Download presentation
Presentation is loading. Please wait.

1
Antepartal Nursing Care
Lunar month- 4 weeks, 28 days

2
OB Terminology Pregnancy – divided into 3 trimesters 13 weeks each
EDC - estimated date of confinement EDB - estimated date of birth *same thing Gestation - number of weeks since first day of last menstrual period Abortion - birth that occurs before end of 20 weeks gestation Preterm weeks Term wks Postterm after 42 weeks Gravida -any pregnancy (any: when preg lasts 4, 5, 6wks or to term) Para - birth after 20 weeks gestation multiples count as one Stillborn - born dead after 20 weeks Primigravida - first time pregnancy Multigravida - second or any subsequent pregnancy
 Para - birth after 20 weeks gestation multiples count as one. Stillborn - born dead after 20 weeks. Primigravida - first time pregnancy. Multigravida - second or any subsequent pregnancy.")
3
Essential Components of a Prenatal History
Basis of prenatal care- reevaluated and updated throughout the pregnancy. Obstetric history – pertaining to pregnancy current and past Gynecologic history- …how long pt has had menses. Medical history - Current and past Family medical history including Father’s health history Religious, spiritual, and cultural history Occupational history Personal information about woman Comprehensive psychosocial assessment

4
Comprehensive OB History Acronym
TPAL T - term births, twins or more count as one 38 weeks P - birth from weeks A - spontaneous or therapeutic abortion L - living children- multiples count here Just knowing a woman’s gravida and para does not always provide you with the complete OB picture. The following acronym gives the entire OB story: Start with gravida then >

5
Practice Cindy is currently 34 weeks gestation and in labor with her first baby. Gravida 1 Para 0 After delivery - G 1 P 1 More detail: Gravida 1 Term 0 Preterm 1 Abortions 0 Living 1

6
Practice Mary is currently 26 weeks gestation and she has a 4 year old daughter that was born at 38 weeks gestation. G P 1 More detail: G 2 T 1 PT 0 AB 0 L 1

7
Practice Ms Johnson is pregnant for the 4th time. She had one abortion at 8 wks gestation. She has a daughter who was born at 40 wks gestation and a son born at 34 weeks gestation. G P 2 More detail: G 4 T 1 PT 1 AB 1 L 2

8
More Practice Ms T, at 27 weeks gestation, comes to the clinic for a routine prenatal visit. This is her 4th pregnancy. She has three children at home. One child was born at 34 wks gestation and the other two were 40 wks gestation. G P 3 More Detail: G 4 T 2 PT 1 AB 0 L 3

9
One More Practice Sharon is 22 wks pregnant. She has a 2 year old and a 4 year old that were born at 39 wks. She lost 4 pregnancies at 12 wks and she has 10 year old twin boys that were born at 33 wks gestation. G P 3 More detail: G 8 T 2 PT 1 AB 4 L 4

10
Determination of Due Date
Nagele’s Rule- one method of determining the EDB. Fairly accurate method to use if woman’s cycle is every 28 days. First day of LMP Subtract 3 months Add 7 days EDB Nagele’s Rule - one method of determining the EDB. Fairly accurate method to use if woman’s cycle is every 28 days. If woman unsure about when the first day of her last menses was, other methods will have to be utilized to determine EDB,

11
Nagele’s Rule Example LMP April 6 Subtract 3 months - 3 months Jan 6
Add 7 days _7 days EDB Jan 13

12
Another Option of Nagele’s Rule
Just change the month to number December 10 becomes Subtract 3 months _3___ 9 -10 Add 7 days __+_7 EDB Sept 17

