE
AROUND THE 10th DAY POST-OP. CALLING FOR BED-PAN EXPIRING SUDDENLY OR WHILE IN THE ACT OF DEFECATION IMMEDIATELY FATAL,2/3 DIE IN THE FIRST TWO HOURS

10
Massive PE SHOCK DYSPNEA APPREHENSION TACHYCARDIA SWEATING CHEST PAIN
FAINTNESS CYANOSIS AF COLLAPSE

14
PULMONARY EMBOLISM PE is the most common preventable cause of death in hospitalized patients ~600,000 deaths/year 80% of pulmonary emboli occur without prior warning signs or symptoms 2/3 of deaths due to pulmonary emboli occur within 30 minutes of embolization Death due to massive PE is often immediate Diagnosis can be difficult Early treatment is highly effective

16
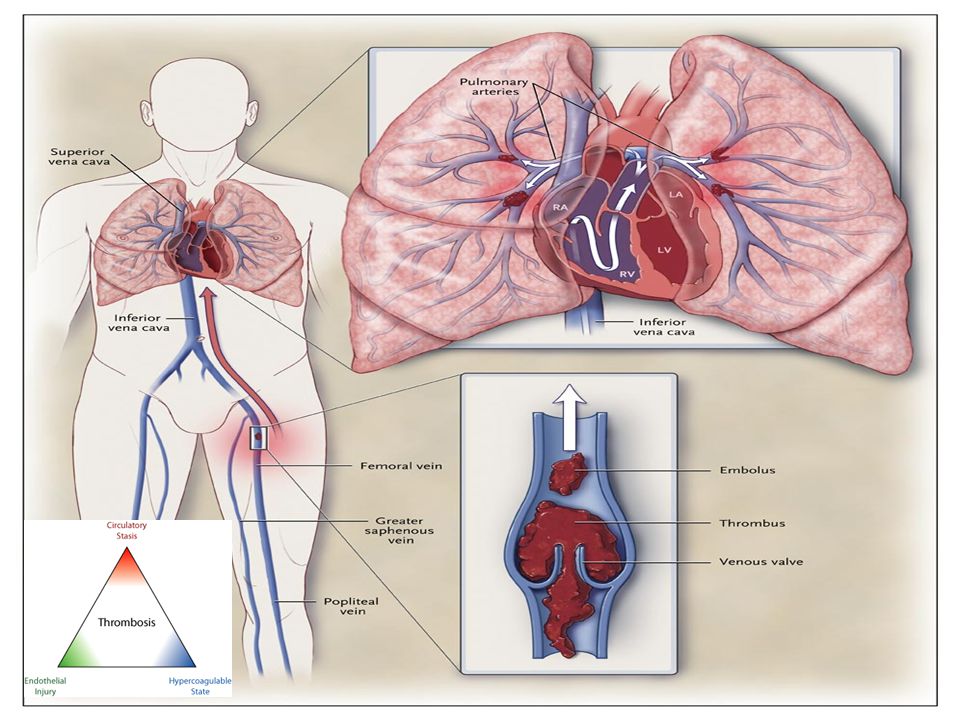
At least 90% of pulmonary emboli originate from major leg veins.

17
Natural History of pe 40-50% of pts with DVT develop PE, often “silent” PE presents 3-7 days after DVT Fatal within 1 hour after onset of respiratory symptoms in 10% Shock/persistent hypotension in 5-10% (up to 50% of patients with RV dysfunction) Most fatalities occur in untreated pts Perfusion defects completely resolve in 75% of all patients (who survive)
 Most fatalities occur in untreated pts. Perfusion defects completely resolve in 75% of all patients (who survive)")
18
Clinical Presentation
Dyspnea, tachypnea, or pleuritic chest pain most common Pleuritic pain : distal emboli pulmonary infarction and pleural irritation Isolated dyspnea of rapid onset: central PE with hemodynamic sequlea Retrosternal angina like sxs: RV ischemia Syncope:rare presentation, but indicates severely reduced hemodynamic reserve Symptoms can develop over weeks In pts with pre-existing CHF or COPD, worsening dyspnea may indicate PE

