Download presentation
Presentation is loading. Please wait.

1
Sleep Apnea Dr. Vishal Sharma

2
History Lugaresis (1970): described OSAS Stanford University (1972): Polysomnography Sleep Latency Test devised in 1976 Before 1980’s tracheostomy main treatment Ikematsu performed first UPPP in 1952 Fujita popularized UPPP Kamami developed LAUP in late 1980s
: described OSAS Stanford University (1972): Polysomnography Sleep Latency Test devised in 1976 Before 1980’s tracheostomy main treatment Ikematsu performed first UPPP in 1952 Fujita popularized UPPP Kamami developed LAUP in late 1980s")
3
Definitions

4
Sleep related breathing disorders Synonym: sleep disordered breathing Consists of: A. Snoring B. Obstructive sleep apnea C. Obstructive sleep hypopnea D. Upper airways resistance syndrome

5
Arousal: Abrupt change from deep stage to lighter stage of NREM sleep, or from REM sleep to awakening Arousal index: Number of arousals per hour of sleep Apnea: Cessation of breathing for > 10 seconds Apnea Index: Number of apneas per hour of sleep Hypopnea: Decreased airflow (>50%) with oxygen desaturation (> 4% ) for > 10 seconds Snoring: breathing noise due to partial upper airway obstruction
 with oxygen desaturation (> 4% ) for > 10 seconds Snoring: breathing noise due to partial upper airway obstruction")
6
Obstructive sleep apnea: Cessation of airflow for > 10 seconds even with continued respiratory effort Obstructive sleep hypopnea: Decreased airflow (>50%) with oxygen desaturation (> 4% ) for > 10 seconds even with continued respiratory effort Upper airway resistance syndrome (respiratory effort related arousal): partial airway obstruction with no apnea or hypnea, but arousal index > 15
 with oxygen desaturation (> 4% ) for > 10 seconds even with continued respiratory effort Upper airway resistance syndrome (respiratory effort related arousal): partial airway obstruction with no apnea or hypnea, but arousal index > 15")
7
Respiratory Distress Index: Number of apneas + hypopneas + respiratory effort related arousals per hour Obstructive sleep apnea syndrome: 30 or more episodes of obstructive sleep apnea during a 7- hour period of sleep or apnea index > 5 or respiratory distress index > 15

8
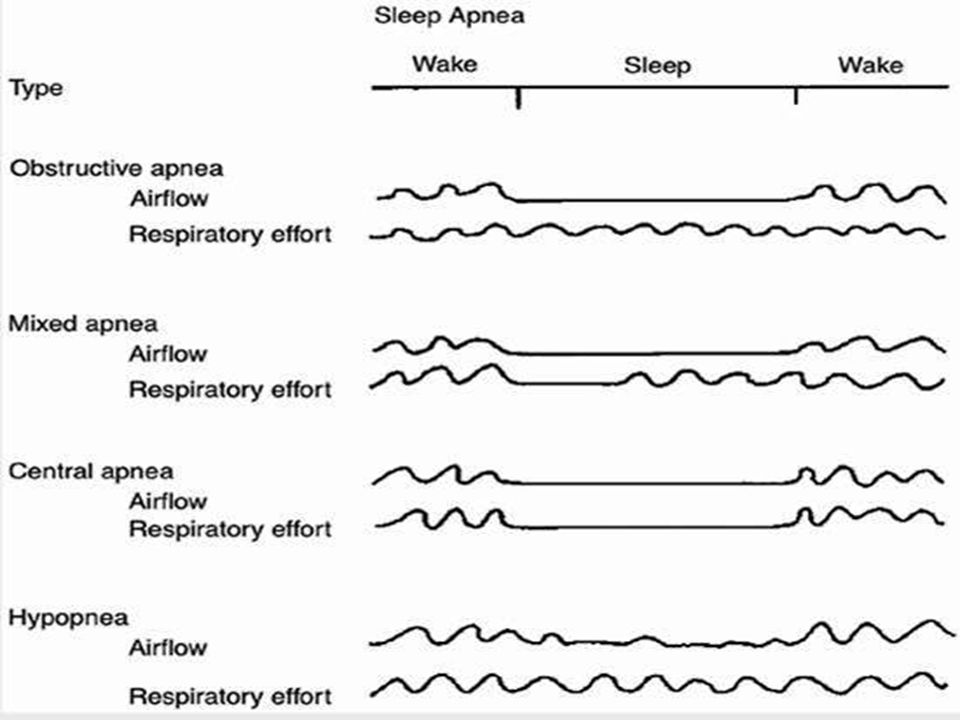
Types of sleep apnea 1. Obstructive: Normal respiratory chest wall movement 2. Central: No respiratory chest wall movement 3. Mixed: Partial respiratory chest wall movement

10
American Sleep association grading: 1. Mild ------------5 - 20 apneas per hour 2. Moderate ----- 20 - 40 apneas per hour 3. Severe --------more than 40 apneas per hour Grades of sleep apnea

11
Etiology of central sleep apnea

12
Cheyne-Stokes breathing-central sleep apnea due to renal failure, heart failure, stroke Diabetes mellitus, Hypothyroidism, Acromegaly, Parkinson disease, Myasthenia gravis, Idiopathic cardiomyopathy, Muscular dystrophy Medullary tumor or infarction Arnold-Chiari malformation Cervical cordotomy High-altitude periodic breathing (at > 5000m) Use of opiates & other CNS depressants
 Use of opiates & other CNS depressants")
13
Cheyne-Stokes crescendo- decrescendo breathing

14
Etiology of obstructive sleep apnea

15
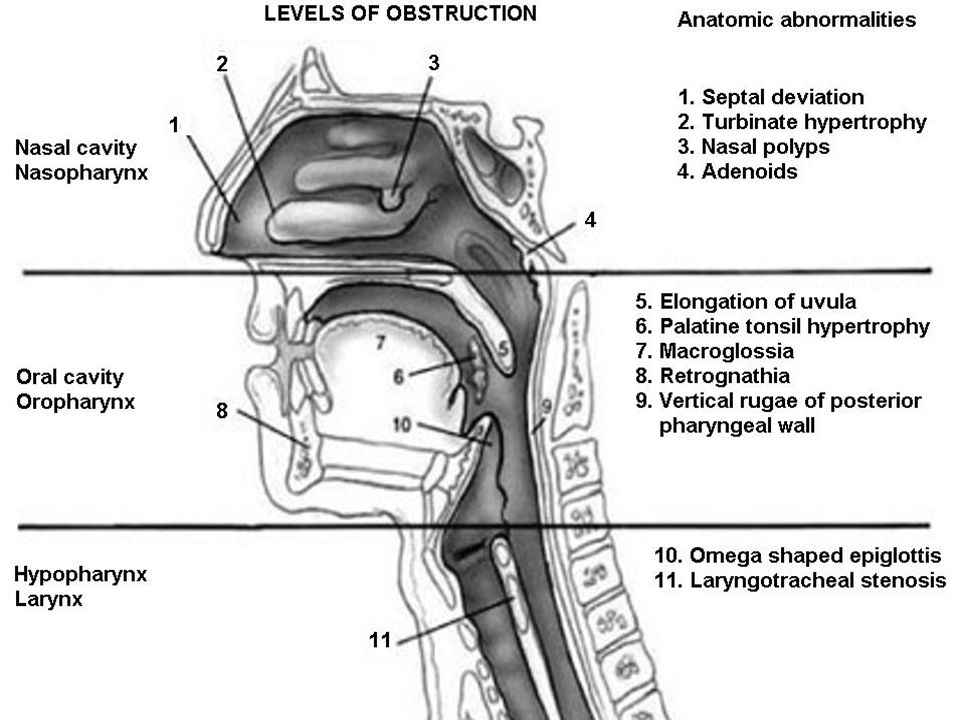
Nose Nasal polyps DNS ed Turbinate Nasal packing Larynx Tumors Edema Stenosis Pharynx Nasopharyngeal tumor Adenoids ed palatal / lingual tonsil Enlarged lingual tonsils Retropharyngeal mass Large tongue Micrognathia / Retrognathia Obesity

