Download presentation
Presentation is loading. Please wait.

2
MECHANICAL VENTILATORS By Dr. Ahmed Mostafa Assist. Prof. of anesthesia & I.C.U.

3
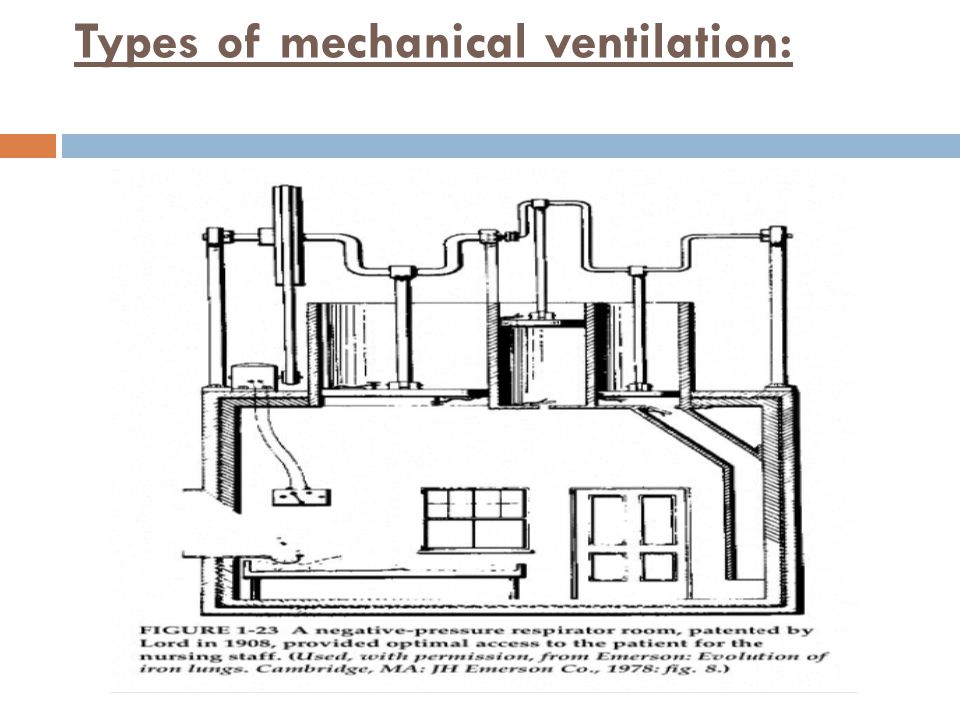
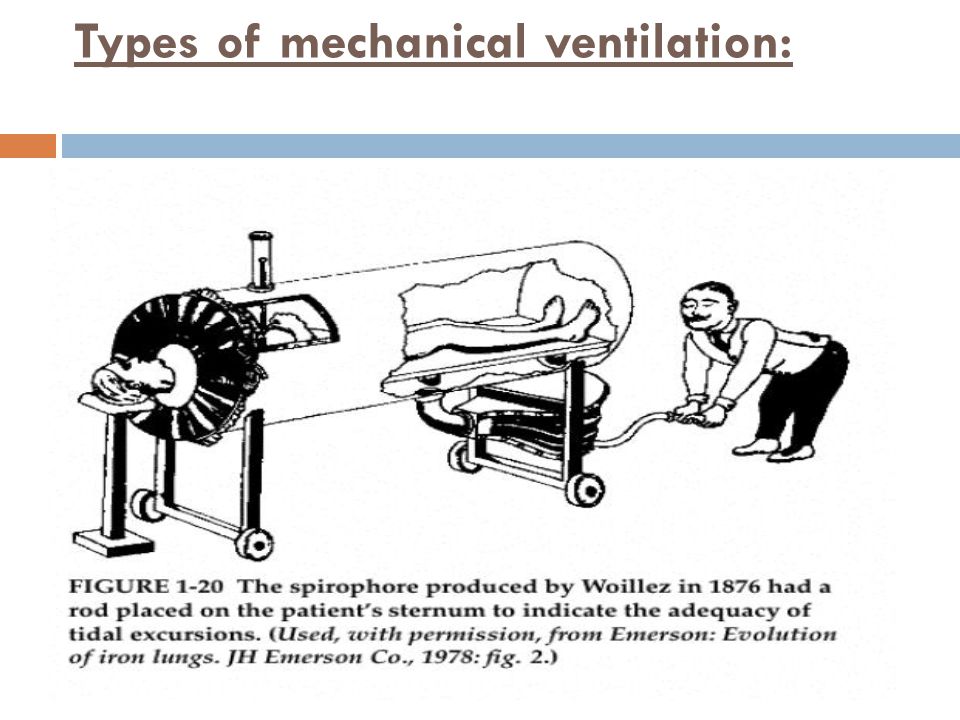
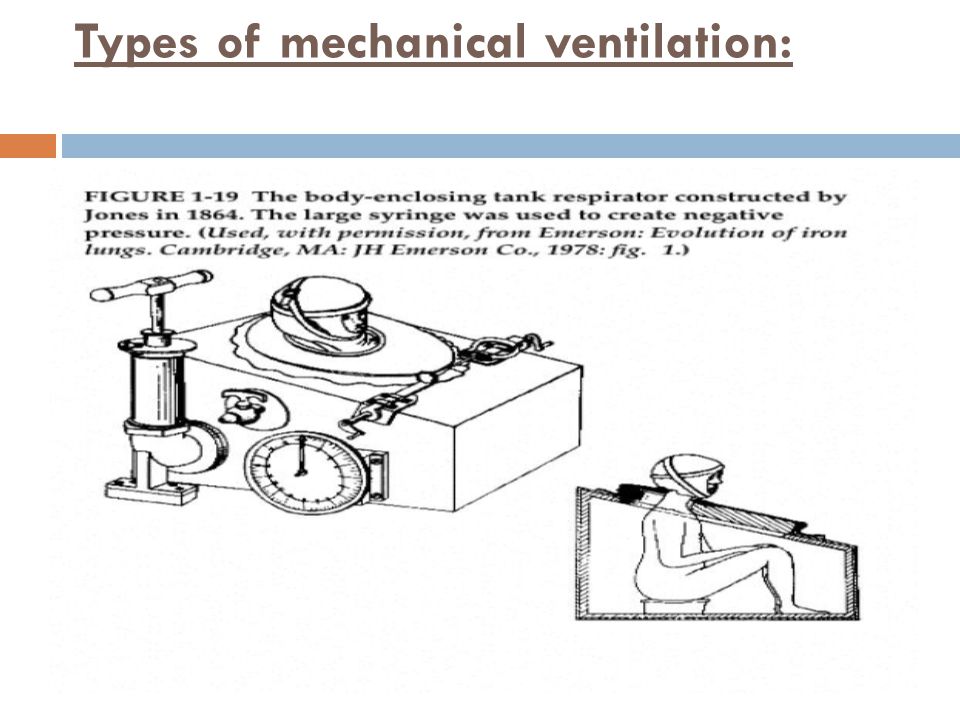
