Download presentation
Presentation is loading. Please wait.

1
Room 535 Jeff Perry, MS, ATC Deborah Cassidy, ATC jgperry@fcps.edujgperry@fcps.edu dkcassidy@fcps.edudkcassidy@fcps.edu Office: 703-426-6818 Cell: 703-932-1950

2
Sports Medicine Support Staff Team Physician: Marc Childress, MD Family/Sports Medicine, Fairfax Family Medicine, Fair Oaks 3650 Joseph Siewick Dr. Ste. 400 Fairfax, VA 22033 Team Orthopaedic: Matt Levine, MD Sports Medicine/Orthopedic Surgeon Inova Orthopaedics and Sports Medicine 3299 Woodburn Rd., Ste. 230, Annandale, VA 22003 Please contact athletic trainer first to expedite Orthopedic appt.

3
Sports Medicine Support Staff George Mason Univ. ATS: Salvatore Ferranti (Spring 2015) The ATS is a University athletic training student studying in professional educational program at GMU. They typically spend between 100 and 200 hours outside of their academic classes observing, assisting, and receiving instruction in each semester long clinical rotation. RHS ATSAs: Alisha C, Giselle C, Lexi Hsu, Seye Raymond The ATSA is a high school athletic training student aide interested in going to college to study athletic training, physical therapy, medicine, or other allied health care field. Valuable experience observing and assisting can be obtained.
 The ATS is a University athletic training student studying in professional educational program at GMU. They typically spend between 100 and 200 hours outside of their academic classes observing, assisting, and receiving instruction in each semester long clinical rotation. RHS ATSAs: Alisha C, Giselle C, Lexi Hsu, Seye Raymond The ATSA is a high school athletic training student aide interested in going to college to study athletic training, physical therapy, medicine, or other allied health care field. Valuable experience observing and assisting can be obtained..")
4
Certified Athletic Trainer (ATC) What is an Athletic Trainer? –At least 4 year degree and successful completion of National Accreditation Exam –Licensed by Virginia’s Board of Medicine to practice athletic training –Often confused with “personal trainer” or “sports trainer” at a gym or fitness club –Visit www.nata.org for more information

5
AT Responsibilities 1.Prevention of injuries and re-injury 2.Recognition, evaluation, and assessment of injuries and conditions resulting 3.Immediate care of injuries 4.Rehabilitation and reconditioning of injuries 5.Organization and administration of Athletic Training Program 6.Professional development and education (for athletes, coaches, community)
")
6
Athletic Trainer Coverage Athletic Training Center Room 535 Located upstairs south side of field house. The Athletic Trainer is available for evaluations, treatments, rehabilitation, and questions from student athletes, parents and physicians each school day afternoon. Office Hours: generally M-F 12:30 to 5 PM, then practice or event coverage to 8, 9 or10 PM.

7
FALL Football (all games and equipment/contact practices) Field Hockey Volleyball* Cheer Competition Cross Country Meets* WINTER Wrestling Basketball Gymnastics Indoor Track Swim playoff meets* Athletic Trainer Event Coverage SPRING Boys and Girls Lacrosse Track and Field Soccer Tennis* Softball Baseball*ATC on site
 Field Hockey Volleyball* Cheer Competition Cross Country Meets* WINTER Wrestling Basketball Gymnastics Indoor Track Swim playoff meets* Athletic Trainer Event Coverage SPRING Boys and Girls Lacrosse Track and Field Soccer Tennis* Softball Baseball*ATC on site")
8
VHSL Sports Physicals (PPE) Before participation, Athletes must have a sports physical completed after May 1 st and before sport season. It is valid until June 30 th the following year. It Must be completed on a current VHSL Pre- Participation Exam form (Revised March 2013). A Commonwealth School Entrance Exam or BSA form are NOT valid for sports. Find the current form on the athletics website. Don’t save a copy to your computer as forms are occasionally updated and VHSL does not accept older versions of their own form. PPE is needed to join in team related conditioning and “green day” activity as well.
. A Commonwealth School Entrance Exam or BSA form are NOT valid for sports. Find the current form on the athletics website. Don’t save a copy to your computer as forms are occasionally updated and VHSL does not accept older versions of their own form. PPE is needed to join in team related conditioning and green day activity as well..")
9
VHSL Sports Physicals Completed page 1 of VHSL form and have student signed the bottom of page. Complete page 2 health questions and box used to explain any “Yes” answers. Both student and a parent signed bottom of page 2. The doctor (MD, DO, LNP, PA only) completes page 3, make sure they have signed and dated it. Page 4 should be completed by parent including medical insurance company name and requires a parent signature in 2 places at bottom of page SAVE time, Do not turn in incomplete forms!
 completes page 3, make sure they have signed and dated it. Page 4 should be completed by parent including medical insurance company name and requires a parent signature in 2 places at bottom of page SAVE time, Do not turn in incomplete forms!.")
10
Concussion Education Student-athletes and a parent must complete State mandated concussion education on an annual basis before tryouts. This component of compliance can be completed by going to www.fcps.edu/sports and following path for Concussion Education. Please read directions. www.fcps.edu/sports There is a link for parents and a link for students. Enter Student ID number for each High School student in your family that may tryout for a sport. Include correct date of birth. Also, be sure to choose the correct school---Robinson! It is best to complete Concussion Education early to avoid last minute rush, or web problems, and then not be able to participate in tryouts for a day or two. If any questions contact the athletic trainer.