19
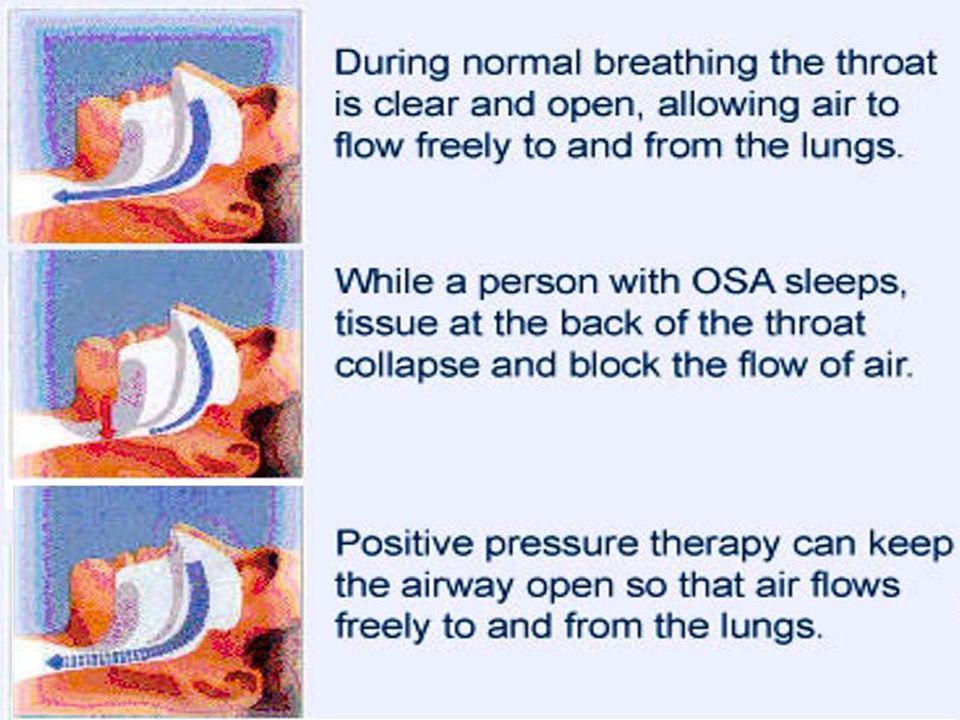
Patho-physiology

20
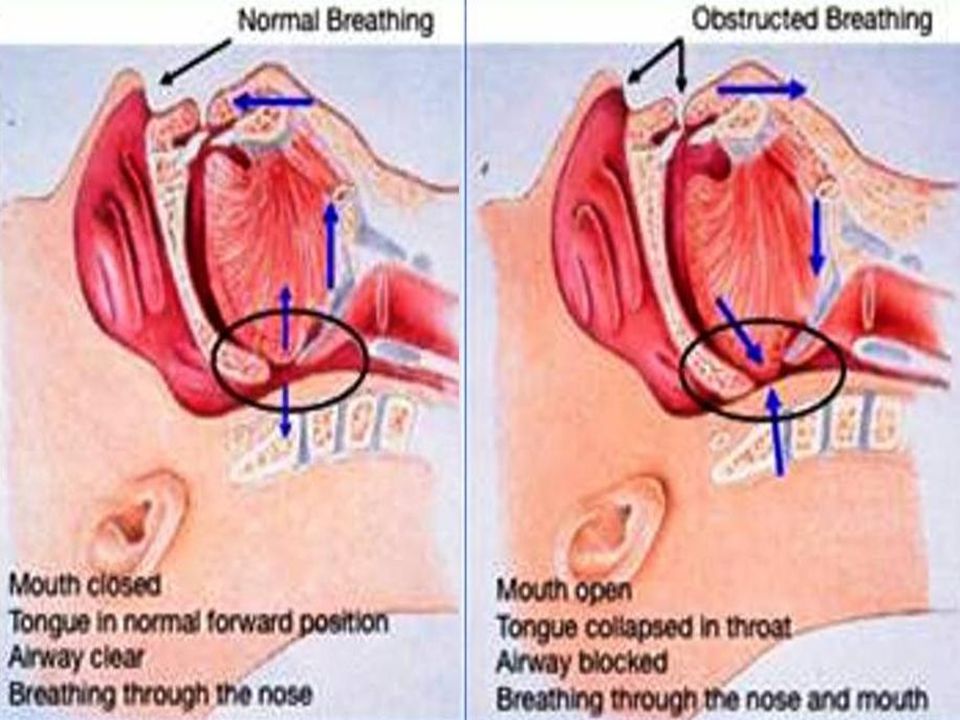
Increased compliance of pharyngeal tissues + Neuromuscular in-coordination & ed muscle tone + Anatomical abnormalities Upper airway collapse airway obstruction Hypoxia + negative intra-thoracic pressure Arousal Increased tone of upper airway muscles + upper airway obstruction clears Patient goes to sleep Upper airway collapses again causing arousal

21
Sequelae of sleep apnea

22
Complications of sleep apnea Systemic hypertension Coronary artery disease Pulmonary hypertension Right heart failure Cardiac arrhythmias Cerebro-vascular accident Polycythemia Sleepiness accidents Depression Impotence Vagal bradycardia Sudden nocturnal death

23
Clinical Features

24
Snoring or sleep apnea?

25
Symptoms of sleep apnea Day- time Excessive sleepiness Morning headache Intellectual deterioration Personality change Depression Xerostomia Abnormal movements Night- time Snoring Observed choking Arousal from sleep Repeated waking Nocturnal sweating Nocturnal enuresis Impotence

26
Typical OSAS patient Synonym: Pickwickian syndrome Middle age or elderly male with hyper somnolence Obese with body mass index > 30 Short neck with its circumference > 17 inches Hypertension & right heart failure Large bulky tongue, hypertrophied tonsils, bulky soft palate, prominent posterior pharyngeal wall rugae

27
Mr. Pickwick & fat boy Joe

28
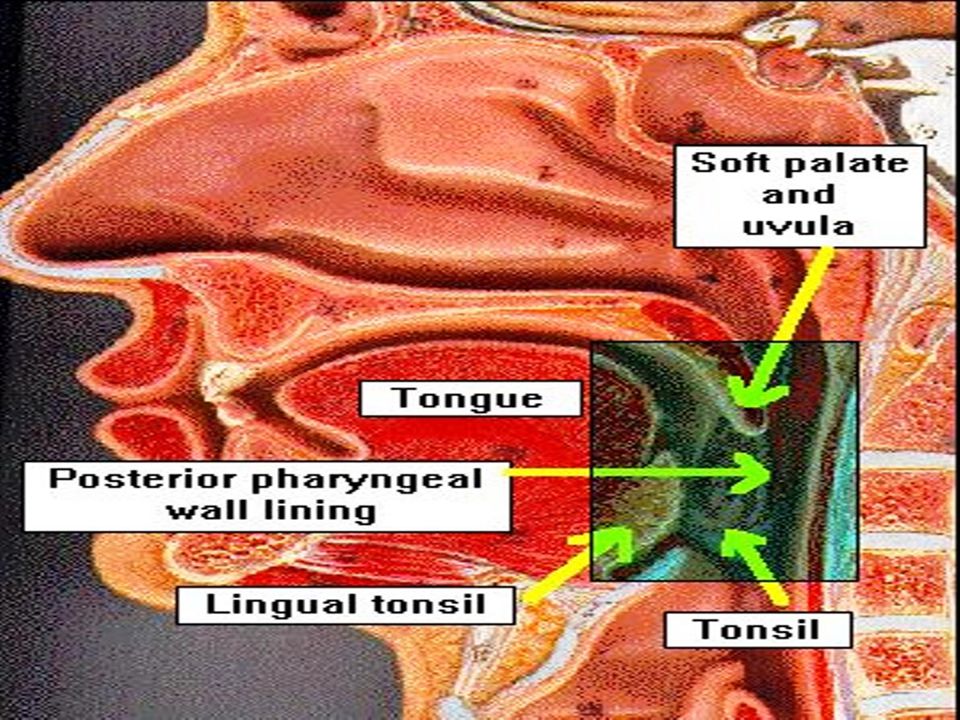
Throat in OSAS

29
History from sleep partner Bed timings Body position Snoring Apnea (choking) Arousal from sleep Alcohol consumption Sedative use
 Arousal from sleep Alcohol consumption Sedative use")
30
Epworth daytime sleepiness scale Score > 16 = moderate to severe sleep apnea

