Download presentation
Presentation is loading. Please wait.

1
Now would be the time to make sure you have coffee in hand.

2
Understand hepatic anatomy and physiology Understand liver’s role in metabolism Review liver functions tests Describe the effects of anesthesia on the liver

3
Dr. Lindsay Higgins will be presenting Chapter 34: Anesthesia for Patients with Liver Disease Hopefully, she will provide cookies.

5
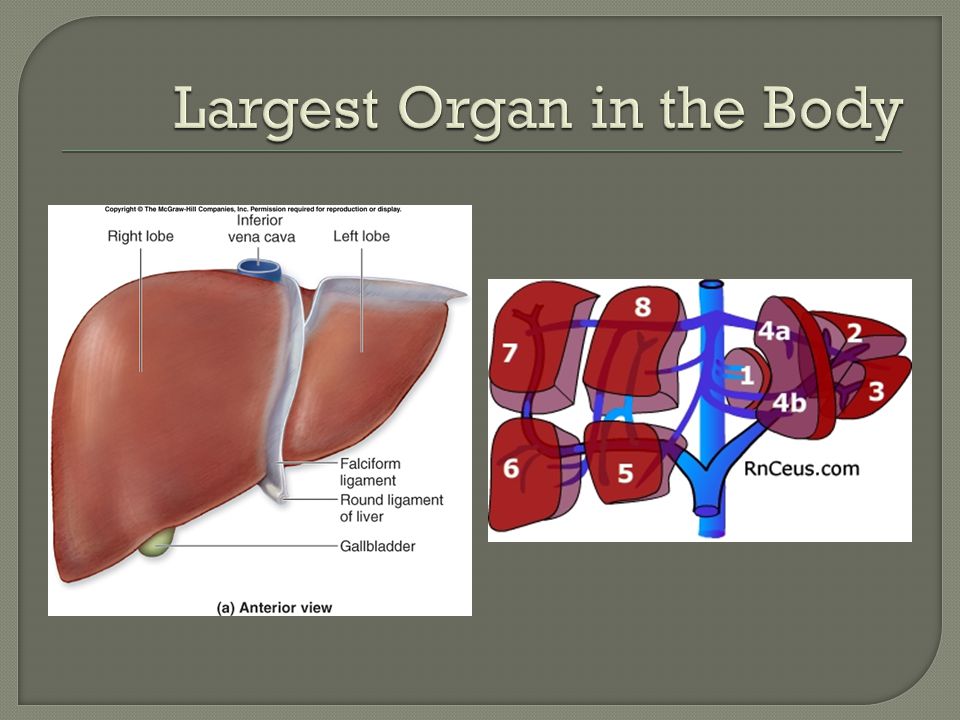
Centrilobular vein surrounded by cylinder of hepatocytes Portal triads surround lobule Hepatic arteriole Bile duct Portal venule

6
Defined by blood supply Portal Tract at the center Centrilobular veins at periphery Zone 1: Near portal tract—well- oxygenated Zone 3: Near vein— susceptible to injury

7
Normal hepatic blood flow 1500cc/min 25-30% from hepatic artery 70-75% from portal vein Oxygenation requirements supplied by both 45-50% from hepatic artery 50-55% from portal vein Liver can act as a reservoir Normally 450 cc Can hold up to 1 Liter in cases of CHF Portal Vein flow not regulated—susceptible to systemic hypotension

8
Blood-cleansing Metabolism of carbohydrates, fats, proteins, and drugs Synthesis of proteins, enzymes, clotting factors

9
Kupffer cells line sinusoids Part of monocyte- macrophage system Involved in phagocytosis, antigen processing, and release of mediators Removes bacteria and endotoxin leaving portal circulation

