Download presentation
Presentation is loading. Please wait.

11
CASE LBP caused by OA PAIN PATHWAY PAIN SENSITIZATION PAIN MANAGEMENT Role of Pain Medications in the Pain Pathway Prevention of Pain Sensitization Pain Management Guidelines

12
56 year old, Female, Public School Teacher DM type 2, well controlled Obese Type 2 Complaints : Hip and knee pain Other complaints: “ngalay of her lower extremeties”

13
What is the cause of the patient’s pain? Based on his history what type of pain is he experiencing? Nociceptive Neuropathic Mixed Acute Chronic

14
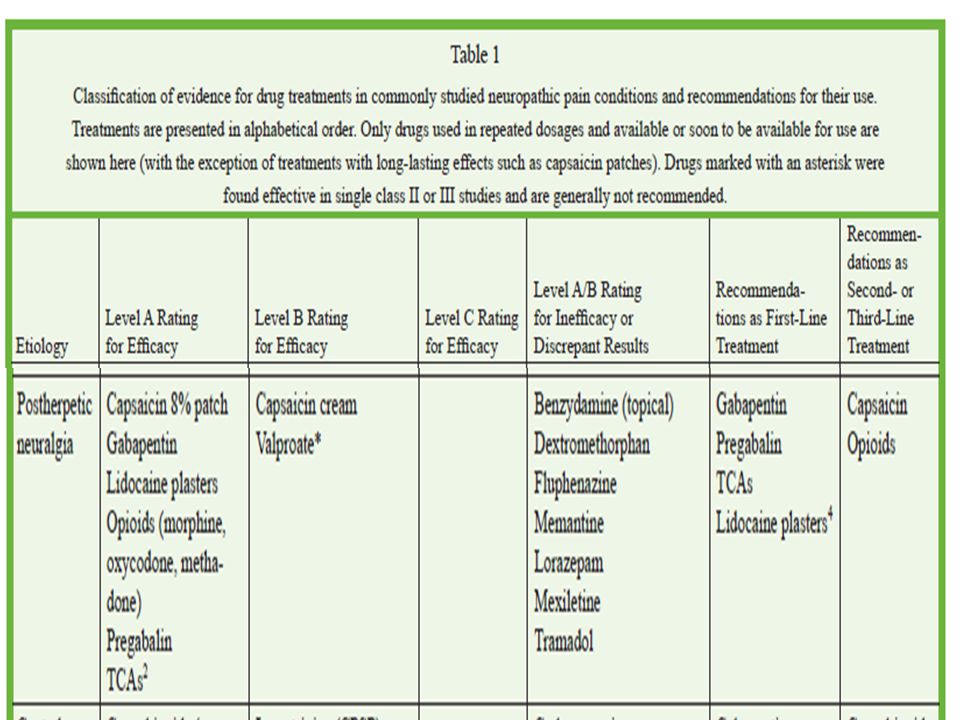
Pain, the predominant symptom in OA, is multidimensional in its nature and mediated through a variety of factors. Osteoarthritis (OA) chronic pain, involve nociceptive as well as nonnociceptive components, including neuropathic components, due to peripheral inflammation and central sensitization C. S. Bonnet and D. A. Walsh Mart van de Laar, Joseph V. Pergolizzi Jr, Hans-Ulrich Mellinghoff The Open Rheumatology Journal, 2012, 6, 320-330 1874-3129/
 chronic pain, involve nociceptive as well as nonnociceptive components, including neuropathic components, due to peripheral inflammation and central sensitization C. S. Bonnet and D. A. Walsh Mart van de Laar, Joseph V. Pergolizzi Jr, Hans-Ulrich Mellinghoff The Open Rheumatology Journal, 2012, 6, /.")
15
Many patients with chronic lower back pain have no radiculopathic or anatomic abnormalities that could explain their symptoms. Evidence suggests that sensitization of the central nervous system (CNS) may perpetuate the perception of pain in the absence of ongoing tissue damage. Borenstein DG. Epidemiology, etiology, diagnostic evaluation, and treatment of low back pain. Curt Opin Rheumatol. 2001;13:128-134.
 may perpetuate the perception of pain in the absence of ongoing tissue damage. Borenstein DG. Epidemiology, etiology, diagnostic evaluation, and treatment of low back pain. Curt Opin Rheumatol. 2001;13:")
17
Bingham B et al. (2008) The molecular basis of pain and its clinical implications in rheumatology
 The molecular basis of pain and its clinical implications in rheumatology")
18
TRANSDUCTION Journal of Medicinal Chemistry, 2007, Vol. 50, No. 11