31
General appearance, weight, body mass index Blood pressure, cardiovascular examination Cranio-facial: retrognathia, hypoplastic maxilla Nasal: airway patency, DNS, turbinate hypertrophy Tongue: macroglossia, lingual tonsil Nasopharynx: adenoids, polyp, cyst, tumor Physical examination

32
Oropharynx: Soft palate, palatine tonsil, base of tongue, posterior pharyngeal wall Hypopharynx: tumor Larynx: cyst, tumor, vocal cord mobility Neck: short wide neck (circumference > 17 inches) Thyroid enlargement, features of hypothyroidism
 Thyroid enlargement, features of hypothyroidism")
33
Investigations

34
General Investigations Complete blood count: anemia, polycythemia Chest x-ray: cardiomegaly, pulmonary disorder Lung function: portable spirometry flow volume loop saw-tooth pattern Thyroid function tests: hypothyroidism Electro-cardiography: cardiac arrhythmias Arterial blood gas analysis

35
Portable spirometer

36
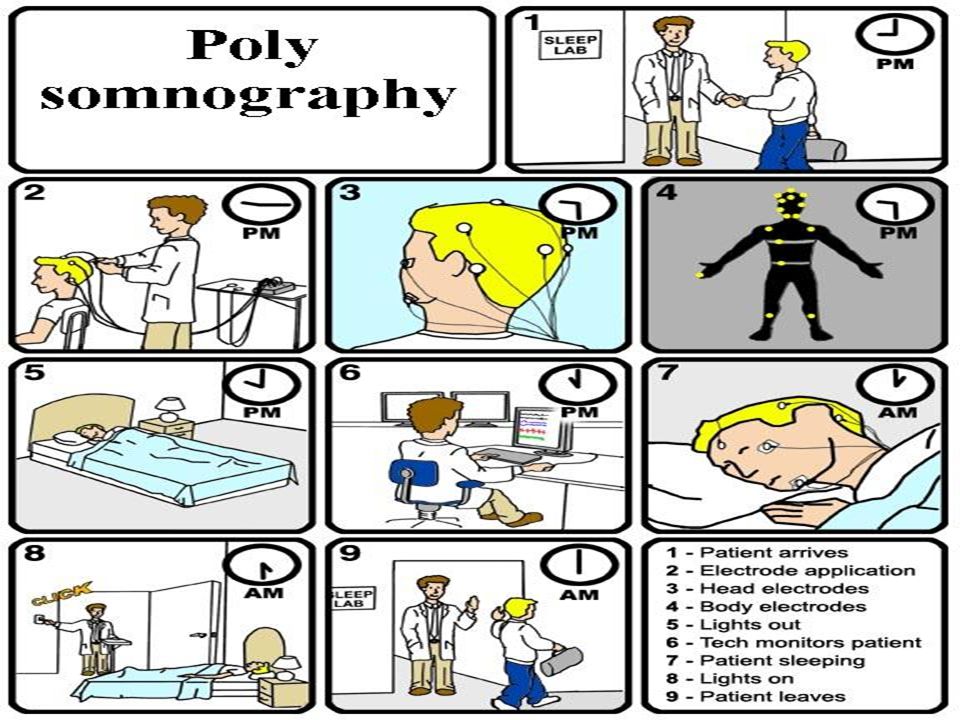
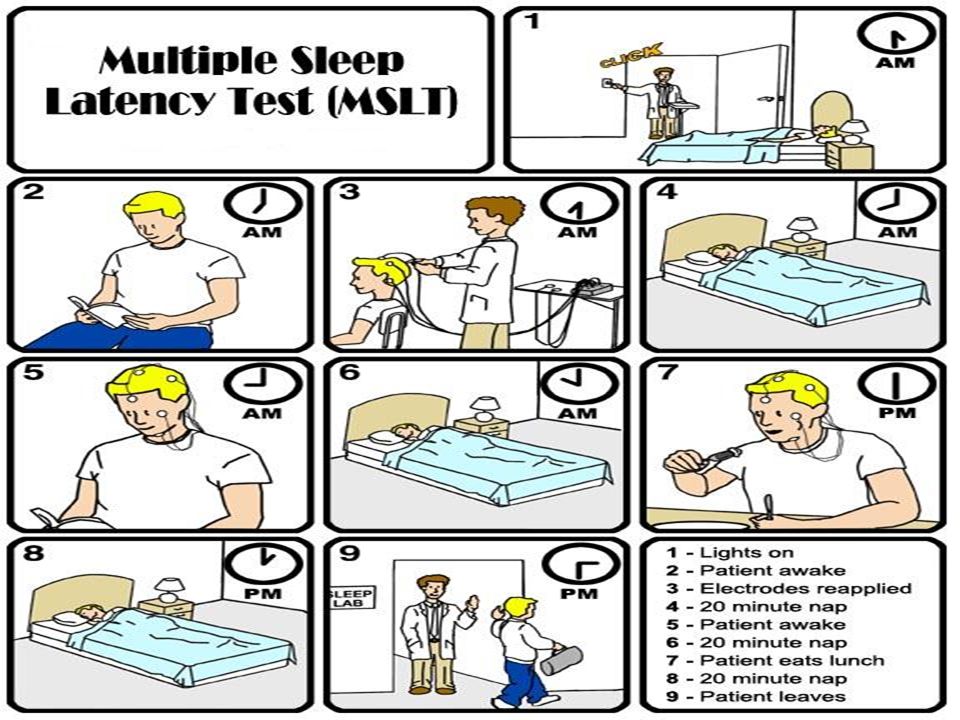
Investigations for confirmation of sleep apnea Polysomnography Portable sleep monitoring Overnight pulse oximetry recording Multiple sleep latency test