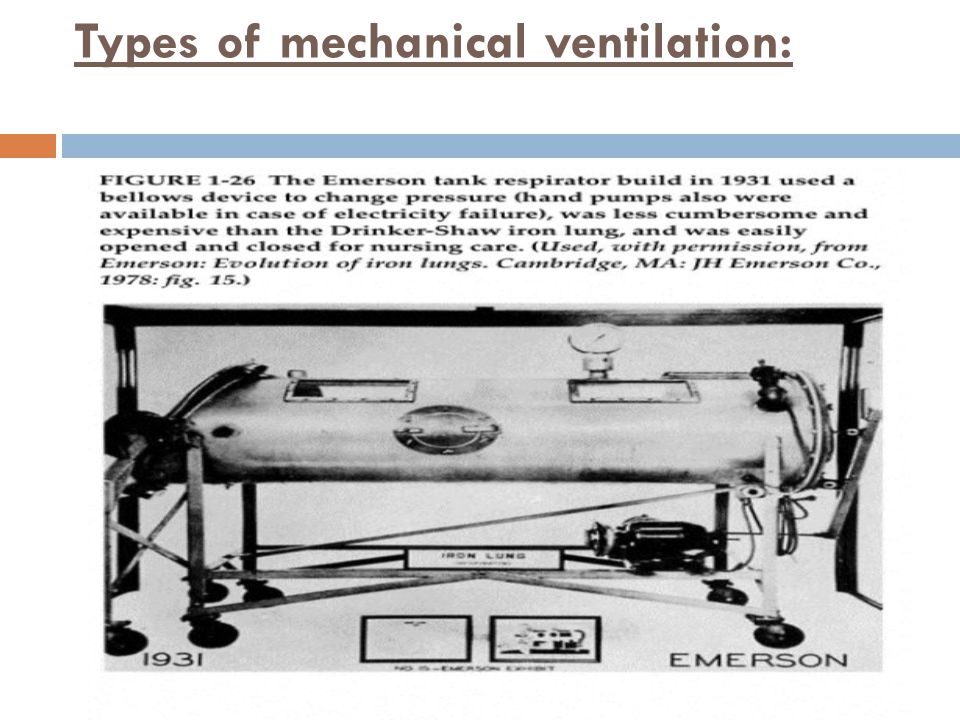
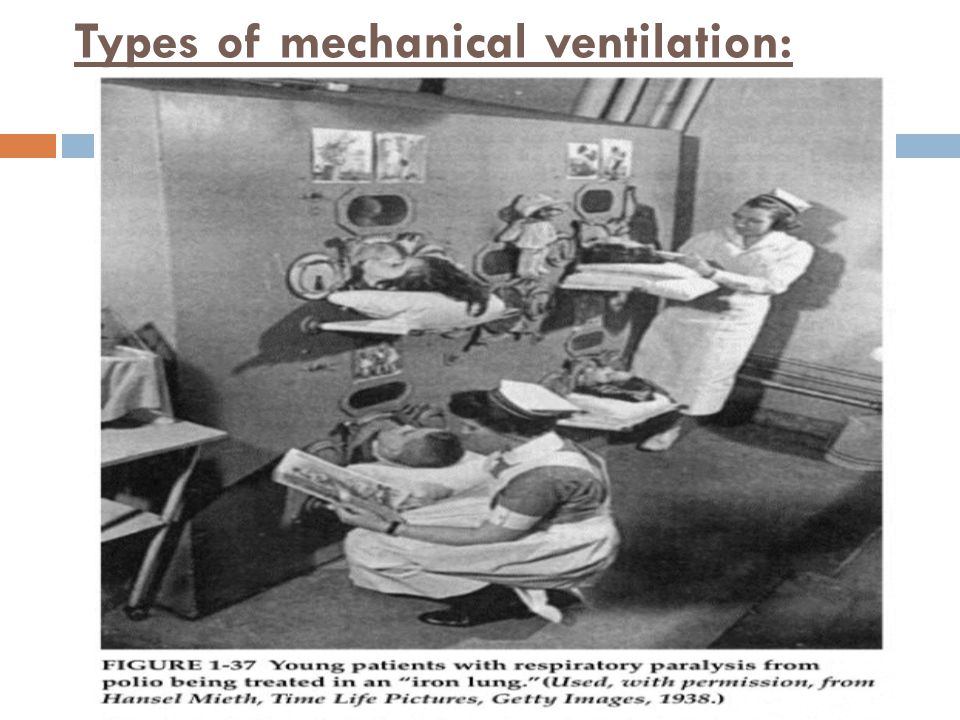
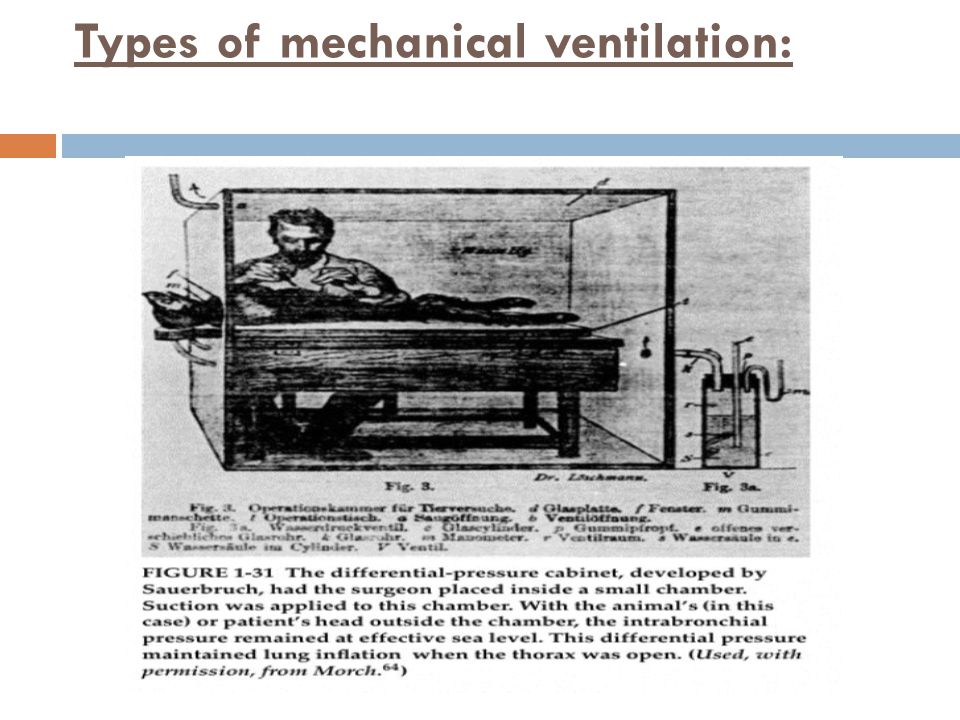
Types of mechanical ventilation: A) Negative pressure ventilation: Until the mid-1950s, mechanical ventilators used for continuous ventilation were predominantly of the negative-pressure variety. Types: 1. Around the patient’s whole body, except the head and neck: The iron lung, or tank ventilator, was the most familiar of these. 2. Around the thorax and abdomen only e.g. Cuirass ventilators.