20
Clinical Diagnosis of PE
In summary, clinical signs, symptoms and routine tests do not allow for the exclusion or confirmation of acute PE but may increase the index of its suspicion Consider PE in cases of unexplained tachycardia or syncope

21
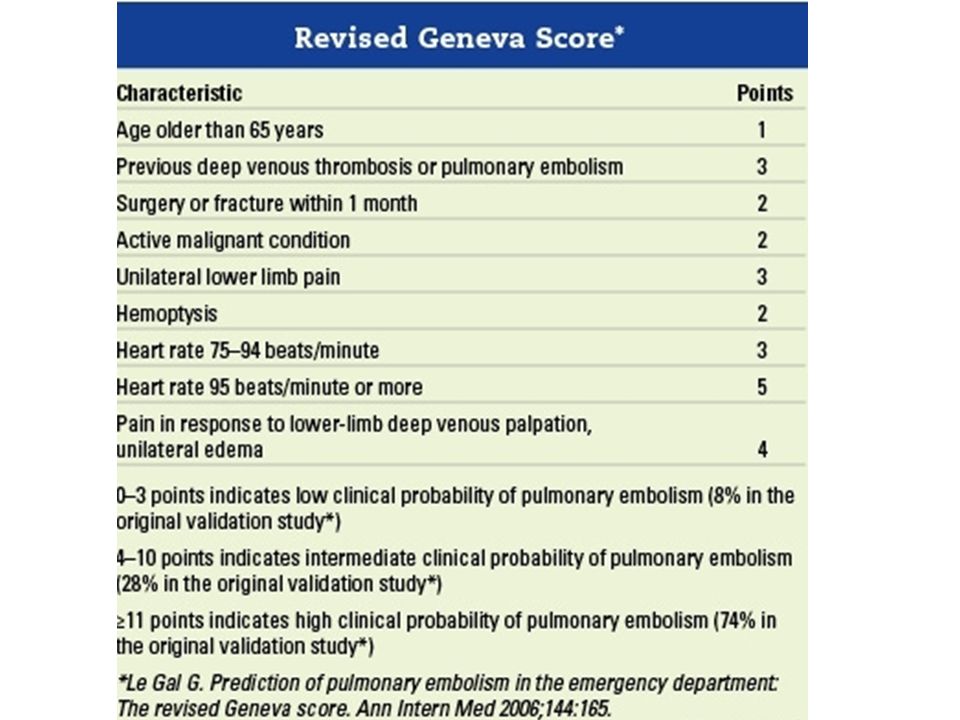
Diagnosis-Probability Assessment
Implicit clinical judgement is fairly accurate: “Do you think this patient has a PE?” Validated prediction rules standardize clinical judgement Wells Geneva

22
Proportion with PE 65% 30 10%

25
Non-Specific!!

26
Chest X-Ray Usually abnormal, but non-specific
Study of 2,322 patients with PE: Cardiac enlargement (27%) Normal (24%) Pleural effusion (23%) Elevated hemidiaphragm (20%) Pulmonary artery enlargement (19%) Atelectasis (18%) Parenchymal pulmonary infiltrates (17%) Chest Radiographs in Acute Pulmonary Embolism: Results From the International Cooperative Pulmonary Embolism Registry. Chest July :3338; /chest
 Normal (24%) Pleural effusion (23%) Elevated hemidiaphragm (20%) Pulmonary artery enlargement (19%) Atelectasis (18%) Parenchymal pulmonary infiltrates (17%) Chest Radiographs in Acute Pulmonary Embolism: Results From the International Cooperative Pulmonary Embolism Registry. Chest July :3338; /chest")
27
ECG Usually non-specific ST/T waves changes and tachycardia
RV strain patterns suggest severe PE Inverted T waves V1-V4 QR in V1 Incomplete RBBB S1Q3T3

