Download presentation
Presentation is loading. Please wait.

1
PHCL 424 Management Gout Ahmed Shaman Clinical Pharmacy Department KSU shaman@KSU.edu.sa 1

2
Introduction Inflammatory arthritis mediated by the crystallization of uric acid within joints, tophi Manifests as recurrent episodes of – Acute joint pain and inflammation – Secondary to the deposition of monosodium urate (MSU) crystals in the synovial fluid and lining MSU deposition in the urinary tract can cause urolithiasis and urinary obstruction Patients with gout cycle between – Flares of acute joint pain and inflammation – Periods of quietness with no symptoms of the disease They can also exhibit chronic tophaceous gout and hyperuricemia
 crystals in the synovial fluid and lining MSU deposition in the urinary tract can cause urolithiasis and urinary obstruction Patients with gout cycle between – Flares of acute joint pain and inflammation – Periods of quietness with no symptoms of the disease They can also exhibit chronic tophaceous gout and hyperuricemia")
3
Introduction Tophi are hard nodules of MSU crystals that have deposited in soft tissues and are most commonly found in toes,fingers,and elbows Acute gout presents as mono-articular inflammation in 85% to 90% of patients with the first metatarsophalangeal joint (great toe) typically affected Patients presenting with acute gout may or may not have hyperuricemia.
 typically affected Patients presenting with acute gout may or may not have hyperuricemia.")
4
Gout - Acute Arthritis Acute synovitis, ankle & first MTP joints

5
Chronic Tophaceous Gout Tophus = Localized deposit of monosodium urate crystals

6
Gout - Tophus Classic location of tophi on helix of ear

7
Gout - X-Ray Changes DIP joint destruction Phalangeal bone cysts

8
Gout - X-Ray Changes Bony erosions

9
Uric Acid Metabolism Uric acid serves no biological function It is the end product of purine metabolism Humans lack the enzyme uricase – Which degrades uric acid into more soluble products for excretion (allantoin) 60-80% excreted renally & reminder by GIT May result from – Overproduction 10% – Underexcretion 90% – Both
 60-80% excreted renally & reminder by GIT May result from – Overproduction 10% – Underexcretion 90% – Both")
10
Uric Acid Metabolism Overproduction – Excessive de novo purine synthesis rare genetic enzyme mutation defects – Neoplastic diseases – Aggressive cytotoxic chemotherapy – Excessive intake of dietary purines meat, seafood, dried peas and beans, certain vegetables (e.g., mushrooms, spinach, asparagus), beer, and other alcoholic beverages
, beer, and other alcoholic beverages")
11
Uric Acid Metabolism Underexcretion – After glomerular filtration, 98-100% reabsorbed; approx. 50% secreted back into proximal tubule. & 40% reabsorbed again. – Only 8-12% of urate excreted in urine as uric acid – Homeostasis between reabsorption and secretion of urate is maintained in normal subject – Renal impairment, certain drugs can cause this balance to fail

12
Renal handling of uric acid Glomerular filtration Tubular reabsorption Tubular excretion Post-secretory reabsorption Net excretion

13
Uric Acid Metabolism cell breakdown dietary intakePurine bases HypoxanthineXanthine Uric acid Xanthine oxidase catalyzes hypoxanthine to xanthine & xanthine to uric acid

14
Hyperuricemia - mechanisms hyperuricemia excessive production inadequate excretion

15
Hyperuricemia - mechanisms hyperuricemia Overproducersunderexcretors

16
Gout - problems Excessive total body levels of uric acid Deposition of monosodium urate crystals in joints & other tissues Crystal-induced inflammation

17
Crystal-Induced Inflammation PMN is critical component of crystal- induced inflammation Phagocytosis leading to secretion of interleukin-1β, TNF-α, interleukin-6 and 8, leukotrienes, and alarmins, C5b-9 membrane attack complex MSU crystal deposition hyperuricemia protein binding receptor binding cytokine release influx of PMN’s crystals engulfed inflammation