4
Types of mechanical ventilation:

14
B) Positive pressure ventilation: Types: 1. Around the thorax and abdomen only e.g. inflatable cuirass ventilators.

15
Types of mechanical ventilation:

17
2. To the lung through a tracheal tube or mask e.g. Modern anesthesia and I.C.U. ventilators. Application of I.P.P.V.: either by: a. Invasive ventilation: with intubation. b. Non-invasive ventilation: without intubation. Either applied by 1. Noninvasive C.P.A.P. or 2. Mask mechanical ventilation.

18
Types of mechanical ventilation:

19
Advantages: 1. Avoid intubation and its complication. 2. Decrease patient’s discomfort. 3. Preserve speech and swallowing. 4. Decrease the amount of sedation. 5. Allows application of therapy. 6. Preserves lower airway defense mechanisms. 7. Effective in improving PaO 2 / FiO 2 ratio. 8. Decrease work of breathing.

20
Types of mechanical ventilation: Disadvantages: 1. Limited access for airway management. 2. Patient discomfort. 3. Leaks. 4. Needs an alert and co-operative patient.

21
Classifications: According to: 1. Power source: a. Pneumatic. b. Electrical. c. Both. 2. Ventilator circuit design: a. single circuit system. b. Double circuit system.

22
Classifications: 3.Inspiratory phase characteristics: a. Pressure generator: Constant pressure but variable volume. b. Flow generator: Constant flow and volume but variable pressure.

23
Classifications: 4.The methods of cycling from inspiration to expiration: Termination of the inspiratory phase and the beginning of the expiratory phase is triggered by one of the following: A) Pressure cycled: -These ventilators deliver a volume of air until a preset pressure is reached. - Peak inspiratory pressure is constant. - Tidal volume is variable. - Inspiratory flow is variable. - Advantages: a- Can compensate for leak. b- Protect against barotrauma. c- May recruit the collapsed alveoli. - Disadvantages: Cannot deliver enough tidal volume if there is increased airway pressure.