28
S1Q3T3 and T wave changes

30
Other tests Most patients with PE have a normal pulse oximetry
A-a gradient is insensitive and non-specific

31
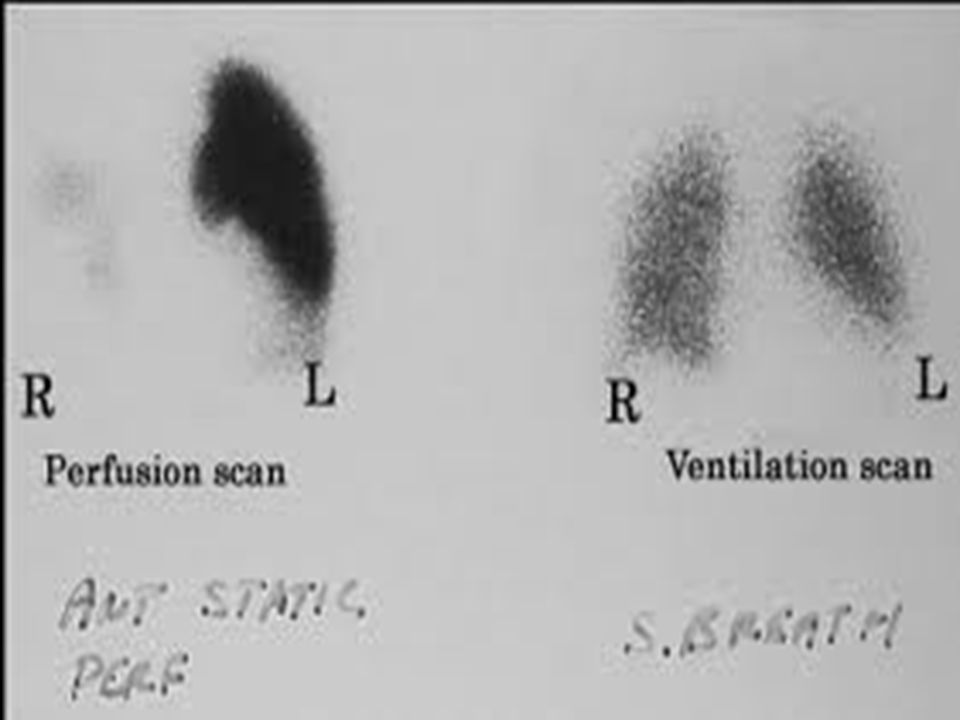
Diagnosis D-Dimer VQ Scan Fibrin degradation product
ELISA tests are highly sensitive (>95%) Non specific (~40%): cancer, sepsis, inflammation increase d-dimer levels VQ Scan Negative result excludes PE safely in PE-unlikely patients (using Clinical probability scores)
 Non specific (~40%): cancer, sepsis, inflammation increase d-dimer levels. VQ Scan. Negative result excludes PE safely in PE-unlikely patients (using Clinical probability scores)")
32
A Normal V/Q Scan Excludes Pulmonary Embolism