11
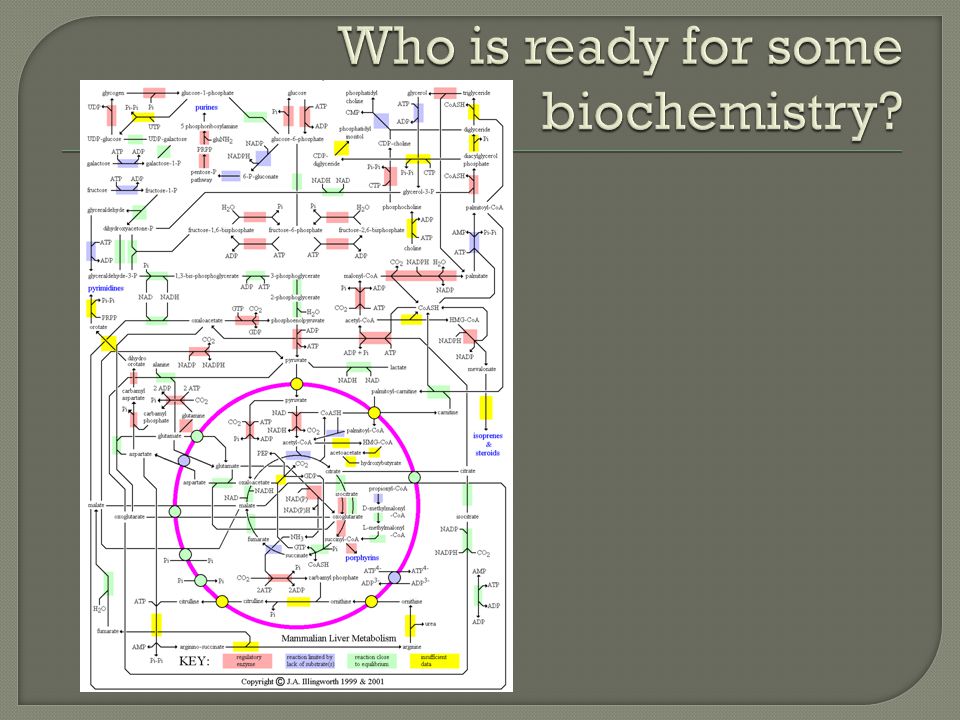
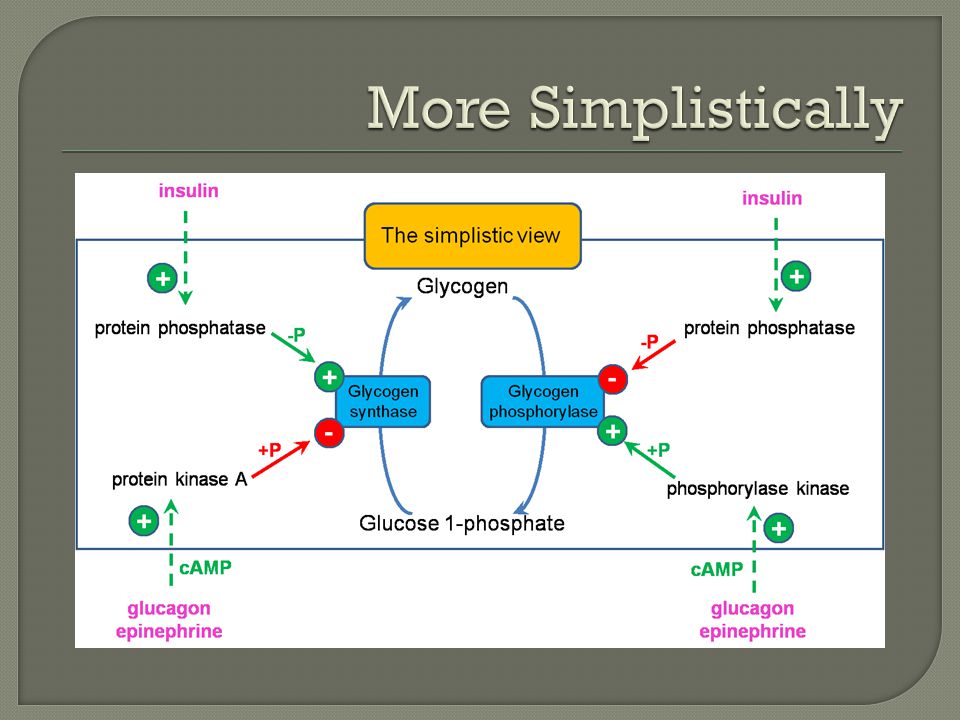
Main organ for storage and release of glucose Glycogenesis converts glucose to glycogen Big Meal Increased insulin glycogenesis Glycogenolysis breaks down glycogen to glucose Initiated by starvation, stress, or sympathetic activation Epi or Glucagon glyconeolysis Glycogen stores depleted after 24 hours