14
Other Indicators of EDB
Fundal Height – correlates with weeks gestation (top of a pregnant woman's uterus (fundus) to her pubic bone) Quickening - fetal movement felt be the mom (~16-22wks, not very accurate) Fetal heartbeat - Doppler wks and wks with fetoscope. Ultrasound - most accurate Quickening - usually occurs around 20 wks but could range from wks. So, not very accurate method. Ultrasound - ID fetal sac at 5-6 wks, heart activity at 6-7 wks, crown to lump measurements, femur and biparietal measurements can determine EDC
 to her pubic bone) Quickening - fetal movement felt be the mom (~16-22wks, not very accurate) Fetal heartbeat - Doppler wks and wks with fetoscope. Ultrasound - most accurate. Quickening - usually occurs around 20 wks but could range from wks. So, not very accurate method. Ultrasound - ID fetal sac at 5-6 wks, heart activity at 6-7 wks, crown to lump measurements, femur and biparietal measurements can determine EDC.")
15
Initial Physical Assessment
Head to toe physical assessment 8-12 wks gestation Starts with VS and ends with pelvic exam. A complete head to toe physical assessment is done on the first visit with the provider to mainly establish baselines and identify any issues that may have a impact on the pregnancy. Usually the first assessment is done at about 8-12 wks gestation The exam starts with assessment of vital signs, proceeds through a head-to-toe assessment and ends with the pelvic exam.

16
Pregnancy Physical Assessment
Blood pressure - trimester specific changes (1st tri = BP drops and will rise towards the 3rd) Weight - sudden wt gain Skin - pigmentation ENT - nosebleeds and swollen gums, dental infection preterm labor Breast – enlarge, colostrum 12 wks Abdomen - becomes larger, measured each visit (Fundal Height Measurement) Blood pressure > trimester specific changes. Could exhibit pregnancy related hypertension after about 20 wks gestation Weight > sudden wt gain in a short period of time could be related to PIH (pregnancy induced HTN) Skin > pigmentation changes normal ENT > nosebleeds and swollen gums may be expected, poor dental situation associated with preterm labor Breast > enlarge, “feel heavy”, pigmentation changes, colostrum formation at about 12 wks Abdomen > becomes larger, stretch marks,
 Weight - sudden wt gain. Skin - pigmentation. ENT - nosebleeds and swollen gums, dental infection preterm labor. Breast – enlarge, colostrum 12 wks. Abdomen - becomes larger, measured each visit (Fundal Height Measurement) Blood pressure > trimester specific changes. Could exhibit pregnancy related hypertension after about 20 wks gestation. Weight > sudden wt gain in a short period of time could be related to PIH (pregnancy induced HTN) Skin > pigmentation changes normal. ENT > nosebleeds and swollen gums may be expected, poor dental situation associated with preterm labor. Breast > enlarge, feel heavy , pigmentation changes, colostrum formation at about 12 wks. Abdomen > becomes larger, stretch marks,")
17
Fundal Height Measurement
Measure in centimeters from the top of the symphysis pubis to the top of the uterine fundus. weeks - fundal height correlate with weeks of gestation Too small or too large - needs to be evaluated.