37
1. Electro-encephalogram (EEG) 2. Electro-myogram (EMG): submental, anterior tibialis 3. Electro-oculogram (EOG) / Electro-nystagmogram 4. Electro-cardiogram (ECG) 5. Oxygen saturation 6. Nasal & oral airflow 7. Chest + abdominal movement detector 8. Sleeping position detector 9. Tracheal microphone 10. Esophageal manometer Polysomnography parameters
 / Electro-nystagmogram 4. Electro-cardiogram (ECG) 5. Oxygen saturation 6. Nasal & oral airflow 7. Chest + abdominal movement detector 8. Sleeping position detector 9. Tracheal microphone 10. Esophageal manometer Polysomnography parameters.")
39
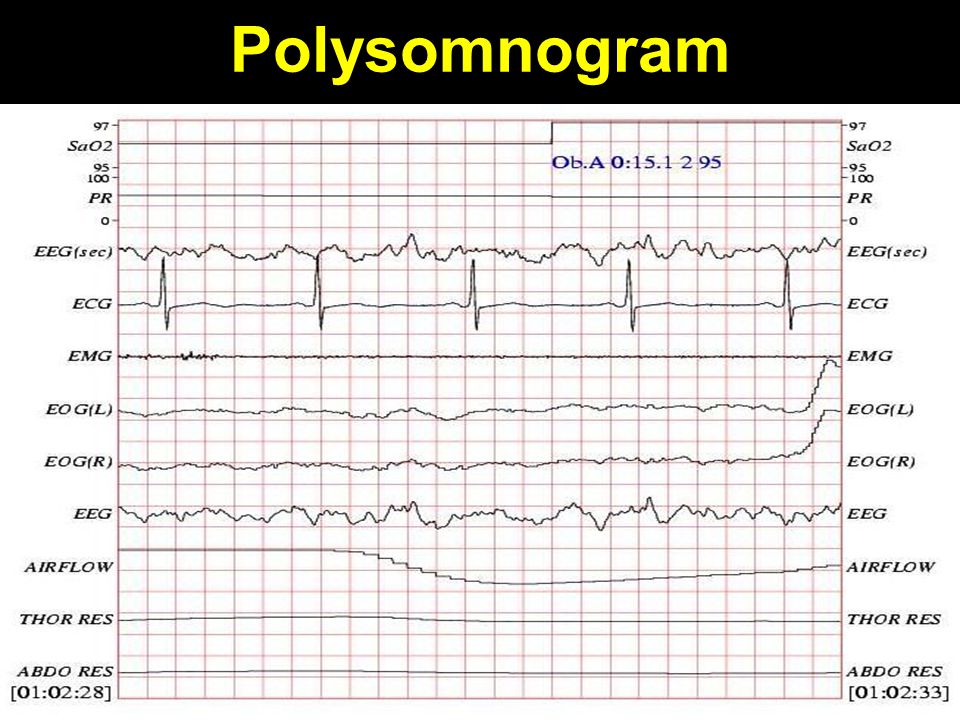
Polysomnogram

42
Polysomnogram in arousal

43
Portable polysomnogram

45
Awake patientSleeping patient Muller maneuver Flexible nasendoscopy Lateral cephalometry Somno-fluoroscopy C.T. scan of neck Cine C.T. scan Pharyngeal manometry Investigations to assess site of airway obstruction

46
Flexible endoscopy

47
Muller’s maneuver After a forced expiration, pt attempts inspiration with closed mouth & nose, whereby negative pressure leads to collapse of airway Previously introduced flexible endoscope (via nasal cavity) identifies weakened sections of airway at levels of soft palate & tongue base, during this maneuver
 identifies weakened sections of airway at levels of soft palate & tongue base, during this maneuver")
49
Muller’s maneuver in snoring shows no airway narrowing Before MullerAfter Muller

50
Muller’s maneuver in apnea shows airway narrowing Before MullerAfter Muller

51
Degree of airway obstruction 0 = no collapse 1+ = minimal collapse 2+ = collapse es cross-sectional area by 50% 3+ = collapse es cross-sectional area by 75% 4+ = collapse obliterates airway 3+ or 4+ score at soft palate level with 0 score at tongue base level is ideal for UPPP Score of > 2+ at tongue base level is not suitable for Uvulo-palato-pharyngo-plasty (UPPP)
")
52
Muller’s obstruction types Oropharynx obstruction (soft palate) Hypopharynx obstruction (tongue base) I3+, 4+0, 1+ II a3+, 4+1+, 2+ II b3+, 4+ III0, 1+3+, 4+
 Hypopharynx obstruction (tongue base) I3+, 4+0, 1+ II a3+, 4+1+, 2+ II b3+, 4+ III0, 1+3+, 4+")
53
Lateral cephalometry

55
Measurements in obstructive sleep apnea: Posterior airway space (PAS) or narrowest width of hypopharynx is < 5 mm Distance b/w mandibular plane to hyoid bone (MP-H) is > 24 mm
 or narrowest width of hypopharynx is < 5 mm Distance b/w mandibular plane to hyoid bone (MP-H) is > 24 mm")
56
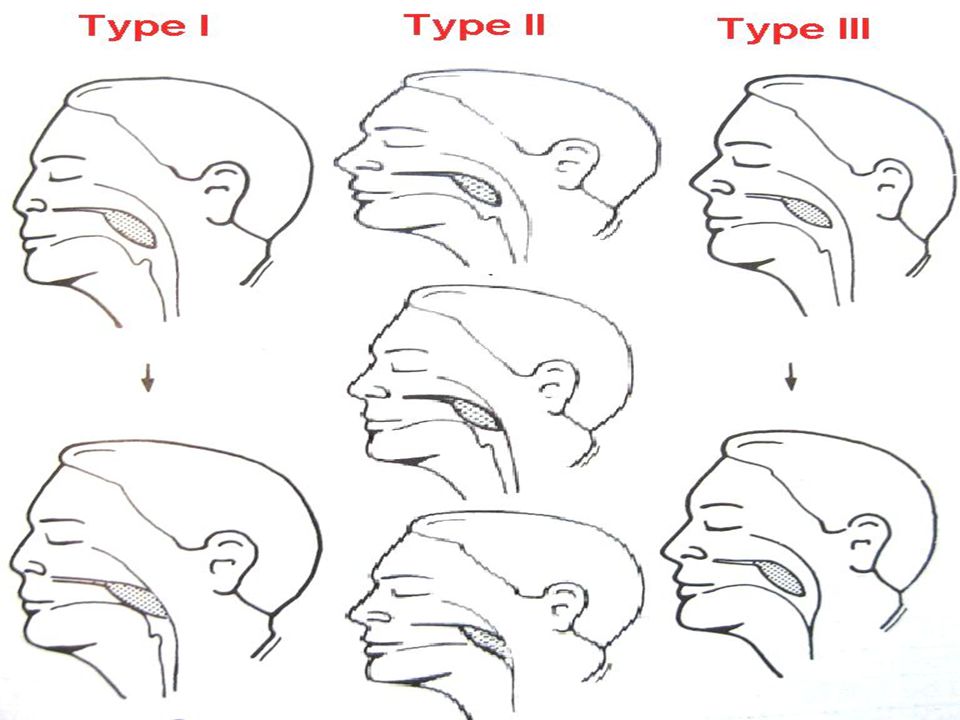
Somno-fluoroscopy Sleeping pt observed with polysomnography & during apneic episode visualized with fluoroscopy for upper airway obstruction Type I = obstruction at soft palate level only Type II = obstruction at soft palate level followed by obstruction at tongue base level Type III = obstruction at tongue base level

58
Cine C.T. scan: Rapid CT scanning of 8 cm of upper airway in 240 msec during apneic episode to study anatomical changes during apneic episode. Research tool. Pharyngeal manometry: Measurement of intra-luminal pressure at level of soft palate, tongue base & hypopharynx

59
D/D of excessive daytime sleepiness (hyper somnolence) Sleep apnea syndrome Narcolepsy Sleep deprivation Hypoglycemia Hypothyroidism Severe anemia Cerebral tumors Depression Sedative drugs Nocturnal myoclonus Idiopathic
 Sleep apnea syndrome Narcolepsy Sleep deprivation Hypoglycemia Hypothyroidism Severe anemia Cerebral tumors Depression Sedative drugs Nocturnal myoclonus Idiopathic")
60
Non-surgical Tx for OSAS Lifestyle modifications Sleep hygiene Medications Nasal valve dilator Positioning device Nasal positive airway pressure device

