Download presentation
Presentation is loading. Please wait.

1
Anaemia management Indian Scenaro
Dr

2
Estimates of prevalence of CKD in the USA: NHANES III
Stage Description GFR (ml/min/1.73 m2) Prevalence (%) 1 Kidney damage with normal or GFR 90 3.3 2 Kidney damage with mild GFR 60–89 3.0 3 Moderate GFR 30–59 4.3 4 Severe GFR 15–29 0.2 5 Kidney failure 15 or (or dialysis) 0.1 Coresh et al AJKD 2003
 Prevalence. (%) 1. Kidney damage with normal or GFR. Kidney damage with. mild GFR. 60– Moderate GFR. 30– Severe GFR. 15– Kidney failure. 15 or. (or dialysis) 0.1. Coresh et al AJKD")
3
EXTENT OF CKD IN INDIA India-diabetic capital. Every 5th Indian diabetic and every 5th Indian Hypertensive 40-50% of all chronic kidney disease is due to diabetes Prevalence of CKD Chennai- 0.16 Delhi- 0.78 Incidence of CKD per million population (Jha et al) 785 per million population (Agarwal et al)
 785 per million population (Agarwal et al)")
4
Cause of End Stage Renal Disease (SJMCH)
")
5
Challenges in Anaemia Management Many patients affected by anaemia
44 GFR (mL/min per 1.73 m2) n=15 625 Astor et al 2002
 n= Astor et al")
6
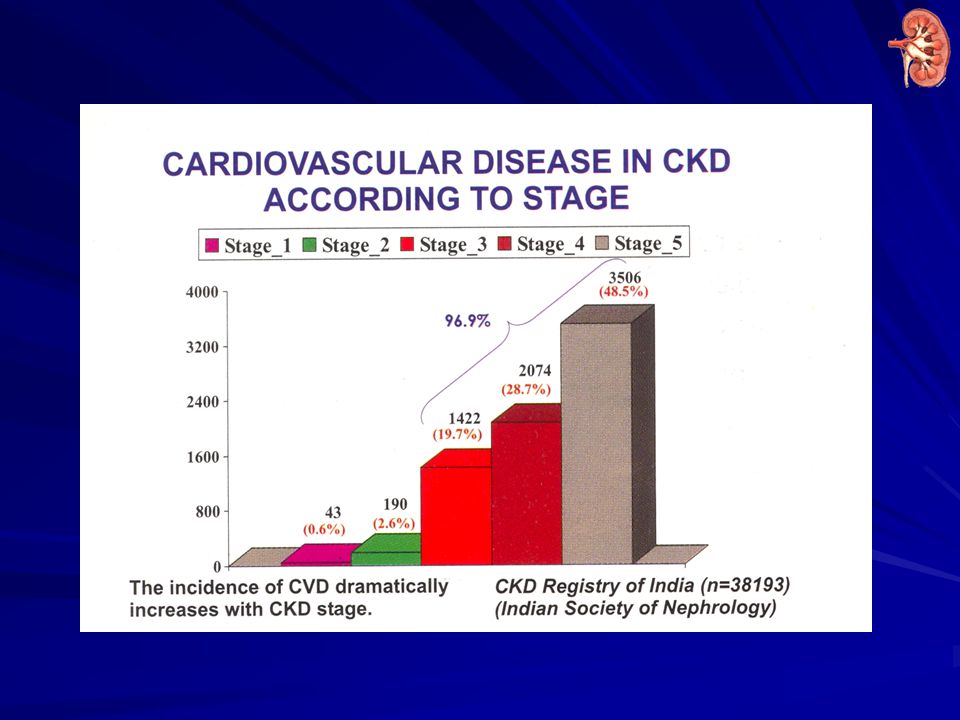
CKD REGISTRY INDIA