18
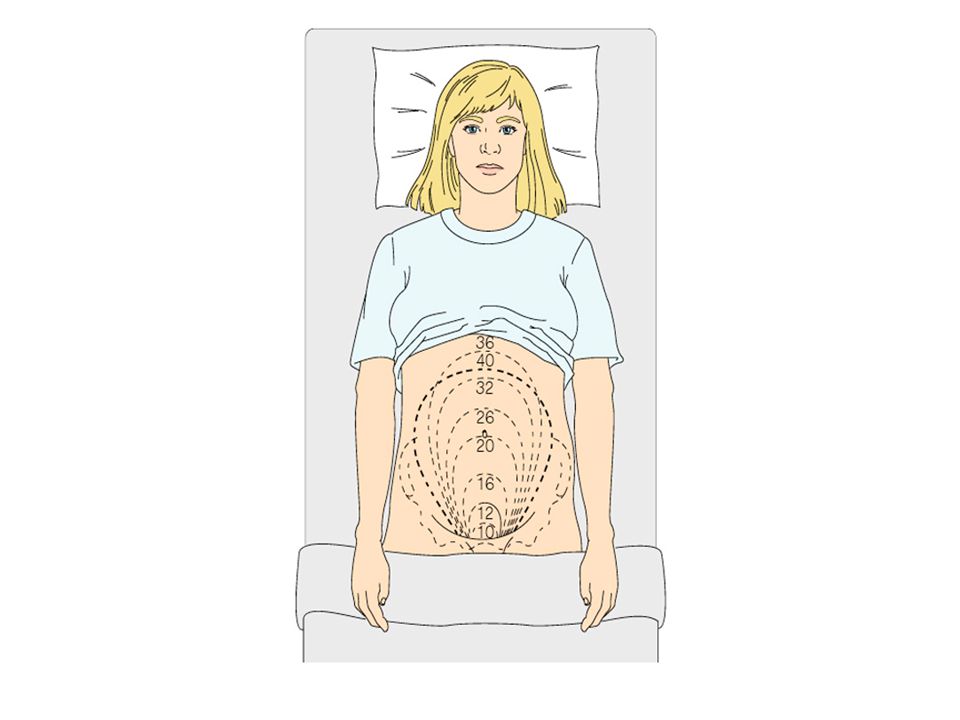
Figure 8–3 A cross-sectional view of fetal position when McDonald’s method is used to assess fundal height.

19
Fundal Height Assessment
10-12 wks - fundus slightly above symphysis pubis 16 wks - fundus halfway between symphysis and umbilicus 20-22 wks - fundus at umbilicus 28 weeks - fundus three finger breadths above umbilicus 36 wks - fundus just below ensiform cartilage

21
Abdominal Assessment Fetal movement felt by examiner -18 weeks
Ballotment - Fetus floating in amniotic fluid Fetal heart tones BPM Doppler 10-12wks Fetoscope wks Palpate fetal movement > felt by examiner at about 18 weeks Ballotment > noted beginning the 4-5 month. Fetus floating around in amniotic fluid Fetal heart tones > Bpm, may be heard by doppler 10-12wks gestation; heard with fetoscope at wks.

22
Physical Assessment cont
Extremities - edema of hands and feet in later pregnancy Reflexes - hyperactivity or clonus associated with preeclampsia Pelvic - Pelvic measurement assessed for shape and size; dilatation and effacement Rectum - hemorrhoids (if already present, give advice about incr fiber and fluids)
")
23
Initial Laboratory Evaluation and Screening
CBC (Anemia give more iron) ABO and Rh typing, Antibody Screen, Blood type Serolgy (RPR tests for syphilis) Rubella Hepatitis HIV PAP smear STD screen Urinalysis – C&S; drug screen, can have a UTI that is asymptomatic Thyroid panel- because of chance of cretinism
 ABO and Rh typing, Antibody Screen, Blood type. Serolgy (RPR tests for syphilis) Rubella. Hepatitis. HIV. PAP smear. STD screen. Urinalysis – C&S; drug screen, can have a UTI that is asymptomatic. Thyroid panel- because of chance of cretinism.")
24
Subsequent Prenatal Visit Routines
Every 4 weeks until 28 wks Every 2 wks until 36 wks Every wk until delivery Visits include teaching and assessment of maternal/fetal well-being.