14
If carbohydrate stores are saturated, carbs converted to triglycerides. Fatty acids can be used immediately or stored for winter. Of note, RBCs only use glucose for fuel Neurons only utilize glucose except during starvation ketone bodies Fatty acids converted to Acetyl-CoA which then enters…

15
The Citric Acid Cycle! ATP produced Acetyl CoA : converts to ketone bodies Utilized in cholesterol and phospholipid production

16
Without the liver’s role in protein metabolism death would occur within several days Deamination of excess amino acids carbohydrates and fats All plasma proteins except immunoglobulins synthesized in the liver Nonessential amino acids synthesized

17
Answer: Ammonia accumulation Urea Cycle converts ammonia and CO 2 to Urea excretion by kidney

18
All plasma proteins except immunoglobulins Coagulation factors Unfortunately will talk more about this Bile formation Absorption of fat soluble vitamins

23
Most drugs undergo hepatic biotransformation Two (or three) pathways Phase I: modification of active groups by cytochrome P- 450 or mixed-function oxidases Phase II: conjugation of metabolites to water-soluble substrates elimination via urine or bile Phase III (Baby Miller): energy dependent excretion into bile Metabolism of certain drugs dependent on hepatic bloodflow LidocaineMorphineVerapamil LabetalolPropranolol
 pathways Phase I: modification of active groups by cytochrome P- 450 or mixed-function oxidases Phase II: conjugation of metabolites to water-soluble substrates elimination via urine or bile Phase III (Baby Miller): energy dependent excretion into bile Metabolism of certain drugs dependent on hepatic bloodflow LidocaineMorphineVerapamil LabetalolPropranolol")
24
Key point of drug interactions Inducers of note: barbituates, ketamine, ethanol, phenytoin, rifampin, omeprazole, isoniazid Induction increases action increased metabolism Patient exhibits increased tolerance to medications Inhibitors of note: anti-retrovirals, cimetidine, chloramphenicol, fluconazole, bupropion Inhibition decreases action decreased clearance Prolonged duration of action

25
AST (SGOT) ALT (SGPT) Alk Phos Albumin Prothrombin Time Bilirubin INR AST, ALT, Alk Phos measure hepatocellular integrity Albumin, PT, INR measure synthetic function
 ALT (SGPT) Alk Phos Albumin Prothrombin Time Bilirubin INR AST, ALT, Alk Phos measure hepatocellular integrity Albumin, PT, INR measure synthetic function")
26
Bilirubin T bili (N 3 Direct (conjugated) may reflect hepatocellular dysfunction, cholestasis, or biliary obstruction Indirect (unconjugated) seen with hemolysis or defects in bilirubin conjugation Direct bilirubin is toxic to cells Alkaline Phosphatase Produced by liver, bone, small bowel, kidneys, and placenta Majority derived from bone High levels indicate intrahepatic cholestasis or biliary obstruction
 may reflect hepatocellular dysfunction, cholestasis, or biliary obstruction Indirect (unconjugated) seen with hemolysis or defects in bilirubin conjugation Direct bilirubin is toxic to cells Alkaline Phosphatase Produced by liver, bone, small bowel, kidneys, and placenta Majority derived from bone High levels indicate intrahepatic cholestasis or biliary obstruction")
27
ALT Primarily in liver AST Present in liver, heart, skeletal muscle, kidneys AST elevating to greater extent EtOH Albumin Normal 3.5-5.5 Half-life 2-3 weeks <2.5 chronic liver disease, acute stress, or severe malnutrition

28
Measures activity of fibrinogen, prothrobin, and factors V, VII, X Half-life 4-6 hours Normal 11-14 seconds Prolongation of 3-4 s ~ INR of 1.5 Reflects Severe liver disease Vitamin K deficiency