7
CORRECTION OF ANEMIA TARGET HAEMOGLOBIN =11-12 grams/dl

8
CKD Anaemia Correlates with Survival
Survival of CKD Patients by Haemoglobin Level Reproduced courtesy of A Levin

9
Association between renal anaemia and relative risk of death or hospitalisation
Relative risk of hospitalisation RR, overall=0.95 per 1 g/dl higher Hb (p=0.03) RR, overall=0.96 per 1 g/dl higher Hb (p=0.02) RR RR 1.29 1.09 1 1.07 1.22 1.02 1 0.91 p=0.06 p=0.86 Ref p=0.49 p<0.001 p=0.14 Ref p=0.44 Target of g/dl is appropriate Renal Anemia correlates with outcome (n) (1626) (952) (760) (682) (1521) (919) (733) (670) Hb (g/dl) at study entry Locatelli et al NDT 2004
 RR, overall=0.96 per 1 g/dl higher Hb (p=0.02) RR. RR p=0.06. p=0.86. Ref. p=0.49. p< p=0.14. Ref. p=0.44. Target of g/dl is appropriate. Renal Anemia correlates with outcome. (n) (1626) (952) (760) (682) (1521) (919) (733) (670) Hb (g/dl) at study entry. Locatelli et al NDT")
10
CKD REGISTRY INDIA

12
Problems in anemia management in CKD
Common challenges faced are – Maintenance of stable hemoglobin levels in their patients Avoid overshooting Hb targets Balance intravenous iron & EPO Improve EPO response to use the lowest effective EPO dose A major concern is EPO hyporesponsiveness & insufficient iron replacement IV iron is important in managing these challenges to a large extent Kapoian T. Challenge of effectively using erythropoiesis-stimulating agents and intravenous iron. Am J Kidney Dis Dec;52(6 Suppl):S21-8.
:S21-8.")
13
Challenges in Anaemia Management Worldwide prevalence and incidence of CKD
More than 1.7 million treated with renal replacement therapy worldwide in 2004 90% patients receiving RRT live in industrialized countries The incidence of CKD requiring renal replacement therapy has doubled over the last 15 years Dramatically increasing prevalence predicted in the next 10 years largely due to the aging population and increasing incidence of type 2 diabetes El Nahas & Bello 2005 Grassmann et al 2005

14
Challenges in Anaemia Management CKD incidence and prevalence increasing
No. of patients (thousands) Prevalent dialysis and transplant (2002: ) Prevalent dialysis (2002: ) Prevalent transplant (2002: ) Incident dialysis and transplant (2002: ) Year USRDS 2004 Annual Data Report
 Prevalent dialysis and transplant (2002: ) Prevalent dialysis (2002: ) Prevalent transplant (2002: ) Incident dialysis and transplant (2002: ) Year. USRDS 2004 Annual Data Report.")
15
Challenges in Anaemia Management Undertreatment of anaemia remains
Mean Hb (g/dL) Prevalent 13 Incident 12 11 10 9 8 7 6 USA Italy UK Sweden Spain France Japan Belgium Canada Germany Australia / NZ Locatelli et al 2004 Pisoni et al 2004
 Prevalent. 13. Incident USA. Italy. UK. Sweden. Spain. France. Japan. Belgium. Canada. Germany. Australia / NZ. Locatelli et al 2004 Pisoni et al")
16
Challenges in Anaemia Management Many patients below Hb target
Prevalent (%) Patients with Hb <11 g/dL Incident Sweden USA Spain Belgium Canada Australia / NZ Germany Italy UK France Japan 10 20 30 40 50 60 70 80 90 100 Locatelli et al 2004 Pisoni et al 2004
 Patients with Hb <11 g/dL. Incident. Sweden. USA. Spain. Belgium. Canada. Australia / NZ. Germany. Italy. UK. France. Japan Locatelli et al 2004 Pisoni et al")
18
Mark A. Parazella,MD. CKD series: evaluation and treatment of anemia in chronic kidney disease. Hospital physician. 2003; 31-38,46

19
Mark A. Parazella,MD. CKD series: evaluation and treatment of anemia in chronic kidney disease. Hospital physician. 2003; 31-38,46

20
INDIAN BEST PRACTICE GUIDELINES

21
Indian Best Practices Guidelines
Anaemia in CRF can be due to multiple causes, most commonly EPO deficiency and nutritional factors. Since EPO is expensive, all efforts must be made to correct nutritional deficiencies especially iron deficiency and assessment of other nutritional factors.

