Download presentation
Presentation is loading. Please wait.

1
Oncologic Emergencies Mauricio Burotto MD National Cancer Institute National Institutes of Health

2
Oncologic Emergencies Concepts Can be at presentation or during the evolution of the malignancy Usually caused by the tumor itself (primary or metastasis) or secondary to humoral factors Also an oncologic emergency can be related to the cancer treatment
 or secondary to humoral factors Also an oncologic emergency can be related to the cancer treatment")
3
Oncologic Emergencies Concepts –Primary : SVC syndrome related to a NSCLC –Metastasis : Cord compression –Humoral : Hypercalcemia, Hyponatremia

4
Oncologic Emergencies Classification Structural or mechanica l Metabolic or humoral

5
Oncologic Emergencies Concepts Emergency related to the cancer treatment –Chemotherapy TLS –Targeted Agents Hemorrhage Bowel perforation “Allergic reaction” → Infusion reaction

6
Brain metastasis Metastasis to the brain is the most common neurologic complication of cancer (40%) Suspicion at the presentation of any neurological deficit or –Nausea and vomiting –Altered mental status –Seizures
 Suspicion at the presentation of any neurological deficit or –Nausea and vomiting –Altered mental status –Seizures")
7
Brain metastasis Diagnosis Contrast-enhanced CT –Without contrast in patient with known lesions when hemorrhage is suspected MRI with gadolinium phase –More sensitive and better for posterior fossa –Expensive –Longer

8
Melanoma metastasis

9
Brain metastasis Emergencies Intracranial hypertension (ICP) –Herniation Hemorrhagic stroke Seizures
 –Herniation Hemorrhagic stroke Seizures")
10
Increased ICP Management Corticosteroids are routinely used to treat increased ICP caused by brain metastasis by reducing vasogenic cerebral edema. Dexamethasone Osmotic diuresis: Mannitol and hypertonic saline Intensive Care: ICP monitoring and Hyperventilation

12
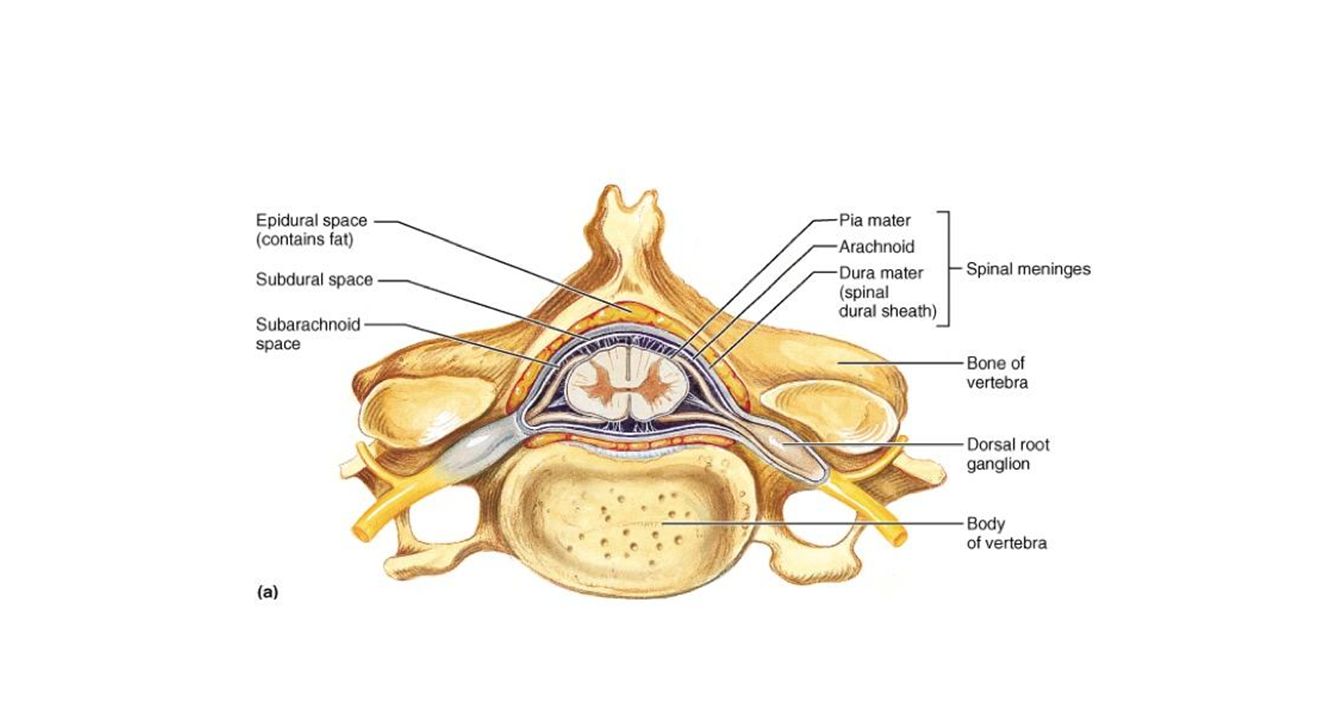
Malignant cord compression Called epidural spine compression (ESCC) Defined as : Compression of the dural sac and its contents by an extradural tumor mass. The minimal radiological evidence for SCC is indentation of the theca at the level of the clinical symptoms Anatomical Causes: Epidural compression by tumor mass or pathological Fx of the vertebrae and retropulsion of bony fragments into the canal