19
SYNAPTIC TRANSMISSION Journal of Medicinal Chemistry, 2007, Vol. 50, No. 11

20
Ascending and Descending Modulation Perception Journal of Medicinal Chemistry, 2007, Vol. 50, No. 11

21
What will be your goal in managing this patient’s pain? Decrease Pain score by -2 from baseline Increase ability to perform ROM exercises Prevent chronicity/sensitization of pain

22
The pain experience in OA results from interactions between inflammation and other features of the disease including: radiological severity, innervation of articular structures, central and peripheral sensitization and psychological factors

23
The Journal of Pain, Vol 10, No 9 (September), 2009: pp 895-926
, 2009: pp")
24
American Family Physician, Gottschalk et.al MAY 15, 2001 / VOLUME 63, NUMBER 10

26
Ultimately, multimodal approaches that address multiple sites along the pain pathway may prove necessary to adequately prevent central sensitization in many surgical procedures. American Family Physician, Gottschalk et.al MAY 15, 2001 / VOLUME 63, NUMBER 10

27
Working Group A.M.A.D.E.U.S. Basic Course in Treatment of Chronic Pain, Cologne 2003.

28
What will be the factors that you will consider in choosing the right pharmacologic intervention? (based on your priority) Efficacy of the drug- alleviate the amount of pain the fastest Side-effect profile of the drug Mode of Action- targets majority of the processes in the pain pathway Pain Management Guidelines
 Efficacy of the drug- alleviate the amount of pain the fastest Side-effect profile of the drug Mode of Action- targets majority of the processes in the pain pathway Pain Management Guidelines.")
29
Although pain is the most pressing problem facing people with OA, adequate pain relief is frequently not achieved maybe because: (a) lack of professional medical attention, (b) failure to incorporate nonpharmacological measures such as weight loss and exercise into the treatment plan, and (c) overreliance on monotherapy. Arthritis Foundation, Association of State and Territorial Health Officials, Centers for Disease Control and Prevention. National arthritis action plan. A public health strategy. Internet: CDC; 1999 [cited September 26, 2003]

30
Selective and nonselective NSAIDs Tramadol/paracetamol combination Mild Pain X Moderate Pain XX Severe Pain X Acute Vs Chronic Pain XX Neuropathic Pain X Anti-inflammatory effect X Pediatric Use X Geriatric Use X Patients with renal failure can still be used to patients with moderate renal impairment Patients with CV Risks X Pergolizzi Jr et al Journal of Pain Research 2012:5 327–346

32
American Family Physician, Gottschalk et.al MAY 15, 2001 / VOLUME 63, NUMBER 10

33
PAIN MEDICATIONTRANSDUCTIONTRANSMISSION DESCENDING MODULATION NSAIDs x Local Anesthetics x Anti-epileptic drugs x Opioids xx Peripheral and Spinal Nerve Blocks x Epidural and intrathecal analgesics x Antidepressants X SNRIs x January 2009 Vol 5 No 1 Bingham et.al.

47
Potential advantages of a fixed-dose tramadol/paracetamol analgesic product: include a broader analgesic spectrum a complementary pharmacokinetic profile potentially synergistic analgesic effect greater convenience (possibly resulting in better compliance, thus, improved therapy) an improved ratio of efficacy to adverse effects. Pergolizzi Jr et al Journal of Pain Research 2012:5 327–346

48
TRAMADOL peak = 2-3 hrs T 1/2 = 6 hrs TIME Drug Effect APAP peak = 30 min T 1/2 = 2 hrs Tramadol/Paracetamol: Rationale In combination, T 1/2 extends to 7-9 hours Result of combination: –Fast onset of action –Prolonged action Pergolizzi Jr et al Journal of Pain Research 2012:5 327–346