22
Guideline 1: Anaemia Evaluation (Evidence level A)
RBC indices / Peripheral smear Iron / TIBC / Ferritin / Tranferrin saturation Stool occult blood Stool parasite test Serum B12 & Red cell folate concentrations

23
Guideline 1 (a): Anaemia Evaluation
RBC indices / Peripheral smear Iron / TIBC / Ferritin / Tranferrin saturation Stool occult blood Stool parasite test A fuller work up should also include the following as indicated. Serum B12 and red cell folate concentrations Differential white blood count Tests for haemolysis (haptoglobin, lactate dehydrogenase)
")
24
Guideline 1 (a): Anaemia Evaluation (contd..)
Serum and / or urine protein electrophoresis / immunoblotting (where available). Serum aluminium Bone marrow examination in selected cases Assessment of occult gastrointestinal blood loss. Elements of this work up will be necessary if there is clinical suspicion of primary haematological disorder (haemolysis, marrow dysplasia), macrocytosis, aluminium poisoning or occult blood loss). (Evidence level A)
. Serum aluminium. Bone marrow examination in selected cases. Assessment of occult gastrointestinal blood loss. Elements of this work up will be necessary if there is clinical suspicion of primary haematological disorder (haemolysis, marrow dysplasia), macrocytosis, aluminium poisoning or occult blood loss). (Evidence level A)")
25
Guideline 2(a): Diagnosis of Anaemia of Chronic Renal Failure
No cause other than CRF by above investigation. GFR <30 in non-diabetics and 45ml/min. in diabetic patients (S. creat >2mg/dl). Measurement of plasma EPO concentration not indicated.
. Measurement of plasma EPO concentration not indicated.")
26
Guideline 7: What are the causes of inadequate response to EPO. (contd
vi) Hemolysis Vii) Osteitis fibrosa viii) Aluminium toxicity ix) Haemoglobinopathies (e.g. alpha & Beta thalassemias, sickle cell anaemia) x) Multiple myeloma & other malignancies. xi) Use of ACE-1 / ARB agents
 Hemolysis. Vii) Osteitis fibrosa. viii) Aluminium toxicity. ix) Haemoglobinopathies (e.g. alpha & Beta thalassemias, sickle cell anaemia) x) Multiple myeloma & other malignancies. xi) Use of ACE-1 / ARB agents.")
27
Guideline 7(a): Resistance to EPO / inadequate response to EPO
Failure to achieve target Hb concentration a) While receiving more than 300IU/kg/week S.C or units IU/kg/week IV. b) Continued need for such dosage to maintain target in presence of adequate iron stores. Resistance (hypo responsiveness) is relative In the absence of detectable abnormalities of any one of the above conditions – marrow examination is indicated (for diagnosis of resistance) including haematologist reference.
 While receiving more than 300IU/kg/week S.C or 450units IU/kg/week IV. b) Continued need for such dosage to maintain target in presence of adequate iron stores. Resistance (hypo responsiveness) is relative. In the absence of detectable abnormalities of any one of the above conditions – marrow examination is indicated (for diagnosis of resistance) including haematologist reference.")
28
ROLE OF IRON

29
Need for IV iron in CKD Iron deficiency in CKD patients develops primarily during the correction of renal anemia by EPO treatment Among ESRD patients receiving EPO, more than 50% are iron deficient Approximately 150 mg of iron is necessary for an increase of 1 g/dl in hemoglobin level Causes of anemia in CKD patients include – Inadequate intake of dietary iron Blood loss during the extracorporeal procedure GI bleeding Inadequate intestinal iron absorption and inhibition of iron release from macrophages Increased iron requirements during therapy with erythropoiesis-stimulating agents (ESAs). Horl WH. Iron therapy for renal anemia: how much needed, how much harmful? Pediatr Nephrol 2007;22:480–9. Guidelines for anemia of chronic kidney disease. NKF K/DOQI guidelines Available at:
. Horl WH. Iron therapy for renal anemia: how much needed, how much harmful Pediatr Nephrol 2007;22:480–9. Guidelines for anemia of chronic kidney disease. NKF K/DOQI guidelines Available at:")
30
IV iron in CKD IV iron therapy is superior to oral iron supplementation in CKD Risk factors associated with IV iron therapy acute allergic reactions long-term complications caused by the generation of powerful oxidant species, Allergy is to related to dextran moiety Iron dextran is associated with higher incidence of Type I hypersensitivity than Iron sucrose Iron sucrose carries the lowest risk for hypersensitivity 1. Horl WH. Iron therapy for renal anemia: how much needed, how much harmful? Pediatr Nephrol 2007;22:480–9.

