Download presentation
Presentation is loading. Please wait.

1
Advocacy, Communication, and Social Mobilization to Fight XDR TB
Wanda Walton, PhD, MEd Communications, Education, and Behavioral Studies Branch Division of Tuberculosis Elimination

2
ACSM to Address Key Challenges to TB Control at Country Level
Improving case detection and treatment adherence Combating stigma and discrimination Empowering people affected by TB Mobilizing political commitment and resources for TB

3
Framework for ACSM to Address Key Challenges to TB Control at Country Level
Building national and subnational ACSM capacity Building inclusion of patients and affected communities Ensuring political commitment and accountability Building country-level ACSM partnerships Learning, adapting, and building on good ACSM practice

4
Advocacy, Communication, and Social Mobilization for XDR TB
Communication to exchange information about XDR TB, informing and creating awareness Advocacy to place XDR TB control high on the political agenda, foster political will, increase financial and other resources, e.g., human resources Social mobilization to bring together allies to raise awareness and demand for program needs, assist in delivery of resources and services, create sustainable change

5
XDR TB Extensive (or Extreme) Drug Resistant TB
MDR TB - defined as TB resistant to at least the 2 most potent anti-TB drugs, isoniazid and rifampicin (first-line drugs) XDR TB* - defined as MDR TB that is also resistant to at least 3 of the 6 classes of second-line drugs *Definition may change based upon recommendations of expert panel
 XDR TB* - defined as MDR TB that is also resistant to at least 3 of the 6 classes of second-line drugs. *Definition may change based upon recommendations of expert panel.")
6
Drugs for the Treatment of TB
1. Isoniazid 2. Rifampicin 3. Pyrazinamide 4. Ethambutol 5. Aminoglycosides 6. Capreomycin 7. Quinolones 8. Thioamides 9. Cycloserine 10. PAS

7
First-line drugs and treatment of drug-susceptible TB
1. Isoniazid 2. Rifampicin 3. Pyrazinamide 4. Ethambutol 5. Aminoglycosides 6. Capreomycin 7. Quinolones 8. Thioamides 9. Cycloserine 10. PAS Standardized treatment of “routine” drug-susceptible TB 4 drugs, 6-9 months Safe, effective, inexpensive 95% cure, $20 (drug costs) Based on solid scientific evidence from ~ 30 years of drug discovery and controlled clinical trials,
 Based on solid scientific evidence from ~ 30 years of drug discovery and controlled clinical trials,")
8
Second-Line Drugs and Treatment of Multidrug-Resistant TB
1. Isoniazid 2. Rifampicin 3. Pyrazinamide 4. Ethambutol 5. Aminoglycosides 6. Capreomycin 7. Quinolones 8. Ethionamide 9. Cycloserine 10. PAS Treatment based on laboratory drug-resistance testing and epidemiology information 4-6 drugs, 2 years Less effective, more toxic, expensive - 65%-75% cure - $3500 (drug costs) No clinical trials evidence to guide treatment or prevention
 No clinical trials evidence to guide treatment or prevention.")
9
Extensive drug resistance
Drug Susceptible Multidrug resistance Extensive drug resistance Isoniazid Rifampicin Pyrazinamide Ethambutol Aminoglycosides Capreomycin Quinolones Thioamides Cycloserine PAS Resistance by definition Resistance possible or likely