18
Classifying Hyperuricemia Serum uric acid level Urine uric acid excretion (24-hour)
")
19
Gout - Cardinal Manifestations NephrolithiasisNephropathyArthritisTophi Hyperuricemia acute & chronic

20
Hyperuricemia & Gout 5-Year PrevalenceAnnual IncidenceSerum Uric Acid Level 30%70> 10 mg/dl 0.6%0.9< 7 mg/dl

21
Risk Factors for Gout Drugs: – Thiazide diuretics, cyclosporine, and low-dose aspirin (<1 g per day) Insulin resistance, metabolic syndrome, obesity, renal insufficiency, hypertension, congestive heart failure, and organ transplantation. Increased intake of dietary purines Lead intoxication History of urolithiasis

22
Diagnosis of Gout Synovial fluid or tophus aspiration – Identification of MSU crystals under polarizing microscopy During acute attacks, strongly birefringent needle-shaped MSU crystals with negative elongation are largely intracellular Effusion appear cloudy due to leukocytes & large amounts of crystals occasionally produce thick pasty or chalky joint fluid

23
Monosodium Urate Crystals Polarized lightRed compensator Needle shape Negative birefringence

24
Drugs for Gout Allopurinol Febuxostat Probenecid Steroids NSAID’s Colchicine Acute Arthritis Drugs Urate Lowering Therapy Pegloticase

25
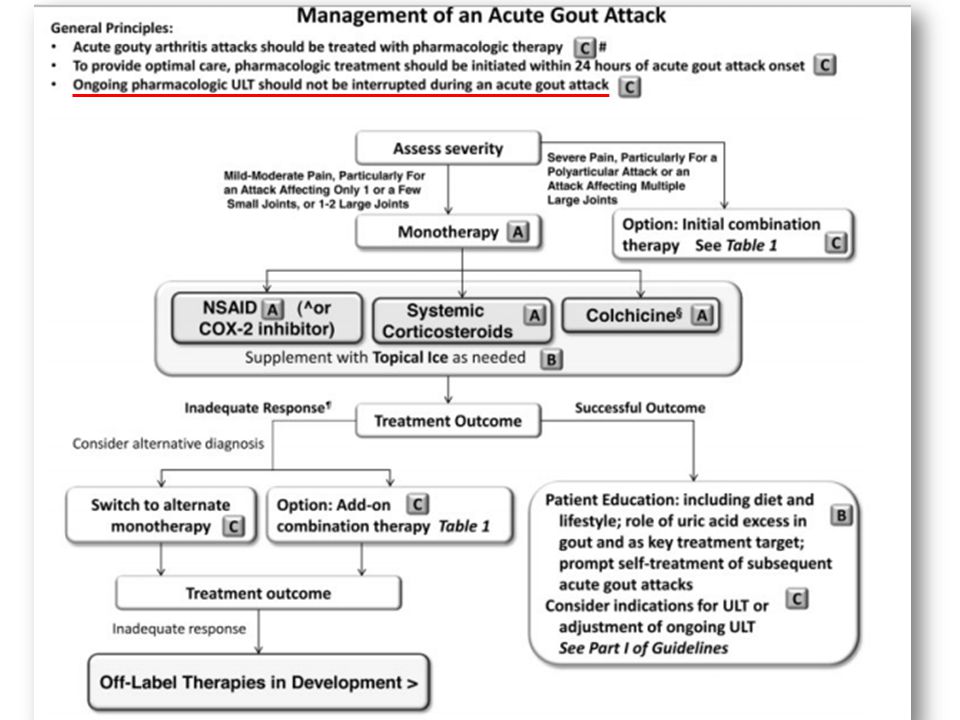
Acute gout NSAIDs (except aspirin) – Treatment of choice for acute gout if not contraindicated – All NSAIDs appear to be equally effective – Use full dose and continue treatment for a week after acute attack has settled Corticosteroids: – Often the preferred treatment for acute gout in patients with complex medical problems where NSAIDs are contraindicated – They may be given systemically (orally or IV) – Or by intra-articular injection when 1 or 2 joints are involved Colchicine – Is reserved for acute gout when NSAIDs and corticosteroids (systemic or intra-articular) are contraindicated or inappropriate
 – Treatment of choice for acute gout if not contraindicated – All NSAIDs appear to be equally effective – Use full dose and continue treatment for a week after acute attack has settled Corticosteroids: – Often the preferred treatment for acute gout in patients with complex medical problems where NSAIDs are contraindicated – They may be given systemically (orally or IV) – Or by intra-articular injection when 1 or 2 joints are involved Colchicine – Is reserved for acute gout when NSAIDs and corticosteroids (systemic or intra-articular) are contraindicated or inappropriate")
26
Colchicine Relief of pain in acute gout Mode of action – Inhibits neutrophil migration, chemotaxis, adhesion and phagocytosis in the inflamed area Reduces the inflammatory reaction to urate crystals Has no effect on uric acid production or excretion