61
Lifestyle modifications Weight reduction for obese patients Body mass index = weight in kg / (height in metres) 2 Ideal BMI: male < 27.8; female < 27.3 Stop smoking Stop alcohol consumption Avoid sedative drugs
 2 Ideal BMI: male < 27.8; female < 27.3 Stop smoking Stop alcohol consumption Avoid sedative drugs")
62
Sleep hygiene Elevate head-end of bed by 30 0 : decreases pressure of abdominal contents on diaphragm & improves upper airway patency Avoid lying supine: T-shirt with tennis ball at back Avoid sleep deprivation Have regular sleep cycle

63
Medications Amitriptyline & Protriptyline: suppress REM sleep, respiratory stimulant, increase pharyngeal muscle tone Nasal decongestant, antihistamine, steroid spray Fenfluramine to reduce obesity Thyroxin for hypothyroidism

64
Nasal valve dilator Adhesive strip placed over bridge of nose at bedtime

65
Nasal valve dilator Plastic spring ends inserted into nostrils

66
Nasal valve dilator

67
Positioning devices Tongue retaining device Mandibular advancement device Optimized mandible retention Thornton adjustable positioner

68
Effect of positioning devices

69
Mandible advancement device

70
Tongue retaining device Prevents falling back of tongue

71
Optimized mandible retention

72
Thornton adjustable positioner

73
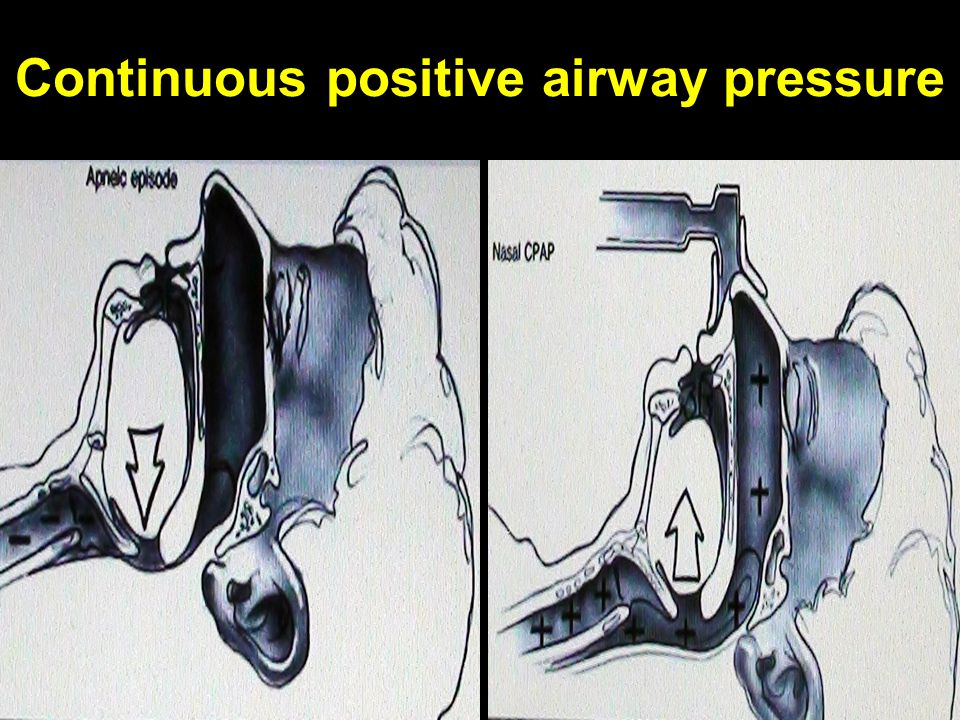
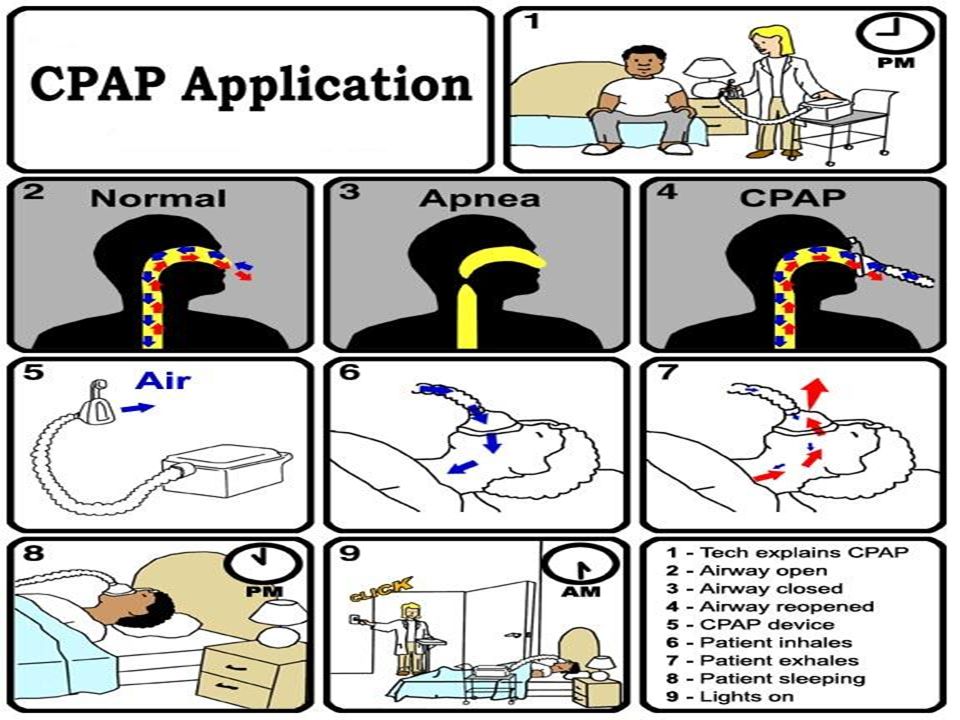
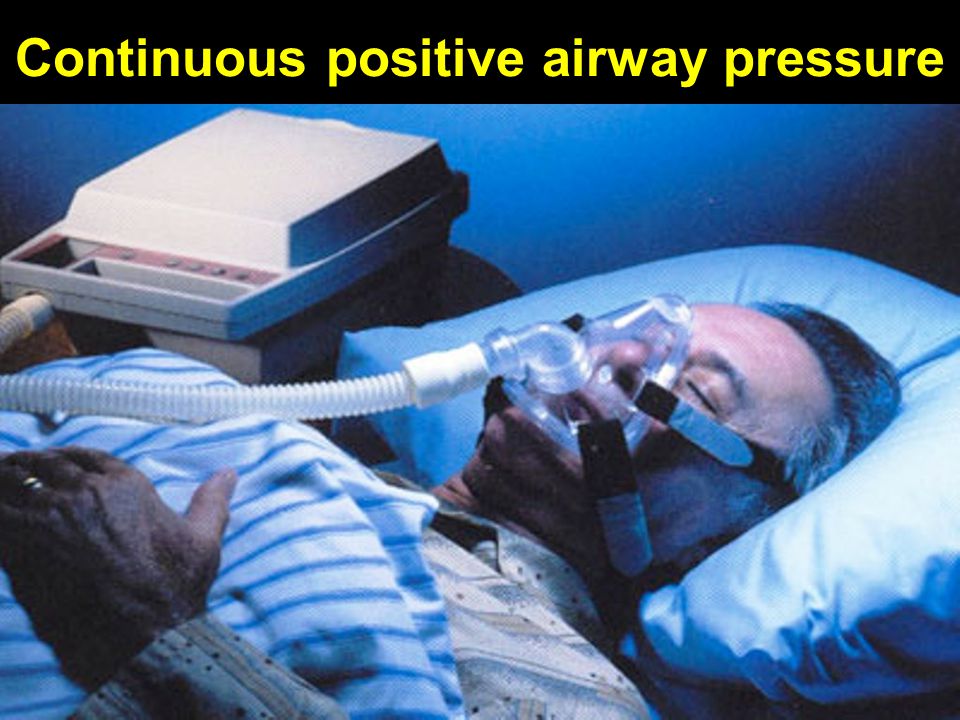
Positive airway pressure devices Gold standard treatment Prevents apneas in 99-100% patients C.P.A.P.: Continuous positive airway pressure Bi.P.A.P.: Bi-level positive airway pressure (less pressure given during expiration) A.P.A.P.: Automatic positive airway pressure (adjusts pressure breath by breath)
 A.P.A.P.: Automatic positive airway pressure (adjusts pressure breath by breath)")
74
Continuous positive airway pressure