10
Extensive Drug Resistance Among MDR TB Isolates Submitted to 14 Supranational Reference Labs, by Region 2000–2004 Geographic Region Total MDR TB isolates (n) XDR TB n ( % ) Industrialized nations Latin America Eastern Europe Africa and Middle East Asia 821 543 406 156 1,572 53 ( 6 ) 32 ( 6 ) 55 ( 14 ) 1 ( <1 ) 204 ( 13 ) Total 3,418 345 (10) When looking at the geographic distribution of the XDR TB isolates, we categorized countries into epidemiological groups based on similar rates of MDR TB prevalence. Isolates were received from all major regions of the world. Among the group of industrialized nations, 6% of MDR TB isolates met criteria for XDR TB. Among MDR TB isolates from countries in Latin America, again 6% met the definition of XDR TB. From the countries of the Eastern Europe where rates of MDR TB are among the highest in the world, 14% of MDR TB isolates were XDR TB. Looking at the population level data in South Korea, 15% of MDR TB isolates – or 2% of all TB isolates tested in South Korea – met criteria for XDR TB.
 XDR TB n ( % ) Industrialized nations. Latin America. Eastern Europe. Africa and Middle East. Asia , ( 6 ) 32 ( 6 ) 55 ( 14 ) 1 ( <1 ) 204 ( 13 ) Total. 3, (10) When looking at the geographic distribution of the XDR TB isolates, we categorized countries into epidemiological groups based on similar rates of MDR TB prevalence. Isolates were received from all major regions of the world. Among the group of industrialized nations, 6% of MDR TB isolates met criteria for XDR TB. Among MDR TB isolates from countries in Latin America, again 6% met the definition of XDR TB. From the countries of the Eastern Europe where rates of MDR TB are among the highest in the world, 14% of MDR TB isolates were XDR TB. Looking at the population level data in South Korea, 15% of MDR TB isolates – or 2% of all TB isolates tested in South Korea – met criteria for XDR TB.")
11
XDR TB Awareness and Emergency Response
Oral and poster presentations at IUATLD conference, November 2005 CDC report on Emergence of Mycobacterium tuberculosis with Extensive Resistance to Second-Line Drugs --- Worldwide, , March 24, 2006 16th International AIDS Conference presentation, August 2006 Global alert issued by WHO on emerging threat of highly lethal strains of drug resistant TB (XDR TB) on September 5, 2006 Emergency experts’ meeting (MRC, WHO, CDC) in Johannesburg, SA on September 7-8 Call for Global XDR TB Task Force in Geneva, first meeting October 2006
 on September 5, Emergency experts’ meeting (MRC, WHO, CDC) in Johannesburg, SA on September 7-8. Call for Global XDR TB Task Force in Geneva, first meeting October")
12
XDR TB in KwaZulu-Natal Province (KZN), South Africa
Reports of high mortality from TB in ARV treatment program in KZN in 2005 Team of collaborators invited to identify problem Investigators preformed cross-sectional study of TB suspects attending rural hospital 1539 patient isolates, 544 diagnosed with M.tb Of these, 221 (41%) MDR TB Of these, 53 (24%) XDR TB Of these patients, 26 had no h/o TB treatment; 44 of 44 tested were HIV infected; 52 (98%) died; 15 were on ARVs XDR TB now documented in 28 health care institutions throughout KNZ
 MDR TB. Of these, 53 (24%) XDR TB. Of these patients, 26 had no h/o TB treatment; 44 of 44 tested were HIV infected; 52 (98%) died; 15 were on ARVs. XDR TB now documented in 28 health care institutions throughout KNZ.")
13
Expert Consultation on Drug Resistant Tuberculosis
Expert Consultation organized by Medical Research Council (MRC) to strategize steps forward in Southern Africa Development Community (SADC) countries to address problem of drug resistance, September 7-8, 2006 Convened by Medical Research Council, Republic of South Africa (RSA) Department of Health Key stakeholders with experience in drug-resistant TB response – WHO, CDC (DTBE and RSA GAP), KNCV Representatives from all 9 provinces of RSA Representatives from 10 SADC countries
 to strategize steps forward in Southern Africa Development Community (SADC) countries to address problem of drug resistance, September 7-8, Convened by Medical Research Council, Republic of South Africa (RSA) Department of Health. Key stakeholders with experience in drug-resistant TB response – WHO, CDC (DTBE and RSA GAP), KNCV. Representatives from all 9 provinces of RSA. Representatives from 10 SADC countries.")
14
Expert Consultation 7-Point Plan: Short Term Response
“Improve function and performance of national TB programs to strengthen treatment adherence and achieve high rates of treatment completion for all TB patients” Develop national emergency response plan for MDR/XDR TB within 3 months Conduct rapid surveys of MDR TB and XDR TB within the next 3-6 months Strengthen and expand current national TB laboratory capacity Urgently implement broad infection control practices in health care facilities with special emphasis on those facilities providing care for PLWHA