31
Iron sucrose in kidney disease
Iron deficiency may be corrected by oral iron supplementation but it is limited by – Poor compliance Adverse gastrointestinal reactions IV iron preparations commonly used include iron sucrose, sodium ferric gluconate, & iron dextran Iron sucrose is safer than iron dextran, is generally considered a safe and effective IV iron preparation in renal anemia 1. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54.

32
Iron sucrose in kidney disease
Iron sucrose is a novel and effective addition in the management of ‘Anemia related to kidney diseases’ Iron Sucrose is elemental iron which replenishes body iron stores in patients with iron deficiency Approximately 25% of hemodialysis patients can be maintained on oral iron supplementation; the others require IV iron supplementation 1. Dennis J. Cada. Iron Sucrose Injection. Drug Reviews From The Formulary, Volume 36, April 2001, 2. W.H. Horl, OPTA-therapy with iron and erythropoiesis-stimulating agents in chronic kidney disease, nephrology dial transplant suppl 3;iii2-iii6

33
Indications IV iron sucrose is indicated in –
Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients receiving an erythropoietin Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients not receiving an erythropoietin Hemodialysis Dependent - Chronic Kidney Disease (HDD-CKD) patients receiving an erythropoietin Peritoneal Dialysis Dependent - Chronic Kidney Disease (PDD-CKD) patients receiving an erythropoietin 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007. 2. Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): 3. Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4.
 patients receiving an erythropoietin. Non-Dialysis Dependent - Chronic Kidney Disease (NDD-CKD) patients not receiving an erythropoietin. Hemodialysis Dependent - Chronic Kidney Disease (HDD-CKD) patients receiving an erythropoietin. Peritoneal Dialysis Dependent - Chronic Kidney Disease (PDD-CKD) patients receiving an erythropoietin. 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; Hollands JM et al. Safety of High-Dose Iron Sucrose Infusion in Hospitalized Patients With Chronic Kidney Disease. Am J Health-Syst Pharm. 2006;63(8): Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:")
34
Iron sucrose in pre-dialysis CRF patients
Patients undergoing chronic hemodialysis often present with anemia IV iron therapy is administered in conjunction with EPO as it helps prevent EPO-hypo-responsiveness Study evaluated use of Iron sucrose in pre dialyzed patients of CRF 60 non-diabetic CRF patients were included in the study Mircescu G ,et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4.

35
Results 60 patients included in the study
58% of patients reporting a rise in Hb > 1 g/dL vs. baseline in the study 80% of patients had a Hb > 10 g/dL vs. 44% at baseline 55% had a Hb > 11 g/dL vs. 0% at baseline Mean serum iron concentration increased from – 73.9 µg/dL at baseline 84.2 µg/dL at 6 months 101.8 µg/dL at 12 months of therapy No worsening of renal function, and no adverse events were reported Mircescu G et al. Intravenous iron supplementation for the treatment of anaemia in pre-dialyzed chronic renal failure patients. Nephrol Dial Transplant 2006;21:120-4.