34
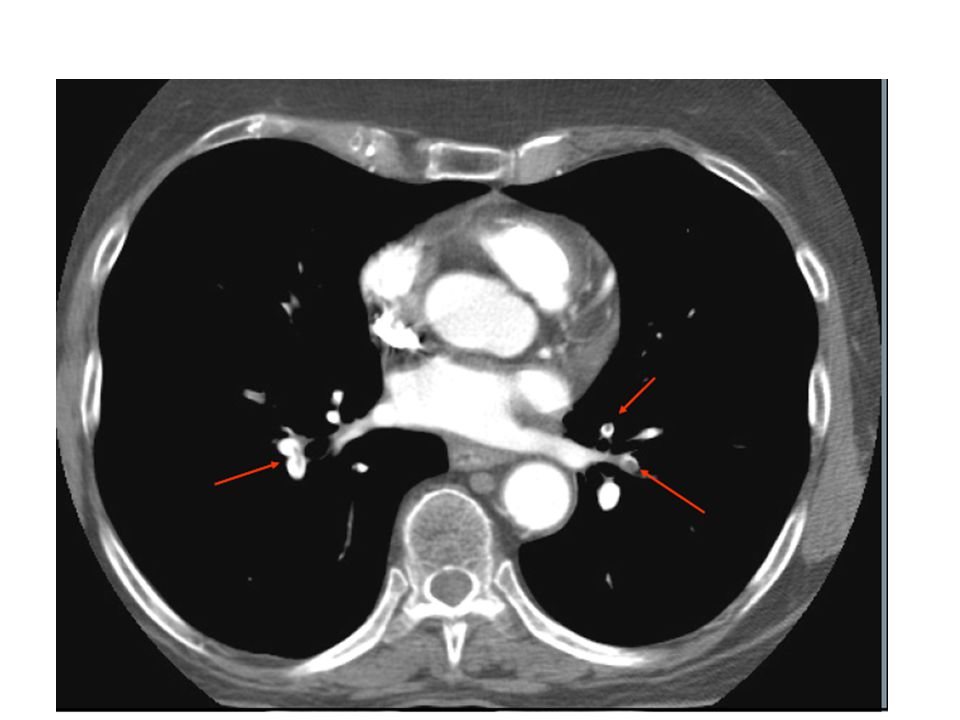
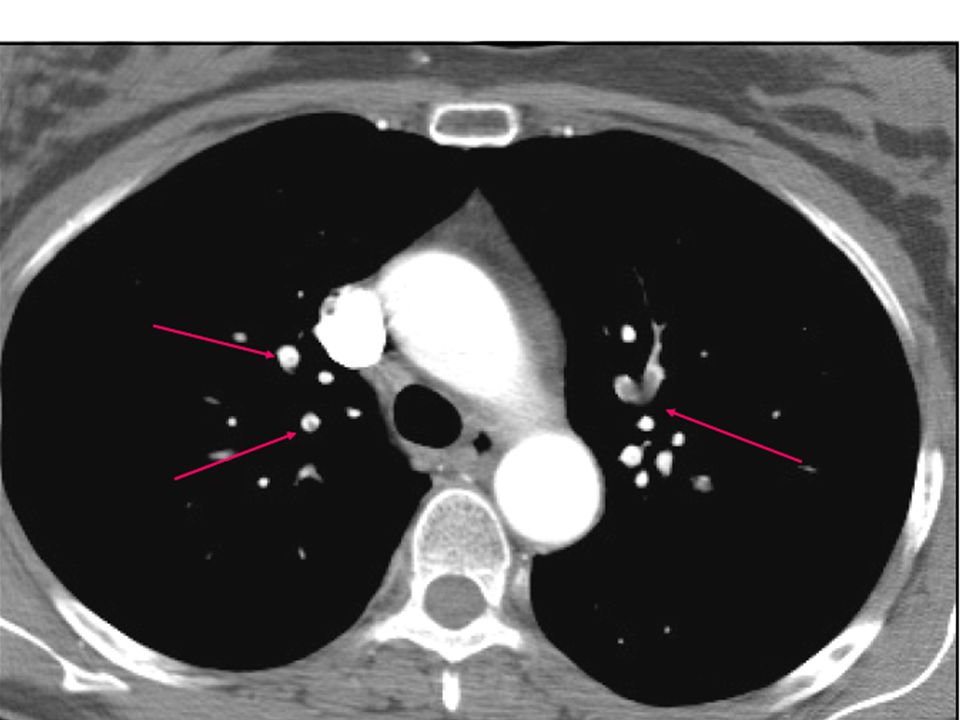
Spiral CT Direct visualization of emboli.
• Both parenchymal and mediastinal structures can be evaluated. • Offers differential diagnosis in 2/3 of cases with a negative scan. BUT… Dye load and large radiation dose Optimally used when incorporated into a validated diagnostic decision tree

37
3 month VTE rate 0.5% (all non fatal) 1.3% This algorithm allowed for a management decision in 98% of patients presenting with symptoms suggestive of PE

38
Diagnosis- Summary History and physical examination
Then 1,2,3 approach: Clinical decision score D-Dimer test Chest CT 3’. (V/Q scan remains a valid option for patients with contraindication to CT)
")
39
Clinical Management After disembarking from a 10 hour airline flight, a 69 year old man w/o past medical hx presents to the ER with acute dyspnea. BP is 120/80 (baseline) and pulse is 120 BPM. Wells score = 5 (intermediate), D-Dimer is positive. Spiral CT shows bilateral pulmonary emboli in >50% of arterial tree.
 and pulse is 120 BPM. Wells score = 5 (intermediate), D-Dimer is positive. Spiral CT shows bilateral pulmonary emboli in >50% of arterial tree.")
40
Congratulations! You’ve made the diagnosis.
What’s next?