14
Malignant cord compression

15
Probability in patient with cancer 2-5% –LUNG, BREAST, MYELOMA, PROSTATE Consequences: irreversible loss of neurologic function Clinical presentation: pain, (seven weeks before neurologic symptoms), weakness, bladder and bowel dysfunction (later)
, weakness, bladder and bowel dysfunction (later)")
16
Malignant cord compression Distribution Thoracic spine 50-70% Cervical 10-30% Lumbosacral 20-30%

17
Malignant cord compression Diagnosis History and physical examination Imaging –Spine X ray –CT scan –MRI

18
Malignant cord compression Diagnosis History and physical examination –Basic neurologic examination ALWAYS!!! Imaging –Spine X ray –CT scan –MRI of the entire spine

19
Malignant cord compression Treatment Symptomatic treatment: –Pain control, anticoagulation*,avoid constipation Glucocorticoids –Not clarity between initial high vs low dose (range 10 to 100 Dexamethasone ) then 16 mg in divided doses
 then 16 mg in divided doses")
20
Malignant cord compression Treatment Definitive treatment: spinal stability, type of tumor and grade of cord compression Surgery : resection + stabilization → Rdt Radiation : –Radiosensitive : Lymphoma, SCLC, MM, Seminoma –Radioresistance : Melanoma, RCC, CRC, Sarcoma –Dose and schedule : Range (8Gy x1 to 40Gy x20 ) Prognostic factors associated with shortened survival after RT include relatively radioresistant histology, the presence of visceral metastases or other bone metastases, non-ambulatory status at treatment, an interval from the original diagnosis to ESCC ≤15 months, and an interval <14 days from the onset of motor symptoms to the initiation of RT
 Prognostic factors associated with shortened survival after RT include relatively radioresistant histology, the presence of visceral metastases or other bone metastases, non-ambulatory status at treatment, an interval from the original diagnosis to ESCC ≤15 months, and an interval <14 days from the onset of motor symptoms to the initiation of RT")
21
Malignant cord compression Treatment Stereotactic body radiotherapy (STBR) –SBRT with a single 16-24 Gy fraction gives excellent tumor control, even in patients who have relatively radioresistant tumors. Chemotherapy

22
Greater than 50 percent vertebral body collapse Subluxation/translation Bilateral facet destruction Movement-related pain Patients with a score of 7 or higher –Spine Instability Neoplastic Score (SINS)
")
23
Superior vena cava syndrome