36
Efficacy of Iron sucrose in hemodialysis patients
Schiesser et al conducted a prospective multicentre clinical trial in 50 iron-replete hemodialysis patients to evaluate the efficacy of iron sucrose administration for 6 months Hb level remained stable (12±1.1 at baseline & 12.1±1.5 g/dl at the end of the study) Reduced dose for EPO Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5.
 Reduced dose for EPO. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5.")
37
Iron sucrose IV reduces EPO demand in dialysis patients
In the study of Iron sucrose in hemodialysis patients conducted by Schiesser et al the dosage for the three different epoetins decreased by – 38.5% with darbepoetin alfa 6.3% with epoetin alfa 8.3% with epoetin beta Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5.
 21: 2841–5.")
38
Results showing reduced EPO need with iron sucrose
Schiesser et al showed reduced EPO need with low dose maintenance iron sucrose in their study Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–5.
 21: 2841–5.")
39
IV iron reduces EPO demand in dialysis patients
Chang et al studies the beneficial effects of 2 weekly IV iron supplementation compared to once monthly IV iron in 149 iron replete patients EPO requirement reduced by 25% when sereum ferritin & Transferrin saturation was maintained at high levels by administering 2 weekly IV iron compared to IV iron given once monthly Significant decrease in serum albumin, cholesterol & pre-dialysis creatinine when IV iron was administered 2 weekly for 1 year Chang CH et al. Reduction in erythropoietin doses by the use of chronic intravenous iron supplementation in iron-replete hemodialysis patients. Clin Nephrol. 2002;57:

40
IV iron reduces EPO demand in dialysis patients – Results from Meta analysis
Compared to oral iron IV iron preparations significantly reduce the EPO requirement in dialysis patients Rozen-Zvi et al. Intravenous Versus Oral Iron Supplementation for the Treatment of Anemia in CKD: Systematic Review and Meta-analysis. American Journal of Kidney Diseases 2008;52:

41
Iron sucrose in CKD patients not on dialysis
Charytan et al compared oral iron with Iron sucrose in 96 NDD-CKD patients More IV iron patients (54.2%) attained hemoglobin values > 11.0 g/dl compared to oral iron patients (31.3%) There were no serious side effects with iron sucrose Charytan C et al. Comparison of intravenous iron sucrose to oral iron in the treatment of anemic patients with chronic kidney disease not on dialysis. Nephron Clin Pract. 2005;100(3):c55-62.
 attained hemoglobin values > 11.0 g/dl compared to oral iron patients (31.3%) There were no serious side effects with iron sucrose. Charytan C et al. Comparison of intravenous iron sucrose to oral iron in the treatment of anemic patients with chronic kidney disease not on dialysis. Nephron Clin Pract. 2005;100(3):c")
42
Efficacy & safety of Iron sucrose in peritoneal dialysis patients
Li et al conducted a study to compare the clinical outcomes & safety of IV iron sucrose & oral ferrous succinate in combination with rHuEPO therapy in patients on maintenance PD 46 patients were included – 26 received iron sucrose & 20 oral iron Hb & Hct increased significantly at 2 weeks in the IV group compared with baseline The total response rate at 8 weeks was 94.8% for the IV group - significantly higher than that of the oral group (55.0%) There were no adverse events with IV iron 8 patients in the oral group had adverse GI effects Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54.
 There were no adverse events with IV iron. 8 patients in the oral group had adverse GI effects. Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54.")
43
Results of Iron sucrose in PD patients contd.
Response rates to IV iron sucrose therapy compared to Oral iron therapy Li H. Intravenous iron sucrose in peritoneal dialysis patients with renal anemia. Peritoneal Dialysis International 2008;28:149–54.

44
Efficacy of Iron sucrose in ESRD
Iron sucrose in apparently iron-replete patients will decrease the EPO requirements for a given target hematocrit in patients on maintenance hemodialysis with end-stage renal disease (ESRD) 1. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841–2845. 2. Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–25.
 1. Schiesser et al. Weekly low-dose treatment with intravenous iron sucrose maintains iron status and decreases epoetin requirement in iron-replete haemodialysis patients. Nephrol Dial Transplant (2006) 21: 2841– Shaldon S. The use of IV iron in the treatment of anaemia of ESRD patients on maintenance haemodialysis: an historical and personal view. Nephrol Dial Transplant (2007) 22: 23–25.")
45
Safety of Iron sucrose Aronoff et al studied the safety of iron sucrose in hemodialysis patients 665 hemodialysis patients with 80 who had experienced previous intolerance to other IV iron preparations were given iron sucrose There were no serious or life-threatening drug-related adverse events Aronoff GR et al. Iron sucrose in hemodialysis patients: Safety of replacement and maintenance regimens. Kidney International, 2004;66:1193–8.