25
Subsequent Prenatal Assessments
Vital signs Weight - 1st trimester > 3.5 – 5lbs 2nd and 3rd trimester > lbs, then a lb per wk Monitor for Edema Uterine size and uterine activity FHT’s and fetal movement Urine screen for protein, glucose and ketones Lab CBC at 7 months AFP at wks Indirect coombs for Rh negative moms at 28 wks Glucose screen 28 wks GBS vag culture 36 wks, “Group B Strept”- Carriers must understand the dangers for the baby. Define: AFP- Alpha Fetal Protein, measurements in amniotic fluid are used for early diagnosis of fetal neural tube defects High = Neural Tube defect (ex: spina bifida) Low = Down’s Syndrome
 Low = Down’s Syndrome.")
26
Danger Signs in Pregnancy
Vaginal bleeding (Any bright red bleeding call phys) Nausea and vomiting that last over 24hrs Dehydration leads to preterm labor Fever Dizziness - sudden and extreme, associated with pelvic or uterine pain True Labor- Lower back pain to the front False labor- Abd pain only Preterm labor symptoms Leaking of fluid from vagina Preeclampsia symptoms - edema, rapid wt gain, headaches, visual disturbances, vomiting, epigastric pain, irritability, scanty urine output (usually won’t see till after 20wks) Decreased fetal movement Symptoms of UTI - dysuria, severe backache, fever
 Nausea and vomiting that last over 24hrs. Dehydration leads to preterm labor. Fever Dizziness - sudden and extreme, associated with pelvic or uterine pain. True Labor- Lower back pain to the front. False labor- Abd pain only. Preterm labor symptoms. Leaking of fluid from vagina. Preeclampsia symptoms - edema, rapid wt gain, headaches, visual disturbances, vomiting, epigastric pain, irritability, scanty urine output (usually won’t see till after 20wks) Decreased fetal movement. Symptoms of UTI - dysuria, severe backache, fever.")
27
1st Trimester Discomforts and Measures to Alleviate
Nausea (due to HcG levels) and vomiting - avoid odors, eat small frequent meals, crackers, avoid spicy or greasy foods HcG- a hormone produced by the placenta about 10 days after fertilization. Its detection is the basis for most pregnancy tests. Urinary frequency - void when needed; increase fluids in day and slow down at night Fatigue - plan rest periods, get help from support system Breast tenderness - wear good supportive bra Increased vaginal discharge - frequent bathing, cotton underwear Nasal stuffiness & epistaxis - cool mist, avoid nasal decongestants and sprays Ptyalism – “excessive saliva/bad taste in mouth” treat w/ mouthwash, chewing gum, candy N&V - seen in about 85% of pregnancies; many times caused by increased hCG levels Urinary frequency > due to pressure of enlarging uterus Fatigue > may be aggravated by nocturia Breast tenderness > from increased estrogen and progesterone Increased vaginal discharge > from hyperplasia of vaginal mucosa Nasal stuffiness and epistaxis > elevated estrogen produces edema of nasal passages Ptyalism > cause unknown
 and vomiting - avoid odors, eat small frequent meals, crackers, avoid spicy or greasy foods. HcG- a hormone produced by the placenta about 10 days after fertilization. Its detection is the basis for most pregnancy tests. Urinary frequency - void when needed; increase fluids in day and slow down at night. Fatigue - plan rest periods, get help from support system. Breast tenderness - wear good supportive bra. Increased vaginal discharge - frequent bathing, cotton underwear. Nasal stuffiness & epistaxis - cool mist, avoid nasal decongestants and sprays. Ptyalism – excessive saliva/bad taste in mouth treat w/ mouthwash, chewing gum, candy. N&V - seen in about 85% of pregnancies; many times caused by increased hCG levels. Urinary frequency > due to pressure of enlarging uterus. Fatigue > may be aggravated by nocturia. Breast tenderness > from increased estrogen and progesterone. Increased vaginal discharge > from hyperplasia of vaginal mucosa. Nasal stuffiness and epistaxis > elevated estrogen produces edema of nasal passages. Ptyalism > cause unknown.")
28
2nd and 3rd Trimester Discomforts and Measures to Alleviate
Pyrosis – “hrt burn” treat w/ small frequent meals, avoid spicy or greasy meals, sit or stand after meal Ankle edema - rest frequently, elevate legs when resting, avoid garters Varicose veins - elevate legs, wear support hose, avoid crossing legs, avoid constrictive bands Flatulence - avoid constipation and gas producing foods Hemorrhoids - avoid constipation Constipation - increase fluids and fiber in diet, exercise, stool softeners as ordered by physician Make sure softeners are okay’d by phys first. Pyrosis > from displaced stomach due to enlarged uterus, progesterone relaxes cardiac sphincter of stomach and decreases GI motility Ankle edema > decreased venous return Varicose veins > from pressure of enlarged uterus that prevents good venous return Flatulence > from increased progesterone that decreases GI motility, and pressure of uterus on the large intestine Hemorrhoids > from underlying constipation, increased blood volume, and uterine pressure on veins Constipation > increased progesterone, displaced intestines from enlarging uterus, possibly from iron intake