26
Any condition that leads to obstruction of blood flow through the SVC

27
Superior vena cava syndrome Malignancy accounts for 60% to 85% of cases –20% to 40% intravascular devices causing thrombosis. –Lung cancer and non-Hodgkin lymphoma are responsible for most cases Symptom severity depends on the extent of the obstruction and its rapidity of onset – Dyspnea, facial swelling, and distended neck veins –Collaterals develop over time and slow the progression symptoms

28
Superior vena cava syndrome Diagnosis Chest x ray –Abnormal in 80% of the cases : Widening and pleural effusion US –First test in patients with vascular devices who present with extremity swelling. CT Chest –Test of choice : identification of the cause and collaterals

29
Superior vena cava syndrome Management Emergent treatment is indicated in patients with airway obstruction or laryngeal edema. However, SVC syndrome most commonly develops gradually, and treatment can be delayed until the primary diagnosis is established. Radiation (NSCLC) Steroids (NHL and Thymoma) Chemotherapy (SCLC, testicular, NHL)
 Steroids (NHL and Thymoma) Chemotherapy (SCLC, testicular, NHL).")
30
Superior vena cava syndrome Management Angioplasty and stenting Surgery Thrombolytic therapy The American College of Chest Physicians recommends establishment of a histologic diagnosis before instituting treatment in stable patients

31
Superior vena cava syndrome Management Always try to obtain and histologic diagnosis Exceptions Central airway obstruction Coma because of cerebral edema

32
Pericardial tamponade

33
Pericardial effusion Thoracic radiation –During radiation of early after finished –Recall reaction Infectious Paraneoplastic autoimmune –Immunotherapies for cancer

34
Pericardial effusion The most common primary malignancy involving the pericardium is lung (2 nd breast) Pericardial tamponade is an increase in intrapericardial pressure that impairs intracardiac filling and cardiac output. Very rare*** Don’t forget primary tumor from the pericardium –Mesothelioma

35
Pericardial tamponade Diagnosis and Treatment Echocardiography –Right atrial collapse is a more sensitive marker of pericardial tamponade, whereas right ventricular collapse is more specific. Emergent pericardiocentesis –Indwelling catheter –Window

36
Intestinal emergencies Acute bowel obstruction –CRC 10-30% –Ovarian Cancer 20-50%* –Treatment options: surgery, endoscopic intervention, and pharmacologic palliation; self- expanding metallic stents Perforation –CRC and lymphomas –Targeted agents: Anti-angiogenic agents Bevacizumab

37
Tumor lysis syndrome The tumor lysis syndrome is the most common disease-related emergency in hematological malignancies Potential consequences –Renal failure –Cardiac arrhythmias –Seizures –Death

38
Tumor lysis syndrome Usually after treatment (most effective most probable) –Can be spontaneous Most common hematological malignancies compared with solid tumors but… –LMA and NHL –Combination chemotherapy –Targeted agents : started to be reported
 –Can be spontaneous Most common hematological malignancies compared with solid tumors but… –LMA and NHL –Combination chemotherapy –Targeted agents : started to be reported")
39
Tumor lysis syndrome Syndrome that may include : hyperkalemia hyperphosphatemia hypocalcemia hyperuricemia massive tumor cell death

40
Cairo and Bishop definition

42
Management Hydration Allopurinol* Rasburicase: most widely accepted dosing is based on the 2008 International Expert Panel on TLS, which suggests a dose of 0.1 mg/kg daily for TLS prevention and 0.2 mg/kg daily for TLS treatment Alkalinization: not longer recommended