27
Colchicine – Toxicity Common – Diarrhea, nausea, abdominal discomfort, vomiting, pharyngolaryngeal pain Hematologic – Agranulocytosis, aplastic anemia, thrombocytopenia Muscular – Myopathy, myalgia, rhabdomyolysis Adverse effects are dose-related – More common when patient has renal or hepatic impairment

28
Colchicine – Dosing For 0.6 mg tablet – A loading dose of 1.2 mg of colchicine followed by 0.6 mg 1 hour later – Followed by gout attack prophylaxis dosing 0.6 mg once or twice daily 12 hours later, until the gout attack resolves For 0.5 mg tablet – 1.0 mg colchicine as the loading dose followed by 0.5 mg 1 hour later – Followed after 12 hours, by continued colchicine (up to 0.5 mg 3 times daily) until the acute attack resolves
 until the acute attack resolves")
29
Colchicine – Dosing CrCl <80 mL/minute or hepatic impairment – Do not use for acute attack if using colchicine for prophylaxis. CrCl <30 mL/minute or severe hepatic impairment, – Do not repeat the course within 2 weeks Dialysis – 500 micrograms single dose – Do not repeat within 2 weeks

30
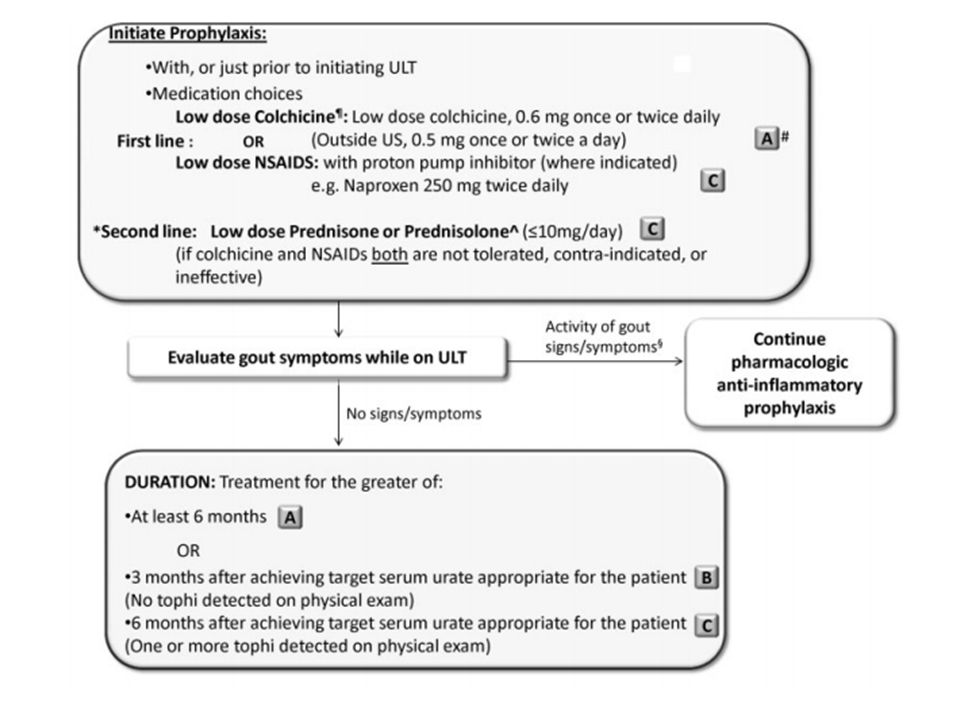
Colchicine – Dosing Prophylaxis when starting urate-lowering treatment: – Adult, 500 micrograms once or twice daily, according to response and GI symptoms. – CrCl <30 mL/minute, initially 250 micrograms once daily. – Dialysis, initially 250 micrograms twice a week.