15
7-Point Plan: Long Term Response
Establish capacity for clinical public health managers to effectively respond to MDR/XDR TB Promote universal access to ARVs for all TB patients through collaboration with HIV/AIDS treatment and care programs Support an increase in research for anti-TB drug development and rapid diagnostic test development for MDR/XDR TB

16
XDR TB is a significant threat to the major gains made in global TB control.
World Health Organization

17
Individuals with TB, including XDR TB, are human beings with human rights. We must treat all people with TB with respect, preserve their dignity, and save their lives. There is no role for stigma and discrimination in managing TB. Professor Gavin Churchyard Director, Aurum Institute for Health Research

18
TB Disease Latent TB Infection

19
XDR TB MDR TB

22
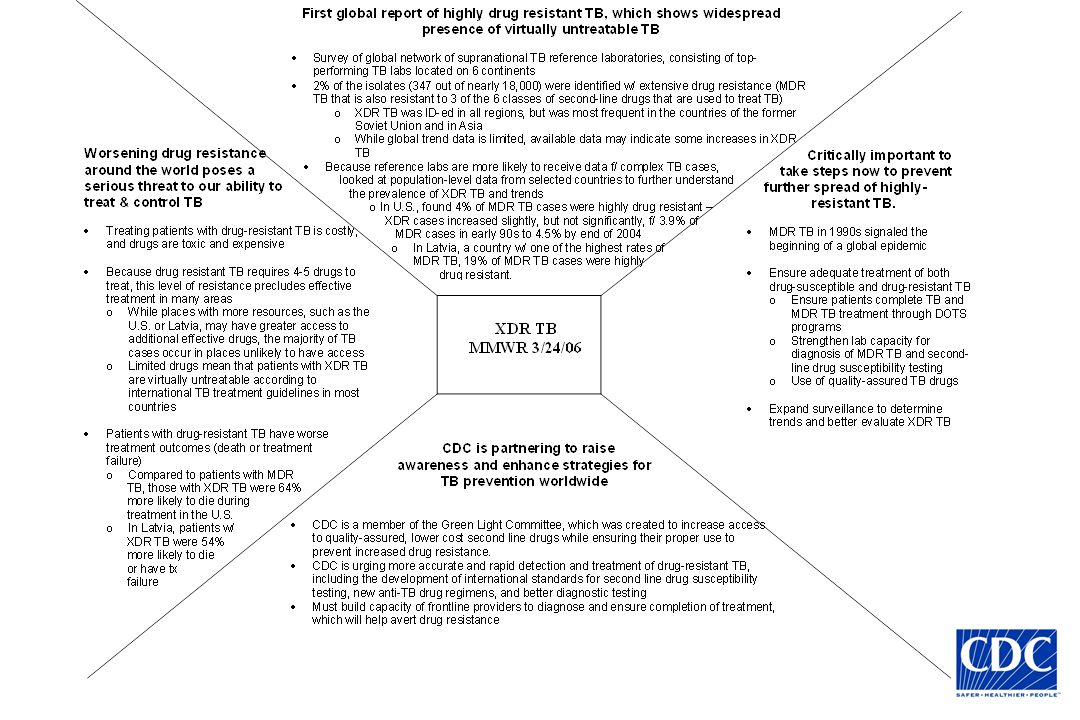
XDR TB Messages First global report of highly drug resistant TB, which shows widespread presence of virtually untreatable TB Survey of global network of supranational TB reference laboratories, located on 6 continents 2% of the isolates (347 out of nearly 18,000) were identified w/ extensive drug resistance XDR TB was ID-ed in all regions, but was most frequent in the countries of the former Soviet Union and in Asia While global trend data is limited, available data may indicate some increases in XDR TB In U.S., found 4% of MDR TB cases were highly drug resistant In Latvia, MDR TB, 19% of MDR TB cases were highly drug resistant
 were identified w/ extensive drug resistance. XDR TB was ID-ed in all regions, but was most frequent in the countries of the former Soviet Union and in Asia. While global trend data is limited, available data may indicate some increases in XDR TB. In U.S., found 4% of MDR TB cases were highly drug resistant. In Latvia, MDR TB, 19% of MDR TB cases were highly drug resistant.")
23
XDR TB Messages Worsening drug resistance around the world poses a serious threat to our ability to treat & control TB Treating patients with drug-resistant TB is costly, and drugs are toxic and expensive Because drug resistant TB requires 4-5 drugs to treat, this level of resistance precludes effective treatment in many areas While places with more resources, such as the U.S. or Latvia, may have greater access to additional effective drugs, the majority of TB cases occur in places unlikely to have access Limited drugs mean that patients with XDR TB are virtually untreatable according to international TB treatment guidelines in most countries