49
Osteoarthritis Low Back Pain

51
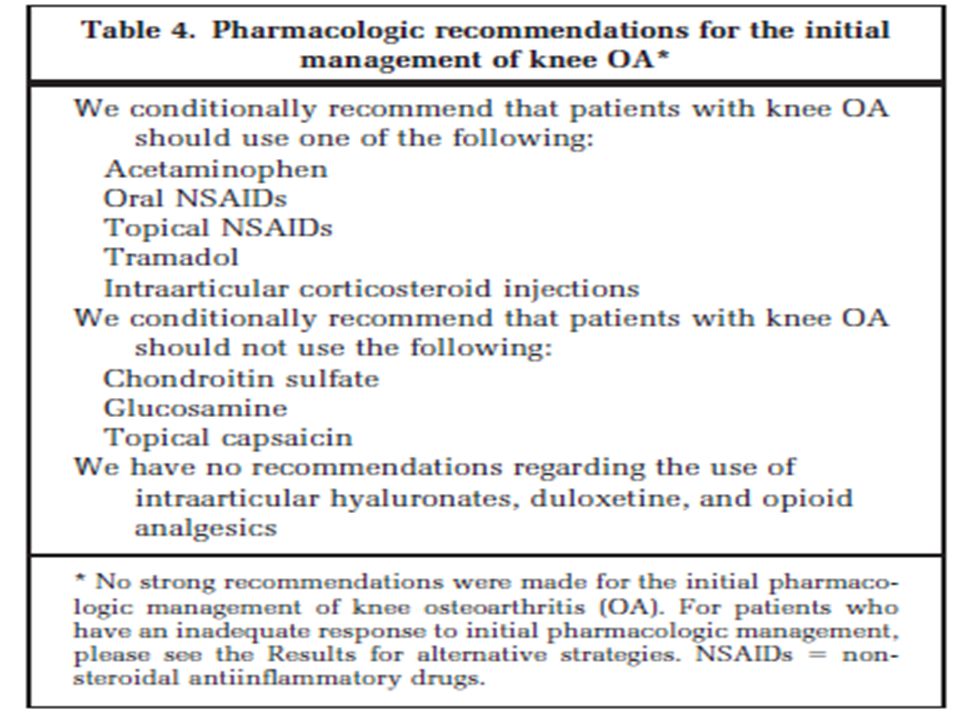
NSAIDs are commonly prescribed for knee OA pain. However, flare ups of OA pain or poor control with NSAIDs alone are common and necessitate the addition of other analgesics with different mechanisms, such as tramadol

52
The purpose of this study is to compare the efficacy of tramadol 37.5 mg/acetaminophen 325 mg combination tablets (tramadol/APAP) with that of nonsteroidal anti-inflammatory drugs (NSAIDs) as maintenance therapy following tramadol/APAP and NSAID combination therapy in knee osteoarthritis (OA) pain which was inadequately controlled by NSAIDs. DESIGN: This was a randomized, multicenter, open comparative study in out-patients at six sites.

54
Why do you think it is a better choice to use Tramadol/APAP FDC as a maintenance drug for OA pain compared to NSAIDs?

55
Our speculation is that in our subjects with inadequately controlled knee OA pain, chronic continuous pain stimuli from diseased joints might have caused sustained activation of sensory fibers supplying the dorsal horn in the spinal cord and change in the nature of the pain and resulted in central sensitization and making pain refractory to NSAIDs.

56
Tramadol is reported to have a dual mechanism of action which are good for the control of central sensitization; μ-opioid receptor binding and inhibiting reuptake of serotonin and norepinephrine. It is therefore probable that tramadol/APAP add-on therapy eased central sensitization and made it easier to control knee OA pain.

57
In conclusion, when added to NSAID, tramadol/APAP was generally well tolerated and significantly improved knee OA pain which was previously refractory to NSAID therapy. In those subjects who showed favorable response to tramadol/APAP and NSAID combination therapy, both tramadol/APAP and NSAIDs were effective at maintaining the pain-reduced state and there was no significant difference in efficacy between tramadol/APAP and NSAIDs.

59
Considering the Long-term treatment with NSAIDs can cause various side effects, Tramadol/Paracetamol can therefore be considered as the good candidate for maintaining pain improved state of Osteoarthritis patients - http://www.who.int/cancer/palliative/painladder/en/

Similar presentations























 Prepared by the United.>")










>")
>")