31
Colchicine Colchicine is metabolized by CYP3A4 and is a substrate of P-glycoprotein Inhibitors of cytochrome P450 3A4 and of P- glycoprotein – Clarithromycin, erythromycin, cyclosporine, and disulfiram, itraconazole – Avoid or adjust the dose by 50%

32
Acute Gout Drugs NSAIDs – Most effective drugs are those with short half-life Indomethacin 25-50 mg t.d.s Ibuprofen 800 mg t.d.s Diclofenac 50 mg t.d.s – COX-II inhibitors are equally effective Glucocorticoids – Prednisolone 0.5-1 mg/kg/day tapered over 5-7 days – Single IV dose of methylprednisolone – Single intramuscular dose of triamcinolone acetonide 60 mg

35
Urate-lowering therapy (ULT) Should be considered in patients with – 1 or more tophi, ≥2 attacks per year – Chronic kidney disease (CKD; stage 2 or worse) – History of urolithiasis First-line: allopurinol or febuxostat Probenecid as alternative Start ULT during acute attack Monitor serum urate level every 2-5 weeks during titration Target serum urate level of <6 mg/dL
 Should be considered in patients with – 1 or more tophi, ≥2 attacks per year – Chronic kidney disease (CKD; stage 2 or worse) – History of urolithiasis First-line: allopurinol or febuxostat Probenecid as alternative Start ULT during acute attack Monitor serum urate level every 2-5 weeks during titration Target serum urate level of <6 mg/dL")
36
2012 American College of Rheumatology Guidelines for Management of Gout Single Agent XOI titrated to Max dose OR (if contraindicated ) Probenecid Serum urate target not achieved, continuing disease activity Add Uricosuric to XOI with both dose titrated to Max dose Pegloticase Serum urate target not achieved, continuing disease activity
 Probenecid Serum urate target not achieved, continuing disease activity Add Uricosuric to XOI with both dose titrated to Max dose Pegloticase Serum urate target not achieved, continuing disease activity")
37
Allopurinol Mode of Action Reduces uric acid production by – Inhibiting xanthine oxidase, and lowers plasma and urinary urate concentrations – Allopurinol is metabolised to oxypurinol, which also inhibits xanthine oxidase

38
Allopurinol Chemical Structure N N O N N Allopurinol N HN O N NHNH HypoxanthineXanthine N N NHNH N HOHO OHOH

39
2012 American College of Rheumatology Guidelines for Management of Gout Starting allopurinol dose should not exceed 100 mg/day – Patients with CKD of stage 4 or higher should be started at 50 mg/day – Dosages should be titrated up every 2-5 weeks to achieve target serum uric acid and can go above 300 mg/day as long as the patient is educated and monitored for adverse events – Screening for the HLA-B*5801 in high-risk individuals

40
Allopurinol Wait until the attack has settled before starting allopurinol – May worsen and prolong the attack – Once treatment is established, continue allopurinol at the current dose, even during acute attacks

41
Allopurinol - common reactions Common – maculopapular or itchy rash Infrequent – Acute attacks of gout – Nausea, vomiting, diarrhea, abdominal pain, headache, drowsiness, vertigo, arthralgia