46
Iron sucrose in patients hypersensitive to iron dextran
Iron dextran has been the only available parenteral iron preparation for a long time Its use has been associated with increased risk of allergic reactions, even after reaction-free previous use Haddad A et al. Use of Iron Sucrose in Dialysis Patients Sensitive to Iron Dextran. Saudi J Kidney Dis Transpl 2009;20(2):
:")
47
Safety of Iron sucrose compared to other iron preparations
Rates of life-threatening ADEs – 0.6 per million for iron sucrose 0.9 per million for sodium ferric gluconate complex 3.3 per million for lower molecular weight iron dextran 11.3 per million per million for higher molecular weight iron dextran Chertow GM et al. Update on adverse drug events associated with parenteral iron. Nephrol Dial Transplant (2006) 21: 378–382.
 21: 378–382.")
48
Dosing and administration
NDD-CKD - Administered as a total cumulative dose of 1,000 mg over a 14 days as a 200 mg slow IV injection undiluted over 2 to 5 minutes on 5 different occasions. HDD-CKD - Administered undiluted as a 100 mg slow IV over 2 to 5 minutes or as an infusion of 100 mg, diluted in a maximum of 100 mL of NS over 15 minutes per consecutive hemodialysis session for a total cumulative dose of 1,000 mg. 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007.

49
Dosing and administration contd.
PDD-CKD - Administered undiluted as a total cumulative dose of 1,000 mg in 3 divided doses, given by slow IV infusion, over 28 days: 2 infusions of 300 mg over 1.5 hs 14 days apart Followed by mg infusion over 2.5 h 14 days later Should be diluted in 250 mL of NS Low maintenance doses in hemodialysis patients include 50mg injected into the venous limb of the haemodialysis tubing system (slow intravenous push at a rate of 10 mg/min) 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.; 2007.
 1. Venofer® [package insert]. Shirley, NY: American Regent, Inc.;")
50
Dosing and administration contd.
The usual dose is 100 mg administered one to three times per week. Most patients will require a minimum cumulative dose of 1000 mg of elemental iron administered over 10 sequential dialysis sessions to achieve a favorable response Patients may continue to receive IV iron therapy at the lowest dose necessary to maintain target levels of hemoglobin, hematocrit & iron storage parameters Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12.

51
Monitoring parameters
Patients receiving regular IV iron therapy require monitoring of hematologic parameters & iron indices (Hb, Hct, TSAT, & ferritin) Maintain TSAT between 20% and 50% Iron therapy should be withheld in patients with TSAT ≥50% Iron therapy should be withheld in patients with ferritin values ≥800 ng/mL Since transferrin saturation values increase rapidly after IV administration of iron sucrose, serum iron values may be reliably obtained 48 hours after IV iron sucrose dosing Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12.
 Maintain TSAT between 20% and 50% Iron therapy should be withheld in patients with TSAT ≥50% Iron therapy should be withheld in patients with ferritin values ≥800 ng/mL. Since transferrin saturation values increase rapidly after IV administration of iron sucrose, serum iron values may be reliably obtained 48 hours after IV iron sucrose dosing. Cada DJ. Iron Sucrose Injection. Hospital Pharmacy 2001;36:404–12.")
52
INDIAN BEST PRACTICE GUIDELINES … contd

53
Guideline 9: When to assess iron status after EPO therapy
Iron status must be assessed once in 3 months while on EPO therapy.