79
Polysomnogram before CPAP

80
Polysomnogram after CPAP

81
Surgical Tx of OSAS 1.Nasal surgery 2.Palatal surgery 3.Tongue base surgery 4.Maxillo-facial surgery 5.Tracheostomy: last resort, 100% cure; relieves all levels of airway obstruction

82
Nasal & nasopharyngeal surgery More effective for snoring than sleep apnea 1. Septo-turbinoplasty 2. Radio-frequency turbinate somnoplasty 3. Nasal polypectomy 4. Nasal valve reconstruction 5. Nasal mass excision 6. Adeno-tonsillectomy

83
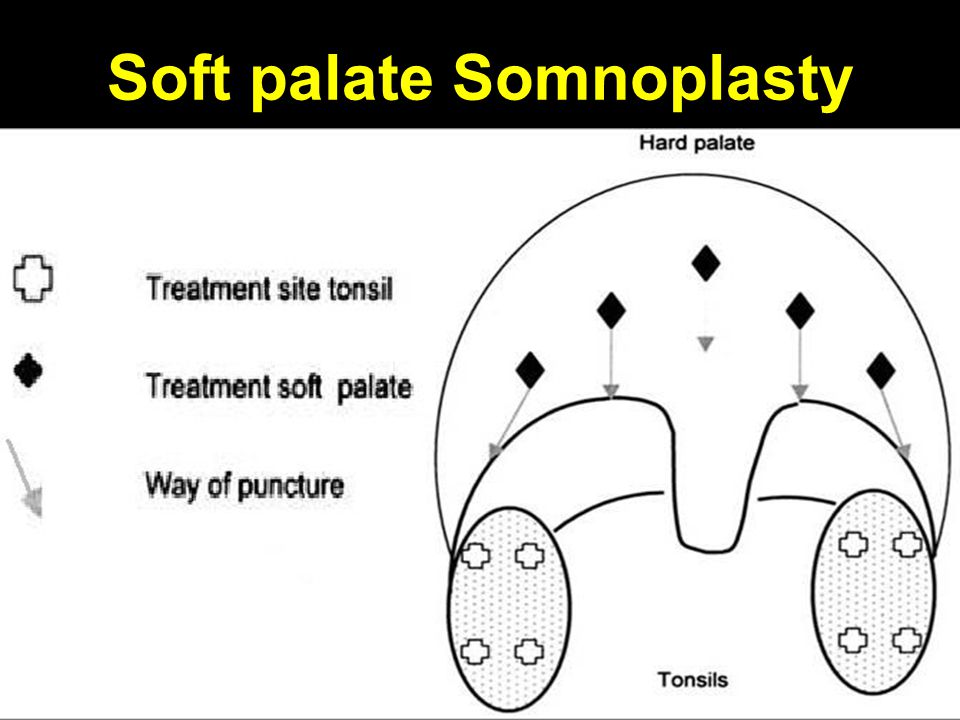
Somnoplasty Small probe delivers radiofrequency energy into tissue bulk, causing coagulative lesions which shrink on healing Body absorbs these lesions over 4-8 weeks leading to tissue volume reduction Used for enlarged base of tongue / soft palate / turbinates causing snoring / sleep apnea

84
Turbinate Somnoplasty

85
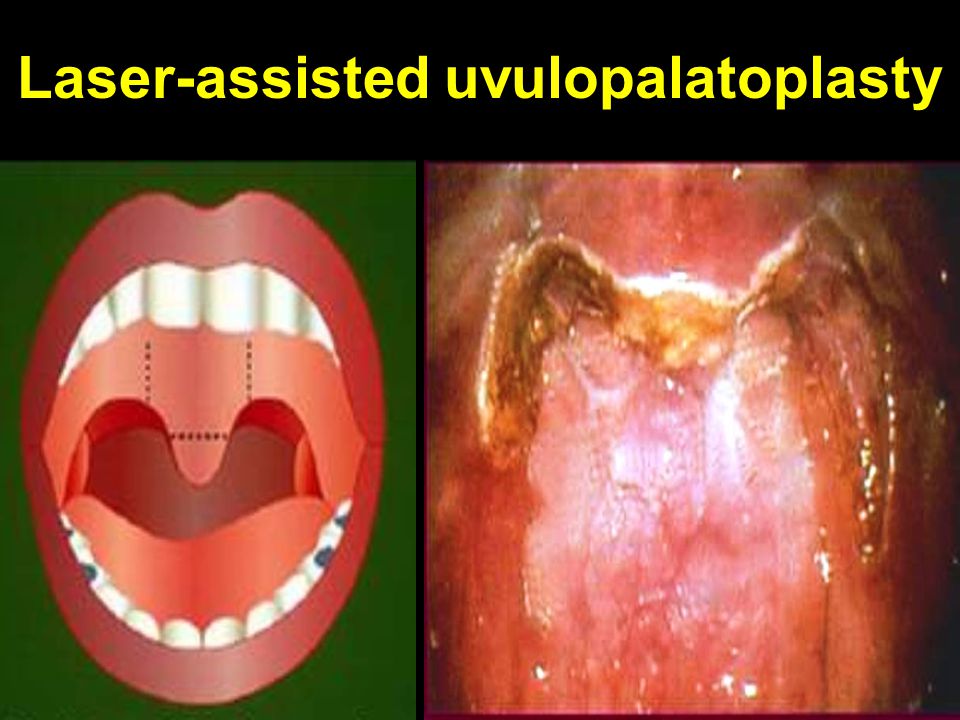
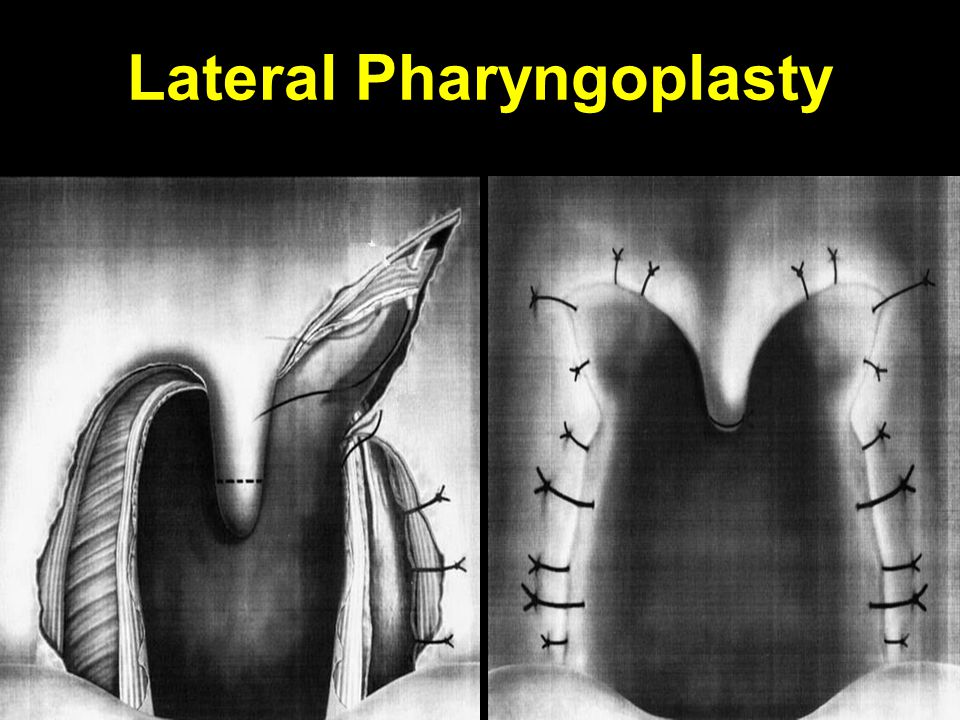
Palatal Surgery Relieve palato-pharyngeal level obstruction 1. Uvulo-palato-pharyngo-plasty (UPPP) 2. Laser-assisted Uvulo Palato-plasty (LAUP) 3. Radio-frequency uvulo-palato-plasty (RFUP) 4. Uvulo-palatal flap 5. Lateral pharyngoplasty 6. Palatal stiffening operations
 2. Laser-assisted Uvulo Palato-plasty (LAUP) 3. Radio-frequency uvulo-palato-plasty (RFUP) 4. Uvulo-palatal flap 5. Lateral pharyngoplasty 6. Palatal stiffening operations.")
86
Uvulo Palato Pharyngo Plasty