24
Classifications: B) Volume cycled: - These ventilators deliver a preset volume of air regardless of the pressure. - Peak inspiratory pressure is variable. - Tidal volume is constant. - Inspiratory flow is constant. - Advantages: Enough tidal volume. - Disadvantages: a. Cannot compensate for leak. b. Barotrauma.

25
Classifications: C) Time cycled: Gas flows into the lungs until a preset inspiratory time is reached. - Peak inspiratory pressure is variable. - Tidal volume is variable. - Inspiratory flow is constant.

26
Classifications: 5. Expiratory phase characteristics: a. To atmospheric pressure. b. To a certain pressure level i.e. P.E.E.P 6. The methods of cycling from expiration to inspiration: a. Time-cycling. b. Pressure-cycling. Microprocessor controlled ventilators: Most recent

27
Modes of ventilation: 1. Controlled ventilation (C.V.): - Either volume or pressure triggered. - Patient is passive. 2. Assisted controlled (A/C): - Either volume or pressure triggered. - Patient is either passive or active. 3. Intermittent mandatory ventilation (IMV): - Either volume where a minimum VT and RR are set to supplement spontaneously breathing patients. or - pressure triggered where minimum peak pressure and RR are set. - Patient is active.
: - Either volume or pressure triggered. - Patient is either passive or active. 3. Intermittent mandatory ventilation (IMV): - Either volume where a minimum VT and RR are set to supplement spontaneously breathing patients. or - pressure triggered where minimum peak pressure and RR are set. - Patient is active..")
28
Modes of ventilation: 4. Synchronized I.M.V. (SIMV): As IMV but coincide with the beginning of spontaneous effort. 5. Mandatory minute volume(MMV): Preset minute volume is set. 6. pressure support ventilation(PSV): A predetermined +ve inspiratory pressure is set to help the patient’s inspiratory effort. Pressure is applied continuously throughout inspiration at the value selected by the operator. - It is one of the weaning modes. - Decrease work of breathing. - Decrease need for sedation and muscle relaxant.
: As IMV but coincide with the beginning of spontaneous effort. 5. Mandatory minute volume(MMV): Preset minute volume is set. 6. pressure support ventilation(PSV): A predetermined +ve inspiratory pressure is set to help the patient’s inspiratory effort. Pressure is applied continuously throughout inspiration at the value selected by the operator. - It is one of the weaning modes. - Decrease work of breathing. - Decrease need for sedation and muscle relaxant..")
29
Modes of ventilation: 7. Inverse ratio ventilation(IRV) 8. Biphasic positive airway pressure(Bi-PAP). 9. High frequency ventilation(HFV). 10. Differential lung ventilation(DLV).
. 9. High frequency ventilation(HFV). 10. Differential lung ventilation(DLV)..")
30
Indications 1. respiratory gas tension: a. Direct indices: PaO2 50 mm Hg on room air. PaCO2 50 mm Hg in absence of metabolic alkalosis. b. Derived indices: PaO2 / FiO2 ratio 250 mm Hg. Pa – a O2 gradient 350 mm Hg. Va / Vt 0.6.

31
Indications 2. Clinical indices: Respiratory rate 35 breath / min. 3. Mechanical indices Tidal volume 5 ml/Kg. Vital capacity 15 ml/Kg. Maximum inspiratory force - 25 CmH2O