30
Both general and regional anesthsia Volatiles reduce portal flow (Halothane > sevo > iso) Isoflurane causes direct arterial vasodilation Neuraxial techniques decrease via lowering arterial BP General anesthesia decreases via lowering BP, reducing cardiac output, and reducing sympathetic stimulation Positive pressure ventilation decrease blood flow through decrease in venous return Hypoxemia reduces flow Beta-Blockers, Alpha-1 agonists, H 2 Blockers, Vasopressin
 Isoflurane causes direct arterial vasodilation Neuraxial techniques decrease via lowering arterial BP General anesthesia decreases via lowering BP, reducing cardiac output, and reducing sympathetic stimulation Positive pressure ventilation decrease blood flow through decrease in venous return Hypoxemia reduces flow Beta-Blockers, Alpha-1 agonists, H 2 Blockers, Vasopressin")
31
Levels of catecholamines, glucagon, and cortisol increase Results in Glycogenolysis Hyperglycemia Negative nitrogen balance Stress response can be blunted by regional techniques, deep general anesthesia, or sympathetic blockade

32
Halothane directly inhibits metabolism Phenytoin Warfarin Ketamine Decreased hepatic blood flow decreases metabolism of other drugs Fentanyl, verapamil, propranolol

33
All opioids potentially cause spasm and increase biliary pressure Fentanyl > morphine > meperidine Relieved by naloxone or glucagon

34
May be due to reduction in blood flow, sympathetic stimulation, or surgery its self Elevation of LFTs postoperatively usually secondary to surgery or pre-existing disease Most common cause of post-operative jaundice is resorption of hematoma