41
Question: For the hemodynamically stable patient, how can we differentiate between patients who are going to do well with anticoagulation alone versus those with worse prognosis who might benefit from more aggressive therapy?

42
RISK STRATIFICATION

43
Poor Prognostic Signs Hypotension (not caused by arrhythmia, sepsis, or hypovolemia) SBP <90 mm Hg = 53% 90-day all cause mortality SBP drop of 40 mm Hg for at least 15 minutes = 15% in–hospital mortality Syncope= bad Shock= really bad

44
Poor Prognosis: myocardial injury
Troponin levels correlate with in-hospital mortality and clinical course in PE Troponins do not necessarily mean “MI” Significantly increased mortality in patients with troponin level >0.1 ng/ml (O.R.= 6) Normal troponin has very high NPV (99-100%) Prognostic value of troponins in acute pulmonary embolism: a meta analysis. Circulation 2007;116:
 Normal troponin has very high NPV (99-100%) Prognostic value of troponins in acute pulmonary embolism: a meta analysis. Circulation 2007;116:")
45
Poor Prognosis: myocardial dysfunction
Brain natriuretic peptide Elevated levels related to worse outcomes. Low levels can identify patients with a good prognosis (NPV %) Prognostic role of brain natriuretic peptide in acute pulmonary embolism. Circulation 2003;107:
 Prognostic role of brain natriuretic peptide in acute pulmonary embolism. Circulation 2003;107:")
46
CT evidence of RV dysfunction
RV dilation RV/LV short axis >1= pulmonary hypertension RV/LV short axis >1.5= severe PE Leftward septal bowing

47
Transverse contrast-enhanced CT scan shows maximum minor axis measurements of the right ventricle (A) and left ventricle (B). Figure 1. Transverse contrast-enhanced CT scan shows maximum minor axis measurements of the right ventricle (A) and left ventricle (B). Note the flattening of the interventricular septum. RV/LV ratio = 1.81. van der Meer R W et al. Radiology 2005;235: ©2005 by Radiological Society of North America
 and left ventricle (B). Note the flattening of the interventricular septum. RV/LV ratio = van der Meer R W et al. Radiology 2005;235: ©2005 by Radiological Society of North America.")
48
Echocardiograms before and after Thrombolysis
Echocardiography-RV Dilation Echocardiograms before and after Thrombolysis. A 29-year-old woman presented with progressive shortness of breath. A computed tomographic scan of the chest showed a central "saddle" pulmonary embolism. An echocardiogram (Panel A) showed an enlarged right ventricle and hypokinetic motion of the right ventricular free wall. After treatment with alteplase, the right ventricular size and wall motion returned to normal (Panel B). Echocardiograms courtesy of Scott D. Solomon, M.D., and Jose M. Rivero. (Videos of these images are available with the full text of this article at
 showed an enlarged right ventricle and hypokinetic motion of the right ventricular free wall. After treatment with alteplase, the right ventricular size and wall motion returned to normal (Panel B). Echocardiograms courtesy of Scott D. Solomon, M.D., and Jose M. Rivero. (Videos of these images are available with the full text of this article at")
49
Summary-Elements of PE Risk Stratification

50
Approved thrombolytic regimens for pulmonary embolism
Streptokinase IU as a loading dose over 30 min, followed by IU/h over 12–24 h Accelerated regimen: 1.5 million IU over 2 h Urokinase 4400 IU/kg as a loading dose over 10 min, followed by 4400 IU/kg/h over 12–24 h Accelerated regimen: 3 million IU over 2 h

51
Catheter Embolectomy & Fragmentation
An alternative in high-risk PE patients when thrombolysis is absolutely contraindicated or has failed Kucher N Chest 2007;132:

52
Heparin plus Alteplase Compared with Heparin Alone in Patients with Submassive Pulmonary Embolism
Stavros Konstantinides, M.D., Annette Geibel, M.D., Gerhard Heusel, Ph.D., Fritz Heinrich, M.D., Wolfgang Kasper, M.D. and the Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators N Engl J Med Volume 347;15: October 10, 2002

53
Conclusions: A combination of alteplase (100 mg given over a two-hour period) and heparin prevented the need for escalation of treatment (with open-label alteplase, catecholamine infusion, or mechanical ventilation) due to clinical deterioration more often than a combination of placebo and heparin. Clinical deterioration usually meant worsening symptoms, especially worsening respiratory failure.
 and heparin prevented the need for escalation of treatment (with open-label alteplase, catecholamine infusion, or mechanical ventilation) due to clinical deterioration more often than a combination of placebo and heparin. Clinical deterioration usually meant worsening symptoms, especially worsening respiratory failure.")
54
Bottom line The decision to use thrombolytic therapy in the intermediate risk PE group should be made on a case-by-case basis after carefully weighing the strength of the indication, the potential benefits, the contraindications, and potential adverse effects.

55
ESC Guidelines: Non-High Risk PE
Anticoagulation should be initiated without delay in patients with high or intermediate clinical probability of PE while diagnostic workup is still ongoing Use of LMWH or fondaparinux is the recommended form of initial treatment for most patients with non-high-risk PE 3. In patients at high risk of bleeding and in those with severe renal dysfunction, unfractionated heparin with an aPTT target range of 1.5–2.5 times normal is a recommended form of initial treatment Guidelines on the diagnosis and management of acute pulmonary embolism European Heart Journal (2008) 29, 2276–2315
 29, 2276–2315.")
56
Non-High Risk PE 4. Initial treatment with unfractionated heparin, LMWH or fondaparinux should be continued for at least 5 days and may be replaced by vitamin K antagonists only after achieving target INR levels for at least 2 consecutive days 5. Routine use of thrombolysis in non–high-risk PE patients is not (yet) recommended, but it may be considered in selected patients with intermediate-risk PE (RV dysfunction, elevated troponin, BNP) and low bleeding risk Guidelines on the diagnosis and management of acute pulmonary embolism European Heart Journal (2008) 29, 2276–2315
 recommended, but it may be considered in selected patients with intermediate-risk PE (RV dysfunction, elevated troponin, BNP) and low bleeding risk. Guidelines on the diagnosis and management of acute pulmonary embolism. European Heart Journal (2008) 29, 2276–2315.")
57
Treatment of Acute Pulmonary Embolism
First unprovoked PE: rx for at least 3-6 months Recurrent PE or PE and uncured cancer: Consider long term anticoagulation if benefits>risk Agnelli G, Becattini C. N Engl J Med 2010;363:

58
IVC Filters May provide lifelong protection against PE
Unclear effect on overall survival Complications: DVT (20%) Post thrombotic syndrome (40%) IVC thrombosis (30%) Risk/benefit ratio difficult to determine since no RCT Use when there are absolute contraindications to anticoagulation and a high risk of VTE recurrence Consider in pregnant women with extensive thrombosis Optimal duration of retrievable filters is unclear
 Post thrombotic syndrome (40%) IVC thrombosis (30%) Risk/benefit ratio difficult to determine since no RCT. Use when there are absolute contraindications to anticoagulation and a high risk of VTE recurrence. Consider in pregnant women with extensive thrombosis. Optimal duration of retrievable filters is unclear.")
59
Bard Recovery vena cava filter (Bard Peripheral Vascular, Tempe, Arizona) implanted in patient 2
Nicholson, W. et al. Arch Intern Med 2010;0: Copyright restrictions may apply.

60
The key is “prevention”
DVT prophylaxis in at-risk patients is quite effective Just do it!

Similar presentations













 F.R.C.P. (E) F.R.C.P. (LONDON) F.A.C.C DESIGNED AT A.V. DEPT F.J.M.C.>")