32
Care of patient requiring mechanical ventilation: 1. Endo tracheal intubation: - Both nasal & oral (translaryngeal) endotracheal intubation are relatively safe for at least 2-3 weeks. If prolonged period sub-glottic stenosis. So, it should be replaced by a cuffed tracheostomy tube if 2-3 weeks period is needed. - Nasal intubation is preferred for prolonged intubation ( than oral route) due to: More comfortable for the pt. More secure (least risk of accidental extubation). Leas risk of laryngeal edema.
 endotracheal intubation are relatively safe for at least 2-3 weeks. If prolonged period sub-glottic stenosis. So, it should be replaced by a cuffed tracheostomy tube if 2-3 weeks period is needed. - Nasal intubation is preferred for prolonged intubation ( than oral route) due to: More comfortable for the pt. More secure (least risk of accidental extubation). Leas risk of laryngeal edema..")
33
Care of patient requiring mechanical ventilation: 2. Initial ventilator settings Depending on the type of respiratory failure use either: a. Full ventilatory support: - by CMV, AC, SIMV, - Usually with RR 10-12 ml/kg may be needed to avoid high peak inflation pressure ( 40–50 Cm H2O) & pulmonary barotraumas as this high airway pressures promotes lung injury.
 & pulmonary barotraumas as this high airway pressures promotes lung injury..")
34
Care of patient requiring mechanical ventilation: b. Partial ventilatory support: - By SIMV using setting of 8 breaths/min. - Maintenance of some spontaneous respiratory activity preserves CO. - Less likely to change normal ventilation-perfusions matching.

35
Care of patient requiring mechanical ventilation: The aim of IPPV are: To maintain adequate oxygenation (SaO2 95 %) of tissues with an FiO2 0.5. To maintain PaCO2 at satisfactory level. Arterial oxygenation is controlled by: 1. FiO2: initially it is adjusted at 40% ( may be 50% in dame severe hypoxic pts), avoid higher conc. 50-60& to avoid reaf of O2 toxicity. Then after 10 min, AB gases is repeated to readjust FiO2. 2. PEEP: 3. IRV
, avoid higher conc. 50-60& to avoid reaf of O2 toxicity. Then after 10 min, AB gases is repeated to readjust FiO2. 2. PEEP: 3. IRV.")
36
Care of patient requiring mechanical ventilation: CO2 tension: - The aim is to produce gradual changes in PaCO2 until reaching adequate satisfactory level. - CO2 tension is controlled by Minute ventilation = RR tidal volume.

37
Care of patient requiring mechanical ventilation: 3. Sedation & Paralysis: Indications: During intubation in vigorous & uncooperative pt. Agitated patient.. During SIMV when pts continue to be tachypneic in spite of high mechanical respiratory rates ( 16-18 breaths/min) ) the work of breathing. By alone or in combination, by i.v. infusions. Opioids (morphine, fentanyl)., Benzodiazepines (diazepam, Midazolam) sedatives or Propofol. Non dep. Ms. Relaxant's paralysis.
 ) the work of breathing. By alone or in combination, by i.v. infusions. Opioids (morphine, fentanyl)., Benzodiazepines (diazepam, Midazolam) sedatives or Propofol. Non dep. Ms. Relaxant s paralysis..")
38
Care of patient requiring mechanical ventilation: 4. Monitoring: 1. Continuous ECG, pulse oximetry. 2. arterial canula for invasive ABP & repeated AB gases. 3. Fluid balance record (intake & output) so, urinary catheter. 4. CVP & PAP in hemodynamically unstable pt. 5. At least daily cheat x-ray.
 so, urinary catheter. 4. CVP & PAP in hemodynamically unstable pt. 5. At least daily cheat x-ray..")
39
Care of patient requiring mechanical ventilation: 6. Airway pressures ( peak, baseline & mean ) Exhaled tidal volume. FiO2 To: Allow optimal adjustment of ventilator setting. peak inflation pr. exhaled Vt indicate presence of large mucus plugs & presence of airway secretions. Abrupt in peak inflation pressure + sudden hypotension indicate pneumothorax.
 Exhaled tidal volume. FiO2 To: Allow optimal adjustment of ventilator setting. peak inflation pr. exhaled Vt indicate presence of large mucus plugs & presence of airway secretions. Abrupt in peak inflation pressure + sudden hypotension indicate pneumothorax..")
40
?
41
Thank you Dr. Ahmed Mostafa

Similar presentations