42
Allopurinol - serious reactions Fever, rash, toxic epidermal necrolysis Hepatotoxicity, bone marrow suppression Vasculities Death Peripheral neuropathy, cataract (treatment >3 years) Drug interactions – Mercaptopurine, azathioprine → risk of severe bone marrow toxicity → reduce Aza dose to 1/3 or 1/4
 Drug interactions – Mercaptopurine, azathioprine → risk of severe bone marrow toxicity → reduce Aza dose to 1/3 or 1/4")
43
Allopurinol – Black Box Warning THIS IS NOT AN INNOCUOUS DRUG. IT IS NOT RECOMMENDED FOR THE TREATMENT OF ASYMPTOMATIC HYPERURICEMIA ALLOPURINOL SHOULD BE DISCONTINUED AT THE FIRST APPEARANCE OF SKIN RASH OR OTHER SIGNS OF AN ALLERGIC REACTION

44
Allopurinol hypersensitivity Extremely serious problem Prompt recognition required First sign usually skin rash More common with impaired renal function Progression to toxic epidermal necrolysis & death

45
Stevens-Johnson Syndrome Target skin lesions Mucous membrane erosions Epidermal necrosis with skin detachment

46
Febuxostat Recently approved by FDA Oral xanthine oxidase inhibitor Chemically distinct from allopurinol 94% of patients reached urate < 6.0 mg/dl Minimal adverse events Can be used in patients with renal disease

47
Probenecid Mode of action – Increases renal excretion of uric acid by blocking its renal tubular reabsorption Contraindications – History of nephrolithiasis – Elevated urine uric acid level – Existing renal disease Less effective in elderly patients

48
Pegloticase Recombinant uricase expressed in E.coli – Enzyme that lowers the levels of uric acid by catalyzing the oxidation of uric acid to allantoin – Uricase speeds resolution of tophi Adverse events – Anaphylaxis, 6.5% – Infusion reactions, 26% – Gout flares, Patients should be pre-medicated – Antihistamines and corticosteroids – Gout prophylaxis

49
Factors influencing drug selection Renal impairment – Corticosteroids are preferred for acute gout – NSAIDs may worsen renal function and are associated with an increased risk of GI toxicity; avoid use – Allopurinol has a renally excreted active metabolite; reduce dose to avoid toxicity – Probenecid is less effective if CrCl <50 mL/minute and is probably ineffective if CrCl <30 mL/minute – Elimination of colchicine is reduced; may cause myelosuppression; avoid colchicine or reduce dose. Anticoagulant treatment – Systemic corticosteroids are often the treatment of choice – Colchicine can be used – Avoid NSAIDs due to risk of GI bleeding – Intra-articular corticosteroids are generally not recommended

50
Factors influencing drug selection Congestive heart failure avoid – NSAIDs, COX-2 inhibitors Peptic ulcer disease avoid – NSAIDs, COX-2 inhibitors, corticosteroids Diabetes mellitus avoid – Corticosteroids Ongoing infection or high risk of infection avoid – Corticosteroids Hepatic disease avoid – NSAIDs,COX-2 inhibitors, colchicine

51
Practice Points for Gout Instruct patients with recurrent acute attacks to take an NSAID or colchicine at the earliest signs of an attack – Most attacks resolve within 7–10 days Colchicine's effect may be delayed in an acute attack – Advise use of an analgesic, e.g. paracetamol, during this time Avoid aspirin as an analgesic during an acute attack – In high doses aspirin may change plasma urate concentration, which may worsen and prolong an attack – Do not stop low-dose aspirin in coronary or cerebrovascular disease, although these doses increase urate concentrations Low-dose NSAID or colchicine long term may be used – when acute attacks occur despite adequate urate-lowering treatment – when urate-lowering treatment is not tolerated or is only partially effective They do not reduce plasma urate concentration or prevent joint damage

Similar presentations


>")








 Mononucleotides.>")




 Mononucleotides.>")