24
XDR TB Messages Worsening drug resistance around the world poses a serious threat to our ability to treat & control TB (2) Patients with drug-resistant TB have worse treatment outcomes (death or treatment failure) Compared to patients with MDR TB, those with XDR TB were 64% more likely to die during treatment in the U.S. In Latvia, patients w/ XDR TB were 54% more likely to die or have tx failure In KZN, 98% of patients with XDR TB and HIV infection died, despite adequate response to ARVs
 Compared to patients with MDR TB, those with XDR TB were 64% more likely to die during treatment in the U.S. In Latvia, patients w/ XDR TB were 54% more likely to die or have tx failure. In KZN, 98% of patients with XDR TB and HIV infection died, despite adequate response to ARVs.")
25
XDR TB Messages Critically important to take steps now to prevent further spread of highly-resistant TB MDR TB in 1990s signaled beginning of a global epidemic Ensure adequate treatment of both drug-susceptible and drug-resistant TB Ensure patients complete TB and MDR TB treatment through DOTS programs Strengthen lab capacity for diagnosis of MDR TB and second-line drug susceptibility testing Use of quality-assured TB drugs Expand surveillance to determine trends and better evaluate XDR TB Must have adequately functioning TB programs to address problem Implement broad infection control precautions Additional resources (human and financial)
")
26
XDR TB Messages CDC is partnering to raise awareness and enhance strategies for TB prevention worldwide CDC is a member of the Green Light Committee, created to increase access to quality-assured, lower cost second line drugs while ensuring their proper use to prevent increased drug resistance CDC is urging more accurate and rapid detection and treatment of drug-resistant TB, including the development of international standards for second line drug susceptibility testing, new anti-TB drug regimens, and better diagnostic testing Must build capacity of frontline providers to diagnose and ensure completion of treatment, which will help avert drug resistance

27
XDR TB Messages CDC is partnering to raise awareness and enhance strategies for TB prevention worldwide (2) New messages Participation in expert consultation with WHO and MRC Consensus plan of action Strengthen the laboratory Train the health care workers

28
Media Quotes in U.S.: March 24, 2006
Dr. Kenneth Castro, director of the CDC's division of TB elimination, said emergence of a super-resistant strain is a potent reminder that tuberculosis remains a formidable threat. "It is widely distributed geographically, including in the United States, and renders patients virtually untreatable," Castro said. Dr. Marcos Espinal, executive secretary of WHO's TB elimination program, called XDR TB a veritable death sentence. "If people are failing first- and second-line drugs and we don't have in the pipeline a new drug for immediate use, that's a crisis," he said.