87
Remove palatine tonsils Trim tonsillar pillars (optional) Remove uvula & variable amount of soft palate Suture posterior tonsillar pillar to anterior tonsillar pillar Suture posterior soft palate mucosa to anterior soft palate mucosa
 Remove uvula & variable amount of soft palate Suture posterior tonsillar pillar to anterior tonsillar pillar Suture posterior soft palate mucosa to anterior soft palate mucosa")
88
Uvulo-palato-pharyngo-plasty

90
Post excision & suturing

91
Structures removed in UPPP

92
Uvulo-palato-pharyngo-plasty

93
Post-UPPP healing

94
Laser-assisted uvulopalatoplasty

96
Soft palate Somnoplasty

98
Uvulo-palatal flap

99
Lateral Pharyngoplasty

101
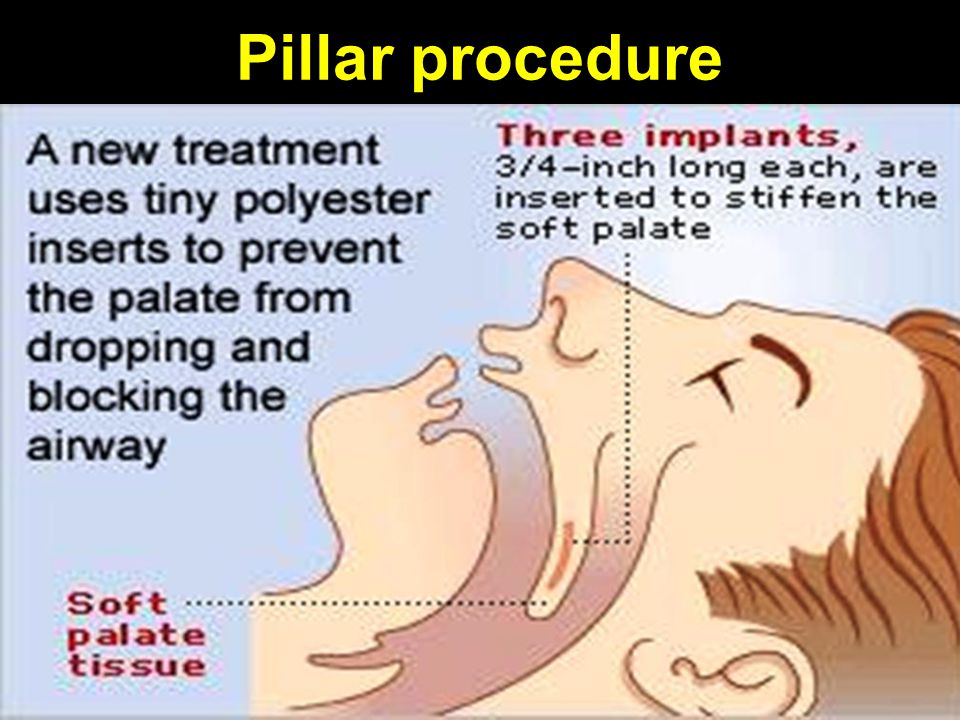
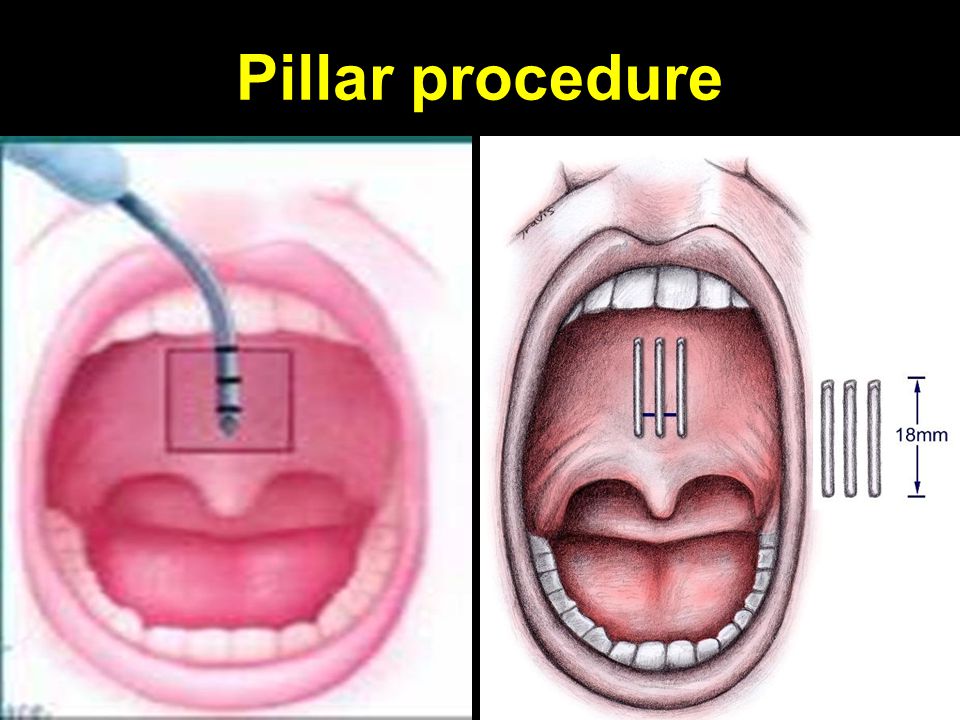
Palatal stiffening surgery Done primarily for snoring Injection of sclerosing agents into soft palate Laser-assisted palatal stiffening operation: longitudinal strip of palatal mucosa removed lesion heals by scarring Cautery-assisted palatal stiffening operation Pillar procedure