46
Hypercalcemia Hypercalcemia is the most common oncologic metabolic emergency (10% to 30% at some point during disease course) It is defined as a total serum calcium concentration greater than 10 mg/dL or an ionized calcium concentration greater than 5.6 mg/dL.
 It is defined as a total serum calcium concentration greater than 10 mg/dL or an ionized calcium concentration greater than 5.6 mg/dL.")
47
Mechanisms Humoral hypercalcemia of malignancy –80% of cases PTHrP Local osteoclastic hypercalcemia 1,25(OH)2D-secreting lymphomas Ectopic hyperparathyroidism
2D-secreting lymphomas Ectopic hyperparathyroidism")
48
Hypercalcemia Presentation Neurologic symptoms –Lethargy, confusion (coma) Gastrointestinal –Constipation, Nausea, Anorexia –Pancreatitis Renal –Nephrogenic diabetes insipidus (Poliuria, polidipsea)
 Gastrointestinal –Constipation, Nausea, Anorexia –Pancreatitis Renal –Nephrogenic diabetes insipidus (Poliuria, polidipsea)")
49
Diagnosis Measurement –Always check with albumin and correct –Ideally check ionized calcium Levels –Mild <12 mg/dL [3 mmol/L] –Moderate 2 to 14 mg/dL [3 to 3.5 mmol/L] –High >14 mg/dL [3.5 mmol/L]
![Diagnosis Measurement –Always check with albumin and correct –Ideally check ionized calcium Levels –Mild <12 mg/dL [3 mmol/L] –Moderate 2 to 14 mg/dL [3 to 3.5 mmol/L] –High >14 mg/dL [3.5 mmol/L]](http://images.slideplayer.com/17/5316667/slides/slide_49.jpg "Diagnosis Measurement –Always check with albumin and correct –Ideally check ionized calcium Levels –Mild <12 mg/dL [3 mmol/L] –Moderate 2 to 14 mg/dL [3 to 3.5 mmol/L] –High >14 mg/dL [3.5 mmol/L]")
50
Hypercalcemia Treatment Hydration (volume expansion) –NaCL 0,9% 150-200 ml urine output 80-100 ml –Loop Diuretics ??? Bisphosphonates –Always in high Ca+ almost always in moderate –Check renal function –Maximum effect in two to four days –Zolendronic Acid (4mg over 15-20 min) –Pamidronate ( 60-90-mg over 2 hours)
 –Pamidronate ( mg over 2 hours).")
51
Hypercalcemia Treatment RANKL inhibitors –Denusumab ** recommended patients with zoledronic acid (ZA)-refractory hypercalcemia 6-120 sc –Can be used in the setting of renal dysfunction –Can cause hypocalcemia (Check vit D levels before ) Steroids: Lymphomas ( granulomatous component) Calcitonin (only in symptomatic patients with high Ca+) Hemodialysis
-refractory hypercalcemia sc –Can be used in the setting of renal dysfunction –Can cause hypocalcemia (Check vit D levels before ) Steroids: Lymphomas ( granulomatous component) Calcitonin (only in symptomatic patients with high Ca+) Hemodialysis")
52
Hypophosphatemia Associated with Cancer Tumor-induced osteomalacia (TIO) tumor production of phosphaturic factors → FGF- 23 results in phosphate wasting –Chondrosarcoma and hemangiopericitoma Hypophosphatemia in hypercalcemia context –Hyperparathyroidism Hypophosphatemia in hypocalcemia context –Vit D deficiency
 tumor production of phosphaturic factors → FGF- 23 results in phosphate wasting –Chondrosarcoma and hemangiopericitoma Hypophosphatemia in hypercalcemia context –Hyperparathyroidism Hypophosphatemia in hypocalcemia context –Vit D deficiency")
53
Hyponatremia in Cancer Hyponatremia is the most common electrolyte disorder encountered in patients with malignancies ( 20-30%) Marker for inpatient mortality in cancer patients Can be an oncological emergency
 Marker for inpatient mortality in cancer patients Can be an oncological emergency")
54
SVC ESCC Brain Mets Cardiac Tamponade Intestinal obstruction Mechanical complications PE Esophago- bronquial fistula Central airway obstruction

55
Leukostasis DIC TLS Tumor ↑K↑K ↑P↑P ↑ Uric Acid Hypercalcemia Hyponatremia

57
Message A cancer patient can have any medical complication Many oncological emergencies can be anticipated but not necessarily prevented Be aware of the new cancer therapies being used in your hospital (discuss with your oncologists) Read the following section –NEJM Reviews (all) –Lancet Seminars (all)
 Read the following section –NEJM Reviews (all) –Lancet Seminars (all)")
58
NCI-NIH Clinical Research Center

Similar presentations
























: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")