11
Assumption Of Risk There is inherent risk of injury in all sport Not all injuries can be prevented Even catastrophic injuries can occur in any sport A comprehensive Athletic Training health care program has proven to influence a reduction in the severity of injury and prevalence of re-injury.

12
When Injury Occurs: Any injury, illness, or medical condition must be reported to Athletic Trainer (AT) regardless of severity, or prior consultations with other Health Care Professional Minor injuries are evaluated and treatment instructions given to the athlete, with daily follow up to full resolution For injuries that MAY be more serious (where a physician evaluation recommended), parents will be contacted and receive a written report as well
 regardless of severity, or prior consultations with other Health Care Professional Minor injuries are evaluated and treatment instructions given to the athlete, with daily follow up to full resolution For injuries that MAY be more serious (where a physician evaluation recommended), parents will be contacted and receive a written report as well")
13
Injuries Happen If present at game, feel free to check on your child’s injury status on bench, sideline, or in AT clinic after their initial evaluation. Referral decisions are based on injury type, potential complication, initial injury grade, lack of progress, etc. AT philosophy is to keep injured athletes involved with their team to some level of participation while protecting injured area Athletes should be doing some rehabilitation under AT direction until released.

14
Immediate Treatment = RICES Rest it!! Ice – 20 minutes max each hour (if freezer ice-- use wet cloth barrier) Compression – wrap with even pressure towards heart Elevation – Raise Above the Heart Support – Crutches, Cane, Brace, Sling all help to protect injury Physician Visits – Please bring in a note* that informs us of diagnosis, what rehab or treatment the physician would like, and participation status. Physical Therapist of Chiropractor PT or DC Intervention should be in conjunction with school based (ATC) treatment and rehab.
 Compression – wrap with even pressure towards heart Elevation – Raise Above the Heart Support – Crutches, Cane, Brace, Sling all help to protect injury Physician Visits – Please bring in a note* that informs us of diagnosis, what rehab or treatment the physician would like, and participation status. Physical Therapist of Chiropractor PT or DC Intervention should be in conjunction with school based (ATC) treatment and rehab..")
15
The “Physician Response Form” can be found on the Athletics web site. Bring it to your doctor appointment or Urgent Care visit so we have clear feedback from treating physician

16
conducted by AT under the supervision of a physician may include the use of modalities in the form, cold, heat, manual therapy, electrical stimulation, or ultrasound Communication between AT, PT, MD or other HCP and parent may enhance the overall treatment and recovery of the student-athlete (see “Physical Therapist Response Form”) Treatments
 Treatments")
17
Rehabilitation Rehabilitation and reconditioning is another primary role of Certified Athletic Trainers We have the tools and time to work with your student-athlete on a daily basis Every injury will benefit from some form of rehabilitation

18
Athletes who are compliant with a proper rehabilitation program are less likely to become re-injured or have detrimental long-term consequences to health or athletic performance Athletes recovering from injury must be evaluated by an ATC to determine a schedule for safe return to full participation

19
Return To Play A Parent, Coach, Treating Physician, Athlete, Administrator, ATC, or Team Physician can exclude an athlete from participation. All of these individuals must agree that the athlete can and should play The Athletic Trainer is to ensure athlete is returned to play in the quickest and SAFEST manner possible to avoid re- injury.