104
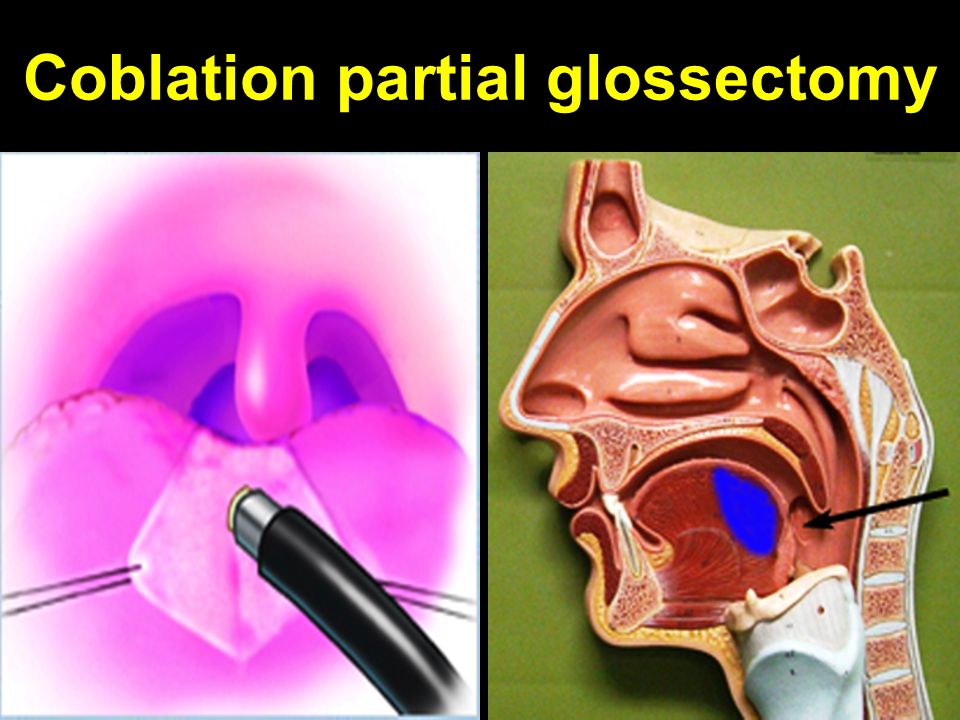
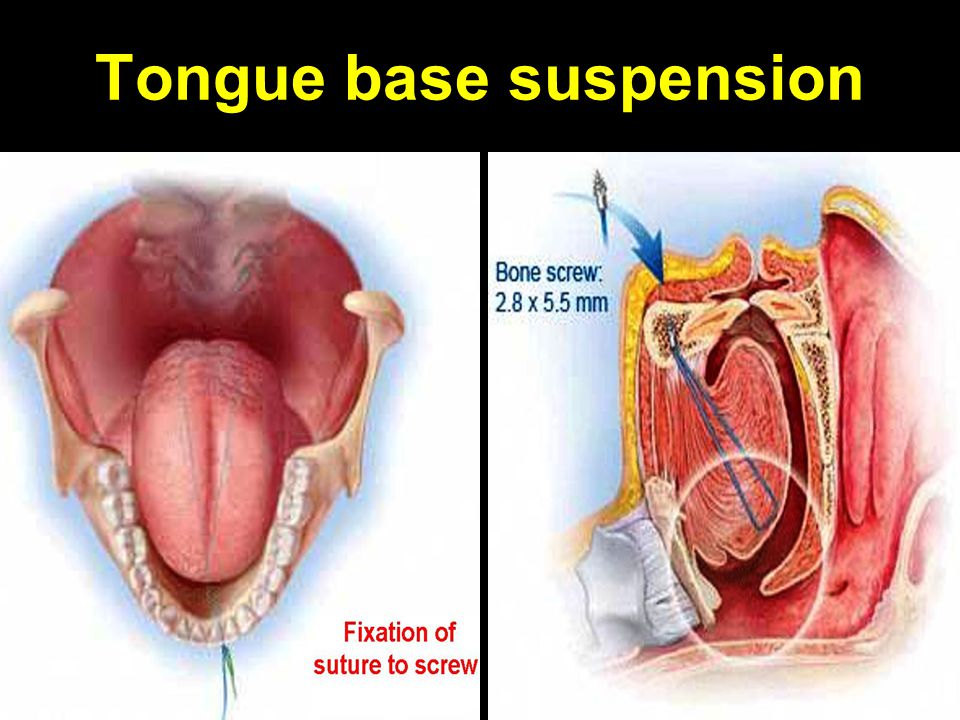
Tongue base surgery 1. Radiofrequency tongue base somnoplasty 2. Submucosal Minimally Invasive Lingual Excision or Coblation tongue base ablation 3. Laser–assisted tongue base ablation 4. Lingual tonsillectomy 5. Linguloplasty 6. Tongue base suspension

105
Tongue base Somnoplasty

106
Coblation partial glossectomy

108
Coblation lingual tonsillectomy

109
Linguloplasty

110
Tongue base suspension

113
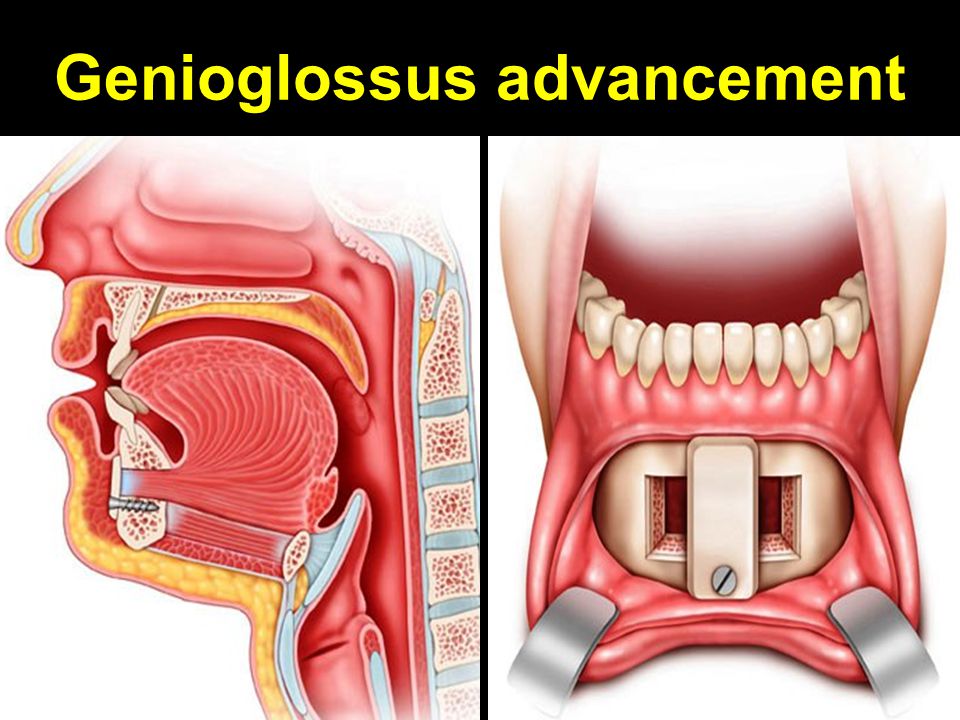
Maxillofacial Procedures Relieve tongue base level obstruction 1. Maxillo-mandibular osteotomy & advancement 2. Genioglossus advancement 3. Maxillary expansion 4. Mandibular expansion 5. Infra-hyoid myotomy & superior suspension 6. Supra-hyoid myotomy & anterior advancement

114
Mandibular advancement

115
Maxillo-mandibular advancement

116
Genioglossus advancement

118
Maxillary expansion

119
Mandibular expansion

120
Infra-hyoid myotomy + superior suspension to mandible

121
Supra-hyoid myotomy & anterior advancement to thyroid cartilage

122
Tracheostomy

123
Treatment of central sleep apnea Acetazolamide: induces metabolic acidosis & increases baseline ventilation Theophylline: respiratory stimulant Zolpidem: sedative hypnotic, consolidates sleep Continuous positive airway pressure Adaptive servo ventilation: provides a fixed CPAP of 5 cm water. Better than nasal CPAP.

124
Thank You

Similar presentations








>")

 is a sleeping disorder that causes a person to stop breathing for a span of seconds In OSA, the airway.>")

 286-7455 Fax: (703) 286-7462.>")

 By Hatem Ezz eldin Hassen MD Consultant of Phoniatrics KFHJ.>")