29
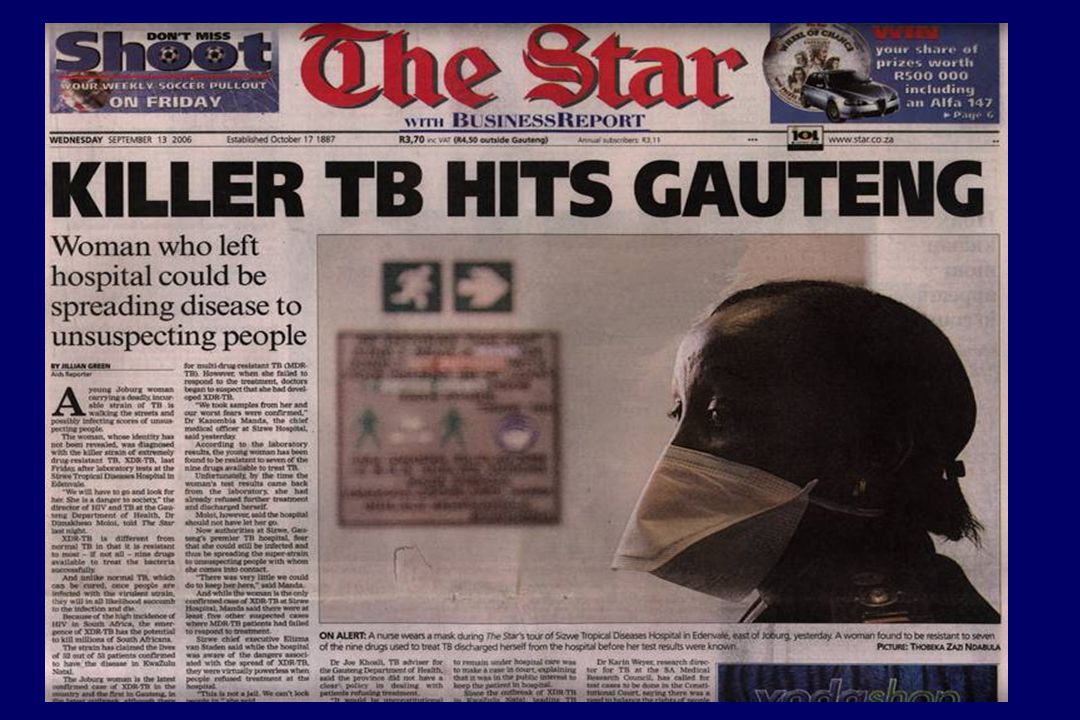
Media Response to XDR TB
in South Africa

32
XDR-TB WHO expresses concern
WHO background briefing note issued prior to XDR-TB Expert Consultation meeting in South Africa