20
Look for more information, forms, etc. on Web

21
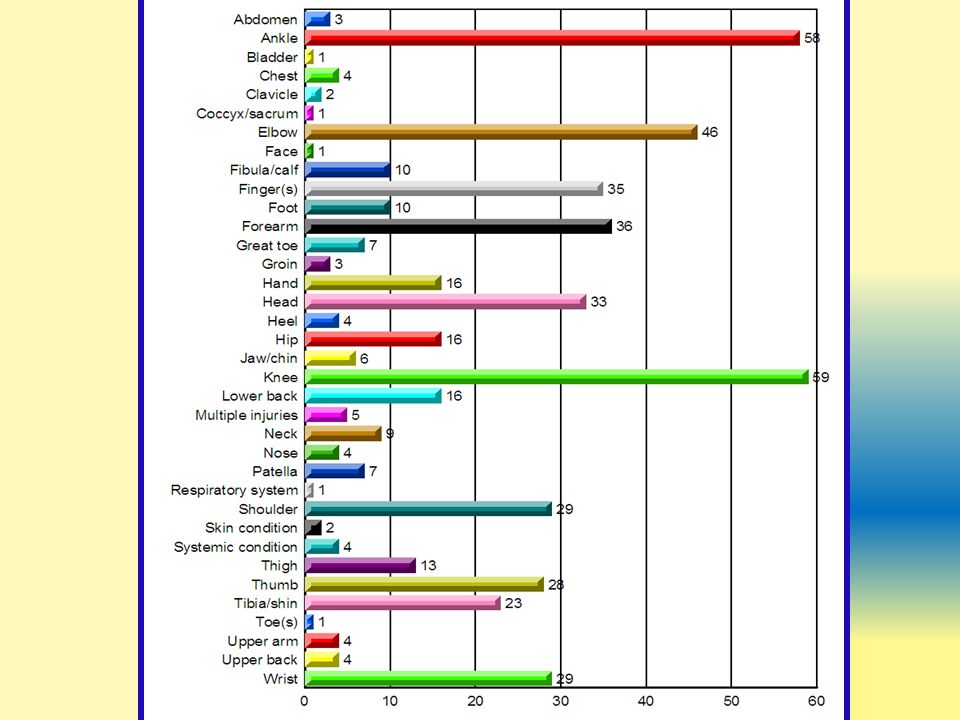
“Problems” vs. Time Loss Injuries Fall 2011 35 (time loss) (585 total “problems” = lesser than injury) 550 ************************* 46 cases (106 Total Injury cases) 60 cases Data on services provided to student-athletes for given periods are typical samples of ATP interventions.
 (585 total problems = lesser than injury) 550 ************************* 46 cases (106 Total Injury cases) 60 cases Data on services provided to student-athletes for given periods are typical samples of ATP interventions..")
23
Tx Summary Fall/Winter 2011-12 Injury Treatment Encounters: 4,161 Total Unique Athletes Seen: 442 Evaluations and Tests: 2,632 Modalities(ice, heat, ES, US,etc): 3,099 Manual Therapy: 580 Rehab Exs: 4,674 Protection (tape, wrap, pad, brace): 1,502 Wound Care: 407
: 3,099 Manual Therapy: 580 Rehab Exs: 4,674 Protection (tape, wrap, pad, brace): 1,502 Wound Care: 407")
24
Some Common Concerns MRSA Personal Hygiene Nutritional Concerns Supplements & “Energy” Drinks Steroids Medications Concussions (Education & Management Issues)
")
25
MRSA: What Is It? MRSA is a “Staph” infection. “Methicillin Resistant Staphylococcus Aureus” It does not respond to some antibiotics It is treatable Like other infections, this can become serious if left untreated Severe infections can be prevented by practicing proper hygiene and early detection

26
MRSA: What Does It Look Like? Mild infections may look like a pimple or boil. Can be red, swollen, painful, have pus or other drainage and are usually easily treated. More serious infections may cause pneumonia or bloodstream infections.

27
MRSA: What Are We Doing? FCPS Certified Athletic Trainers provide information to athletes specific to MRSA during the athlete meetings at the beginning of each season. Included in this session: View a DVD specific to MRSA –Prevention strategies for staph and other communicable diseases. –Importance of proper personal hygiene and clothes washing. –Importance of bringing all questionable lesions to the attention of the certified athletic trainer and parent immediately.

28
MRSA: What Are We Doing? The FCPS Athletic Training Program includes the use of a cleansing product for wound care that contains 4% CHG (chlorhexidine gluconate) which specifically targets MRSA and provides a continuous action to kill MRSA on contact for 6 hours. Suspicious lesions will be treated, covered and referred to parents with information to take to family physician. Contact History Inventory and implementation of disinfecting of specific facilities/equipment.
 which specifically targets MRSA and provides a continuous action to kill MRSA on contact for 6 hours. Suspicious lesions will be treated, covered and referred to parents with information to take to family physician. Contact History Inventory and implementation of disinfecting of specific facilities/equipment..")
29
What Can Parents Do? Encouraging good hygiene (i.e. hand washing: ollowing these tips can minimize the risk of infectious diseases including MRSA: 1.Clean clothes and equipment daily –Wash in warm water and dry completely in hot dryer –Spray equipment with diluted 1-5% bleach solution or commercial product (Lysol, i.e.) 2.Showering after all practices/competitions 3.Proper use and daily cleaning of water bottles 4.Check with your family physician if suspicious skin lesion 5.Read communicable disease info on ATP web site
 2.Showering after all practices/competitions 3.Proper use and daily cleaning of water bottles 4.Check with your family physician if suspicious skin lesion 5.Read communicable disease info on ATP web site.")
30
Nutrition Nutrition is often not a priority for teens Encourage sufficient water intake, proper eating habits--and adequate sleep! Proper Hydration is essential Top choices: WATER! (At least 64 oz./day) Gatorade / Sports Drinks Chocolate Milk (after exercise) There is no quick fix…real food is far better than any pill or supplement Avoid junk food. Provide a good balanced diet 60-70% CHO, 15-20% K, 10-15% fat
 Gatorade / Sports Drinks Chocolate Milk (after exercise) There is no quick fix…real food is far better than any pill or supplement Avoid junk food. Provide a good balanced diet 60-70% CHO, 15-20% K, 10-15% fat.")
31
Nutrition For serious athletes, and those with specific nutritional concerns, consultation with an registered dietician or sports nutritionist at least once in their athletic career is a great idea. Discourage the use of supplements; they are not regulated--may not state all ingredients, and usually are not appropriate for adolescents without consulting a physician or dietician. No FCPS employee may supply, endorse, or encourage the use of supplements.