54
Guideline 9(a): When to assess iron status after EPO therapy?
CKD patients should have sufficient iron stores to maintain target Hb% (Evidence). To achieve this, sufficient iron to be administered. to maintain TSAT>20% Ferritin >100ng/ml
. To achieve this, sufficient iron to be administered. to maintain TSAT>20% Ferritin >100ng/ml.")
55
Guideline 9(a): When to assess iron status after EPO therapy? (contd..)
To achieve this level, aim at - TSAT 30-40% - Ferritin ng/ml (Evidence level B) No benefit is achieved if TSAT >50% & serum ferritin >800ng/ml and iron should not be administered beyond this level (Evidence B)
 No benefit is achieved if TSAT >50% & serum ferritin >800ng/ml and iron should not be administered beyond this level (Evidence B)")
56
Monitoring iron stores & supplement Iron
1. During initiation of EPO & increased dose of EPO. TSAT / serum ferritin to be checked every month in patients not receiving IV iron or once in three months in those receiving IV iron (opinion). Once target Hb% achieved, check iron stores once in 3 months.
. Once target Hb% achieved, check iron stores once in 3 months.")
57
Monitoring iron stores & supplement Iron (contd..)
In doses of not more than 125mg IV Dextran, no interruption of treatment to check iron stores (Evidence). 4. However with large doses (1000mg IV Dextran), a gap of 2 weeks after stopping IV iron, to be ensured to check stores (Evidence). 5. CKD patients not treated with EPO with TSAT >20%, ferritin >100ng/ml, Iron stores to be checked once 3-6 months (opinion).
. 4. However with large doses (1000mg IV Dextran), a gap of 2 weeks after stopping IV iron, to be ensured to check stores (Evidence). 5. CKD patients not treated with EPO with TSAT >20%, ferritin >100ng/ml, Iron stores to be checked once 3-6 months (opinion).")
58
Key points Anemia in CKD patients is common
EPO therapy forms the mainstay of treatment EPO therapy alone may be ineffective unless supplemented by iron Oral iron supplementation has problems of intolerance IV iron forms the best adjunct with EPO in CKD patients.

59
Key points IV iron sucrose is one of the iron preparations
It is indicated in hemodialysis patients, non hemodialysis patients with or without EPO and peritoneal dialysis patients Efficacy is proved in each of these indications Low maintenance dose of Iron sucrose keeps Hb and Hct stable in hemodialysis patients

60
Key points Iron sucrose administration along with EPO reduces the dose requirement of EPO Iron sucrose can be safely given to patients hypersensitive to iron dextran Iron sucrose is safer than other IV iron preparations

61
Laboratory and transfusion data
Parameter HD PD P (n=157) (n=126) value Hemoglobin (g/dl) 10.47 10.71 0.45 Serum ferritin (g/dl) 258.7 253.8 0.77 Transferrin saturation (%) 28.5 28.1 0.94 n = 56 Mean number of transfusions (units) 4.59 2.17 0.01 % of patients receiving at least one transfusion 52.9% 40.9% 0.01 % of patients receiving transfusion if requiring 59.5% 37.5% 0.02 n = 45 between 6,000 and 10,000 units rHuEpo per week Conclusion: Patients receiving renal replacement therapy with HD received more blood transfusions and more rHuEpo to maintain the same hemoglobin as compared to those treated with PD. House AA, et al, Nephrol Dial Transplant, 1998; 13:
 (n=126) value. Hemoglobin (g/dl) Serum. ferritin (g/dl) Transferrin saturation (%) n = 56. Mean number of transfusions (units) % of patients receiving at least one transfusion. 52.9% 40.9% % of patients receiving transfusion if requiring. 59.5% 37.5% n = 45. between 6,000 and 10,000 units. rHuEpo per week. Conclusion: Patients receiving renal replacement therapy with HD received more blood transfusions and more rHuEpo to maintain the same hemoglobin as compared to those treated with PD. House AA, et al, Nephrol Dial Transplant, 1998; 13:")
62
Patients on EPO n = 45 n = 56 n = 56 n = 56 n = 45
Gokulnath et al, IJPD,16:22-28;2008

63
Patients on EPO n = 56 n = 56 n = 56 n = 45 n = 45
Gokulnath et al, IJPD,16:22-28;2008

64
Patients on EPO (IU/kg/wk)
Gokulnath et al, IJPD,16:22-28;2008

65
Patients on Serum Iron (mg)
Gokulnath et al, IJPD,16:22-28;2008

66
Blood Transfusions in patients on Maintenance HD / CAPD
Cohort followed up 30 months Gokulnath et al, IJPD,16:22-28;2008

67
STEM CELL THERAPY FUTURE?

68
Thank you

Similar presentations












 Sofia Medical University. Background Erythropoiesis-stimulating agents are man-made versions of a natural protein known as erythropoietin.>")




 Kingsbrook Jewish Medical Center Clinical Instructor of Pharmacy Practice.>")

