Download presentation
Presentation is loading. Please wait.

1
Clinical diagnosis in the acute phase of stroke – quite a challenge! Peter Sandercock Edinburgh

2
11 am. Wife notices husband speech a bit odd and right hand clumsy. Is it a stroke?

3
Clinical diagnosis in the hyperacute phase (< 6hrs) Need to be quick: ‘Time is brain’ Need to triage in A&E as potential thrombolysis / IST 3 candidate if: –known time of onset –onset less than 5 hrs ago –definite focal neurological deficit still present (use FAST or LAPSS for screening) NIHSS and OCSP classification if FAST +ve
 Need to be quick: ‘Time is brain’ Need to triage in A&E as potential thrombolysis / IST 3 candidate if: –known time of onset –onset less than 5 hrs ago –definite focal neurological deficit still present (use FAST or LAPSS for screening) NIHSS and OCSP classification if FAST +ve")
4
Harbison. Stroke 2003;34;71-76; Face Arm Speech Test (FAST) screening for paramedics/nurses
 screening for paramedics/nurses")
5
‘Acute brain attack with’ +ve FAST screen? CT ScanNon-stroke pathology Stroke: Infarct, intracerebral bleed, SAH Clinical assessment

6
Conditions that mimic acute stroke

7
Acute brain attack If NO evidence of ‘mimic, e.g.: fits/migraine Hypo/hyperglycaemia Other obvious metabolic cause DO CT CT Scan Non-stroke pathology Subdural, tumour Stroke: Infarct, intracerebral bleed, SAH

8
Non-stroke: bilateral subdural haematoma

9
Acute brain attack Exclude: fits/migraine Hypo-hyperglycaemia Other metabolic causes CT Scan Non-stroke pathology: Subdural, tumour, etc CT Normal or evidence of acute ischaemic stroke

10
Do you need a neurologist? Approximately 75% of conditions mimicking stroke are neurological How many of these can be identified by CT? ~15% of non-stroke disorders (eg subdural) found by CT rest diagnosed clinically/with other tests CT < 6hrs of ischaemic stroke often normal If CT is normal Often need stroke specialist or neurologist to confirm clinical diagnosis of stroke before thrombolysis: avoid thrombolysis for migraine, focal epilepsy, ‘functional weakness’, ischaemic deficit after subarachnoid haemorrhage! Problems of clinical diagnosis within 6 hours of onset
 found by CT rest diagnosed clinically/with other tests CT < 6hrs of ischaemic stroke often normal If CT is normal Often need stroke specialist or neurologist to confirm clinical diagnosis of stroke before thrombolysis: avoid thrombolysis for migraine, focal epilepsy, ‘functional weakness’, ischaemic deficit after subarachnoid haemorrhage. Problems of clinical diagnosis within 6 hours of onset.")
11
CT Normal MRI DWI abnormal -but DWI not widely available 2hrs ago right hemiparesis: thrombolyse?

12
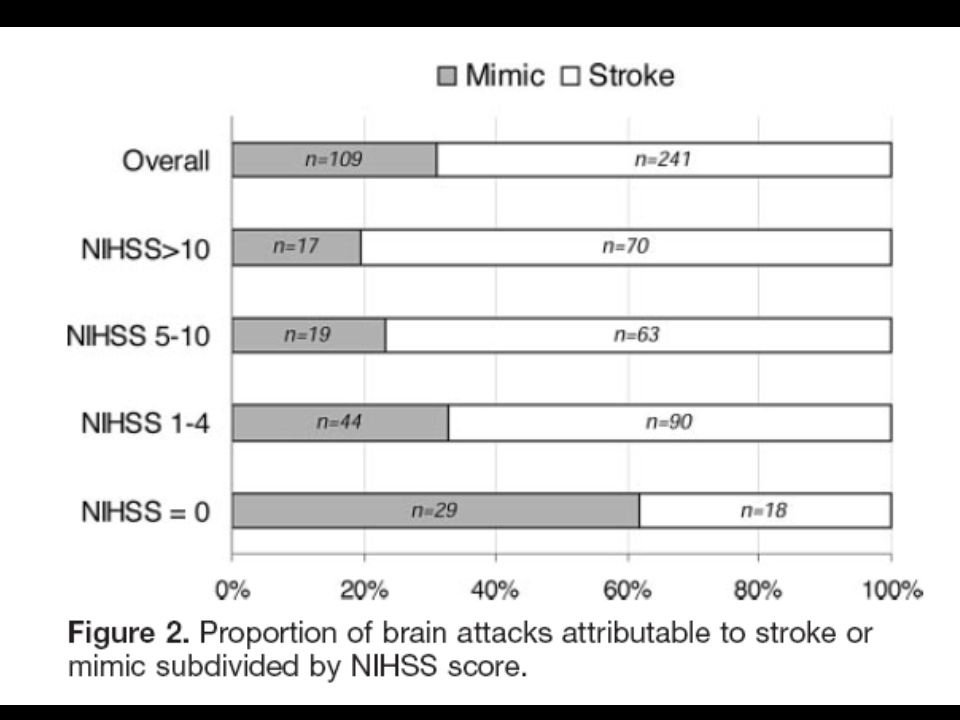
Edinburgh ‘brain attack’ study Aim Identify the ‘brain attack’ patients most likely to have acute cerebral ischaemia, potentially for thrombolysis Patients 350 admissions (336 patients) Age: 76.3 yrs (67 - 83) Source of referral to stroke team: A&E triage in 92% Time from onset to A&E: 4.7 hrs (2 - 14) Hand PJ. Stroke 2006; 37: 769-775.