32
BANNED Using products like these may disqualify a student from participating in contest

33
Anabolic Steroids Signs and Symptoms: Severe Acne, mood swings, aggression, depression, unusually fast strength/wt. gains, change in physical characteristics, among others. The consequences for being caught using steroids is 2 years disqualification from sports. (Virginia state law) Certified athletic trainers are a resource on negative health effects of Anabolic Steroids For more info visit http://taylorhooton.org/http://taylorhooton.org/
 Certified athletic trainers are a resource on negative health effects of Anabolic Steroids For more info visit")
34
Medications Inhalers, Epi Pens & any other Emergency Meds must be with athlete at all times. If they don’t have it, they should not play or practice until they get it The same authorization form you turn in to Health Room is used for us to hold medicines after school. Avoid giving your child prescribed or OTC pain medication before OR during a game. Masking pain may make existing or potential injury worse. NSAIDs may increase bleeding.Talk with your family doctor. Your Name

35
Concussion Education “bell rung” = “dinged” = Concussion It is an injury to the brain (or mTBI) Metabolic, physiological, or microscopic as opposed to visible physical damage. Therefore…A Negative CT Scan does NOT rule out or diagnose a concussion Can be life threatening if ignored Signs & Symptoms include : Headache, confusion, dizziness, change in personality, difficulty sleeping, difficulty concentrating, loss of appetite, loss of memory, “feeling foggy,” etc., etc. Concussions can alter a student’s ability to learn Most are resolved in one to two weeks although some can take much longer, especially if not proper rest. (at least 5 days regardless if cleared by MD)
.")
36
Concussion Management Concussions are managed on Individual Basis Standardized “sideline” tests at time of injury ACE Care Plan, Recommendation for rest, no school or partial days for initial period Clinical Evaluation Follow-ups Symptoms scores Vestibular/Balance and Vision Testing Computerized Neuro-cognitive Test is a web based concussion management tool used to help us identify if the brain has recovered to a point the athlete is safe to begin or continue a progressive return to sport. (Baseline tests are completed on Freshmen and Juniors.

37
Academic Instructional Strategies Are given to teachers through Counselor to assist teachers and students with return to full academic workload Step-wise return to play protocol, Usually 4-5 days to full return to play after all symptoms resolve. May be longer if had a lengthy inactive period Medical referral may be warranted for a prolonged recovery. (3 or 4 weeks without expected progress). Proper physical and mental rest, and reducing anxiety that athletes often feel when returning from concussion are key elements to recovery. Concussion Management
. Proper physical and mental rest, and reducing anxiety that athletes often feel when returning from concussion are key elements to recovery. Concussion Management.")
38
Concussion Management Resources Resources for Parents if AT not available or student having a prolonged recovery: SCORE Fairfax Office, Maegan Sady, PhD www.childrensnational.org/score www.childrensnational.org/score Dr. Scott Ross, MD, Manassas/S. Riding Fairfax Family Medicine Concussion Center, 703-391-2020 Pediatric Neuropsychology. www.fnapc.com/neuropsychology (Jillian Schneider, PhD)
.")
39
Announcements VHSL Sports Physicals at Robinson Tuesday, JUNE 9, 2015. This is Fundraiser, in which proceeds cover about 90% of AT budget for supplies and equipment used for all activities, sports and student-athletes. $50 donation Robinson Secondary Look for KIT message after spring break for on-line registration information Medical Professionals interested in volunteering for the first time? Please contact Mr. Perry or Dr. Childress.

40
On-Line Resources http://www.robinsonathletics.com Click on “Athletic Training” You are here! Check other tabs: News, Photos, Links, Files, health information www.fcps.edu/sports click on for more Sports Medicine information, forms, etc.www.fcps.edu/sports

Similar presentations


>")









 Prepared by: Kathryn Billings.>")