29
2nd and 3rd Trimester Discomforts and Measures to Alleviate cont
Backache - proper body mechanics; avoid high heels, practice pelvic tilt exercise Leg cramps - dorsiflexing foot Faintness - rise slowly from sitting or lying, evaluate hematocrit and hemoglobin Shortness of breath - eat small frequent meals Difficulty sleeping - prop with pillows, use side-lying position Lt Side is better for baby Round ligament pain - position change, heating pad Carpal tunnel syndrome - avoid repetitive movements of hands Backache > lumbosacral curve as uterus enlarges and becomes heavier Leg cramps > pressure from uterus on pelvic nerves or blood vessels Faintness > from increased blood volume and postural hypotension from blood pooling in legs Shortness of breath > from enlarging uterus pressing on diaphragm, which decreases vital capacity Difficulty sleeping > difficult to find comfortable position Round ligament pain > from stretching due to enlarging uterus Carpal tunnel syndrome > from compression of the median nerve in the wrist

30
Promotion of Self Care During Pregnancy
Fetal activity monitoring - after 28 wks Breast care and preparation for breastfeeding Prenatal classes and exercises Clothing Bathing Employment Travel- wear safety belts, travel only if you have no problems, stop every 2 hrs, stay hydrated Activity Fetal activity monitoring - after 28 wks Breast care and preparation for breastfeeding, well fitted bra Prenatal classes and exercises Clothing - loose nonconstricting, no high heels Bathing - bathe daily, tub safety Employment - may have to alter to decrease fatigue, careful with exposure, related to SGA Travel > wear safety belts, travel only if you have no problems, stop every 2 hrs, stay hydrated Activity and rest > rest important, may continue prepregnant activity

31
Promotion of Self Care During Pregnancy cont
Dental Care Immunizations Complementary and alternative therapy Before anything over the counter they need to talk to their phys Tertatogens Medications Categories A – X, pg. 247 – 249; Cat. A is safe during Preg. No to Accutane!! Tobacco- IUGR Growth retardation, Tobacco vasocontricts! Alcohol Caffeine- limit intake Street drugs Flu Vaccine is okay, just not live ones. Dental care > important, poor dental hygiene associated with preterm labor Immunizations - immunizations using killed viruses may be used during pregnancy Complementary and alternative therapy > only under physicians direction Medications Tobacco - IUGR Alcohol – Fetal Alcohol syndrome Caffeine – limit intake Street drugs – ch. 14 Dental care > important, poor dental hygiene associated with preterm labor

32
Concerns About Sexual Activity
Safety for fetus Contraindications PROM “Premature rupture of membranes” (water-break), preterm labor, vag bleeding Changes in sexual desire and response pregnant woman partner
, preterm labor, vag bleeding Changes in sexual desire and response. pregnant woman. partner.")
33
Nursing Care of the Pregnant Woman’s Family
Father – involved, participation Siblings – regression, rivalry Grandparents – involvement, conflicts > assess his knowledge level and intended degree of participation and then work with the couple to assure they meet their goals for this pregnancy

Similar presentations


















 Maternal Newborn Nursing Care. Forth Edition. Addison Wesley.>")