13
Primary analysis ‘Thrombolysis eligible brain attacks’ (n=241) = definite stroke, probable stroke, definite TIA Mimics (n=109) = definite non-stroke, all possible stroke/TIA with a plausible non- stroke explanation
 = definite stroke, probable stroke, definite TIA Mimics (n=109) = definite non-stroke, all possible stroke/TIA with a plausible non- stroke explanation")
14
Pointers to ‘rt-PA/ist3 eligible:’ past history Pointer to ‘more likely NOT for thrombolysis/IST3’ Pointer to ‘more likely eligible’

15
Pointers to ‘rt-PA/ist3 eligible:’ History of this event

18
NIHSS training website http://asa.trainingcampus.net/uas/modules/trees/windex.aspx Note: works best with a high-speed (broadband) connection!
 connection!")
22
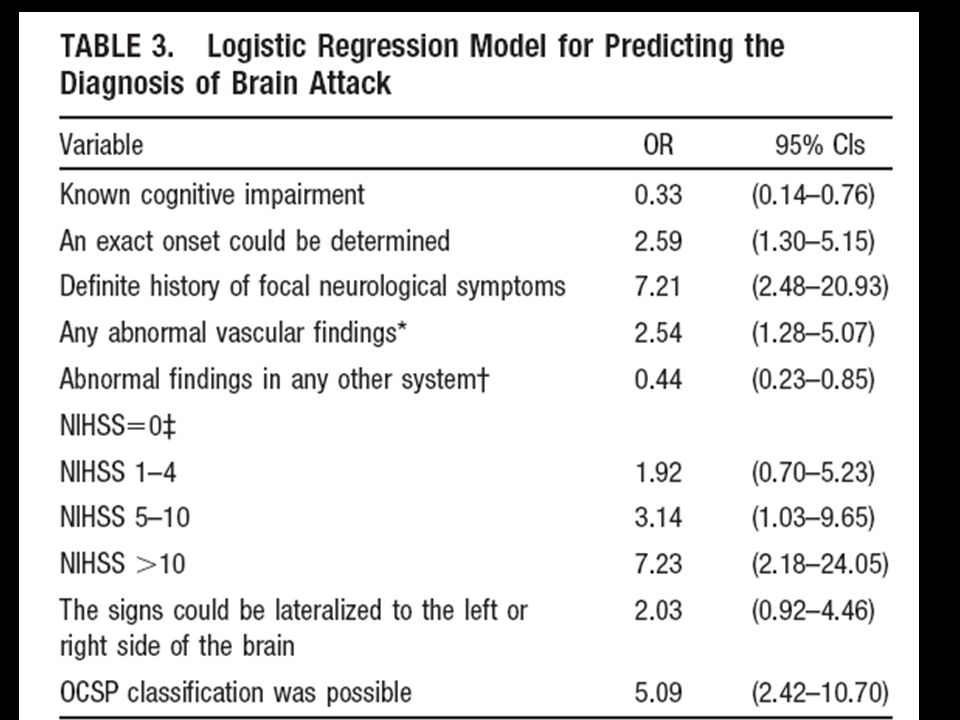
Clinical pointers: summary To ‘likely eligible for thrombolysis/ist3’ Known time of onset Abnormal vascular signs (AF, PVD) Unilateral neurological signs Can assign an OCSP classification Increasing NIH score To ‘likely not eligible’ prior cognitive impairment LOC early seizure can walk now ( too mild)
 Unilateral neurological signs Can assign an OCSP classification Increasing NIH score To ‘likely not eligible’ prior cognitive impairment LOC early seizure can walk now ( too mild)")
23
The time of onset of stroke symptoms is known precisely You have an experienced stroke physician/stroke neurologist able to see the patient urgently in A&E or at CT scan room Urgent non-contrast CT scan is interpreted by someone with expertise in acute stroke CT -> MRI not essential; its place in routine acute stroke care yet to be determined Can you diagnose ‘acute ischaemic stroke suitable for thrombolysis’ without DWI MR? Yes, if:

Similar presentations












 July 2008.>")