33
Coverage from international broadcasters:
XDR-TB Coverage from international broadcasters: 'Virtually untreatable' TB found A "virtually untreatable" form of TB has emerged, according to the World Health Organization (WHO). Extreme drug resistant TB (XDR TB) has been seen worldwide, including in the US, Eastern Europe and Africa, although Western Europe has had no cases. Dr Paul Nunn, from the WHO, said a failure to correctly implement treatment strategies was to blame.
. Extreme drug resistant TB (XDR TB) has been seen worldwide, including in the US, Eastern Europe and Africa, although Western Europe has had no cases. Dr Paul Nunn, from the WHO, said a failure to correctly implement treatment strategies was to blame.")
34
Coverage in major weekly journals
XDR-TB Coverage in major weekly journals Newsweek Sept. 13, 2006 – WHO recently issued a warning that deadly new strains of tuberculosis appear to be spreading around the globe… HIV sufferers are particularly vulnerable because of their weakened immune systems. TB, already the world’s fourth most fatal infectious disease, could wreak havoc with AIDS treatment programs The South African Medical Research Council, WHO, and the US Centers for Disease Control and Prevention plan calls for: rapid surveys to assess the current prevalence of XDR-TB globally; enhanced local laboratory capacity to carry out culture and drug-resistance testing; increased training for public-health staff to identify, investigate, and treat XDR-TB outbreaks; implementation of infection control precautions; increased research support for drugs to treat XDR-TB and for development of rapid diagnostic tests for TB; and access to antiretroviral drugs. The Lancet Failure to act now to contain the threat posed by XDR-TB will have devastating consequences for patients with TB, particularly those co-infected with HIV/AIDS. Prompt enacting of the seven-point plan agreed in Johannesburg is crucial for the future of TB and HIV/AIDS control efforts and for the prevention of XDR-TB related deaths. The Lancet 2006; 368:964 DOI: /S (06) XDR-TB—a global threat See Comment See Articles Following an emergency consultation in Johannesburg on Sept 7 and 8, global health agencies have developed a seven-point plan to combat extensively (or extremely) drug-resistant tuberculosis (XDR-TB). Representatives from several southern African countries have agreed to implement the plan within 3 months. Multidrug-resistant TB (MDR-TB), defined as resistance to at least isoniazid and rifampicin, requires the use of second-line drugs that are less effective, more expensive, and more toxic than first-line regimens based on isoniazid and rifampicin. Recognised earlier this year, XDR-TB is MDR-TB that is also resistant to three or more of the six classes of second-line drugs. Of TB isolates taken between 2000 and 2004, 20% were MDR and 2% were XDR. XDR-TB has now been identified in all regions of the world but is most prevalent in Asia and in eastern Europe. Since WHO guidelines recommend the use of at least four drugs for those with MDR-TB, XDR-TB is untreatable to international standards. Data presented at the XVI International AIDS Conference in Toronto last month indicate the high mortality associated with XDR-TB—of 536 patients with TB in a rural district in KwaZulu Natal, South Africa, 221 had MDR-TB, and 53 of these were defined as XDR-TB, most of whom were coinfected with HIV; 52 of these 53 patients have died.
 XDR-TB—a global threat. See Comment See Articles. Following an emergency consultation in Johannesburg on Sept 7 and 8, global health agencies have developed a seven-point plan to combat extensively (or extremely) drug-resistant tuberculosis (XDR-TB). Representatives from several southern African countries have agreed to implement the plan within 3 months. Multidrug-resistant TB (MDR-TB), defined as resistance to at least isoniazid and rifampicin, requires the use of second-line drugs that are less effective, more expensive, and more toxic than first-line regimens based on isoniazid and rifampicin. Recognised earlier this year, XDR-TB is MDR-TB that is also resistant to three or more of the six classes of second-line drugs. Of TB isolates taken between 2000 and 2004, 20% were MDR and 2% were XDR. XDR-TB has now been identified in all regions of the world but is most prevalent in Asia and in eastern Europe. Since WHO guidelines recommend the use of at least four drugs for those with MDR-TB, XDR-TB is untreatable to international standards. Data presented at the XVI International AIDS Conference in Toronto last month indicate the high mortality associated with XDR-TB—of 536 patients with TB in a rural district in KwaZulu Natal, South Africa, 221 had MDR-TB, and 53 of these were defined as XDR-TB, most of whom were coinfected with HIV; 52 of these 53 patients have died.")
35
Coverage in major weekly journals
XDR-TB Coverage in major weekly journals The South African Medical Research Council, WHO, and the US Centers for Disease Control and Prevention plan calls for: rapid surveys to assess the current prevalence of XDR-TB globally; enhanced local laboratory capacity to carry out culture and drug-resistance testing; increased training for public-health staff to identify, investigate, and treat XDR-TB outbreaks; implementation of infection control precautions; increased research support for drugs to treat XDR-TB and for development of rapid diagnostic tests for TB; and access to antiretroviral drugs. The Lancet Failure to act now to contain the threat posed by XDR-TB will have devastating consequences for patients with TB, particularly those co-infected with HIV/AIDS. Prompt enacting of the seven-point plan agreed in Johannesburg is crucial for the future of TB and HIV/AIDS control efforts and for the prevention of XDR-TB related deaths. The Lancet 2006; 368:964 DOI: /S (06) XDR-TB—a global threat See Comment See Articles Following an emergency consultation in Johannesburg on Sept 7 and 8, global health agencies have developed a seven-point plan to combat extensively (or extremely) drug-resistant tuberculosis (XDR-TB). Representatives from several southern African countries have agreed to implement the plan within 3 months. Multidrug-resistant TB (MDR-TB), defined as resistance to at least isoniazid and rifampicin, requires the use of second-line drugs that are less effective, more expensive, and more toxic than first-line regimens based on isoniazid and rifampicin. Recognised earlier this year, XDR-TB is MDR-TB that is also resistant to three or more of the six classes of second-line drugs. Of TB isolates taken between 2000 and 2004, 20% were MDR and 2% were XDR. XDR-TB has now been identified in all regions of the world but is most prevalent in Asia and in eastern Europe. Since WHO guidelines recommend the use of at least four drugs for those with MDR-TB, XDR-TB is untreatable to international standards. Data presented at the XVI International AIDS Conference in Toronto last month indicate the high mortality associated with XDR-TB—of 536 patients with TB in a rural district in KwaZulu Natal, South Africa, 221 had MDR-TB, and 53 of these were defined as XDR-TB, most of whom were coinfected with HIV; 52 of these 53 patients have died.
 XDR-TB—a global threat. See Comment See Articles. Following an emergency consultation in Johannesburg on Sept 7 and 8, global health agencies have developed a seven-point plan to combat extensively (or extremely) drug-resistant tuberculosis (XDR-TB). Representatives from several southern African countries have agreed to implement the plan within 3 months. Multidrug-resistant TB (MDR-TB), defined as resistance to at least isoniazid and rifampicin, requires the use of second-line drugs that are less effective, more expensive, and more toxic than first-line regimens based on isoniazid and rifampicin. Recognised earlier this year, XDR-TB is MDR-TB that is also resistant to three or more of the six classes of second-line drugs. Of TB isolates taken between 2000 and 2004, 20% were MDR and 2% were XDR. XDR-TB has now been identified in all regions of the world but is most prevalent in Asia and in eastern Europe. Since WHO guidelines recommend the use of at least four drugs for those with MDR-TB, XDR-TB is untreatable to international standards. Data presented at the XVI International AIDS Conference in Toronto last month indicate the high mortality associated with XDR-TB—of 536 patients with TB in a rural district in KwaZulu Natal, South Africa, 221 had MDR-TB, and 53 of these were defined as XDR-TB, most of whom were coinfected with HIV; 52 of these 53 patients have died.")
36
African press coverage:
XDR-TB African press coverage: New TB strain in SA: 'No time to wait' 07 September 2006 The extreme drug-resistant tuberculosis (XDR-TB) in KwaZulu-Natal must be dealt with urgently, international health experts said in Johannesburg on Thursday. "There is no time to wait before we embark on decisive action," said the World Health Organisation's Dr Ernesto Jaramillo, explaining that an epidemic could have a deadly impact.
 in KwaZulu-Natal must be dealt with urgently, international health experts said in Johannesburg on Thursday. There is no time to wait before we embark on decisive action, said the World Health Organisation s Dr Ernesto Jaramillo, explaining that an epidemic could have a deadly impact.")
37
XDR-TB International press coverage:

38
International headlines:
XDR-TB International headlines: Deadly TB strain spreading across globe Africa: "Extreme" TB Bug Prompts Calls for Rapid Action Experts call for urgent steps to battle virulent TB strain South Africa: Action plan developed to combat drug resistant TB WHO urges South Africa to curb TB killer super-bug Global alert over deadly new TB strains TB strain with extreme resistance to drugs creates nightmare scenario TB experts will grapple with deadly new strains: WHO

39
Editorial in New York Times & Int. Herald Tribune
XDR-TB Editorial in New York Times & Int. Herald Tribune EXTREME TUBERCULOSIS SEPTEMBER 14, 2006 TB is outrunning us. In the last few months, 53 patients in the South African province of KwaZulu-Natal were found to have a form of the disease resistant to enough existing drugs that it is virtually incurable. All but one of those patients have died… Stinginess created this problem. Generosity is needed to fix it.

40
Stop TB XDR Response 1. Coordination – Develop an appropriate, coordinated global response to XDR TB 2. Resource mobilization – Raise sufficient funds to ensure no delays in the global response to XDR TB 3. Case definitions – Ensure consistency in surveillance and case management 4. Monitoring and evaluation – Determine geographical and temporal spread of XDR TB

41
Stop TB XDR Response (2) 5. Communications – Provide a proactive flow of information to all stakeholders, including member states and the global media 6. Case management – Define the optimal way of rapidly identifying suspect XDR cases and ensuring appropriate treatment; determine appropriate infection control measures in health facilities 7. Country support – Ensure a timely and sufficient response to requests from countries for assistance

42
This time, I bet you that if the press is prompted and well prepared, journalists will come like flies around a cake and other objects... Mario Raviglione

Similar presentations


>")










 in India Dr Jitendra.>")
 update ACSM workshop, Amman, Jordan April 13-17, 2008 Dr. Sevil Huseynova.>")