35
Halothane Hepatitis also seen with methoxyflurane, enflurane, and isoflurane Range from asymptomatic increase in LFTs (1:5) to fulminant hepatic necrosis (1:35,000) Risk factors include Middle age Obesity Female species Repeat exposure to halothane (> if within 28 days) Diagnosis of exclusion Eliminate pre-existing disease Viral hepatitis, CMV, herpes, etc
 to fulminant hepatic necrosis (1:35,000) Risk factors include Middle age Obesity Female species Repeat exposure to halothane (> if within 28 days) Diagnosis of exclusion Eliminate pre-existing disease Viral hepatitis, CMV, herpes, etc")
36
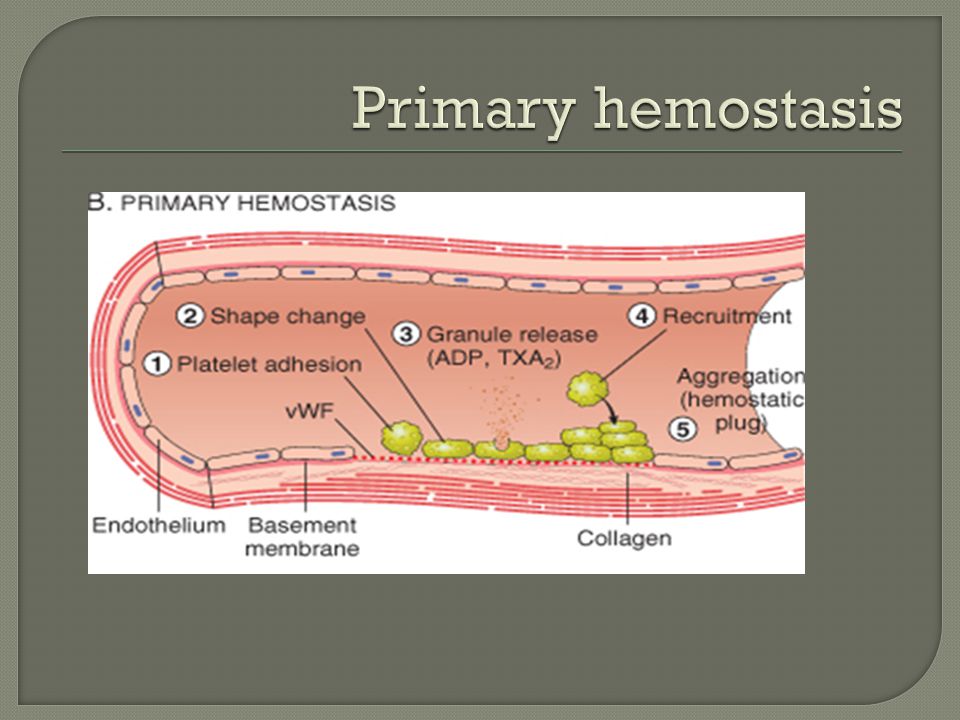
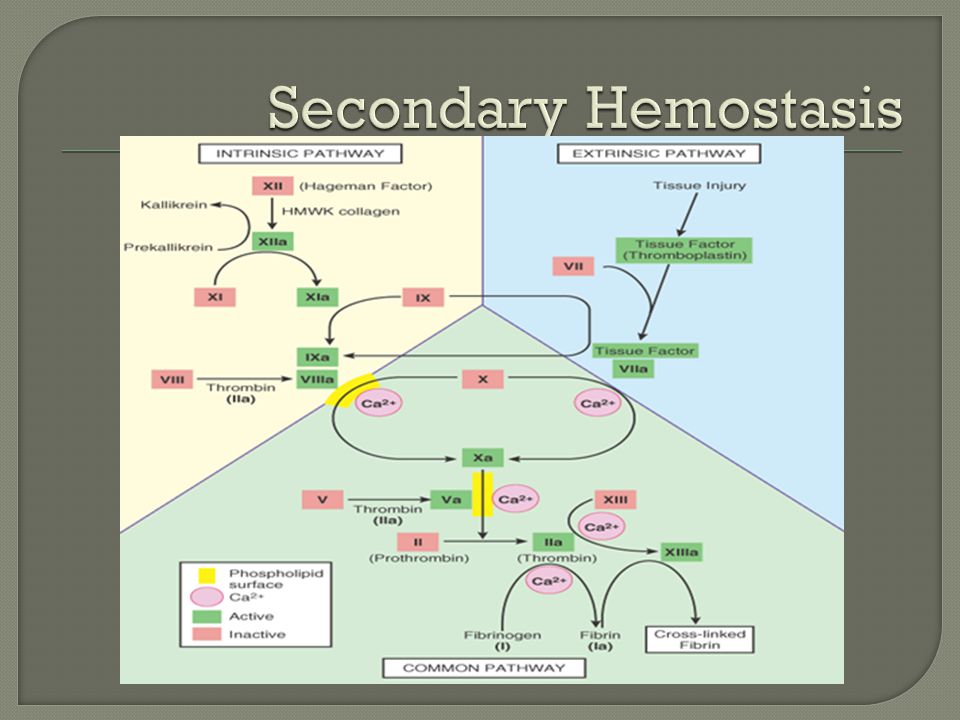
I hate my life Three processes Vascular spasm Platelet plug (primary hemostasis) Coagulation (secondary hemostasis)
 Coagulation (secondary hemostasis)")
40
Prolonged bleeding in liver disease? Vitamin K deficiency Impaired hepatic synthesis Splenic sequestration of platelets Normal PT, PTT, prolonged bleeding time? Platelet disorder Quantitative thrombocytopenia Qualitative Normal platelet count

41
Most common inherited bleeding disorder? von Willebrand’s (1:800) Most heterozygous only apparent during major bleeding Treatment DDAVP is mild Cryoprecipitate or factor VIII if no response Hemophilia A Factor VIII deficiency X-linked (1:10,000 males) Prolonged aPTT, normal PT Symptomatic if < 5% activity, raise level to 50% prior to surgery Hemophilia B (Christmas disease) Factor IX X-linked (1:100,000 males)
 Most heterozygous only apparent during major bleeding Treatment DDAVP is mild Cryoprecipitate or factor VIII if no response Hemophilia A Factor VIII deficiency X-linked (1:10,000 males) Prolonged aPTT, normal PT Symptomatic if < 5% activity, raise level to 50% prior to surgery Hemophilia B (Christmas disease) Factor IX X-linked (1:100,000 males).")
42
Vitamin K dependent factors? II, VII, IX, X Heparin mode of action? Promotes Antithrombin III What’s different about LMWHs? Inhibits Xa preferentially

43
Cutest kid?

Similar presentations














>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")

 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE ONE Dr. Essam H. Aljiffri.>")






