Download presentation
Presentation is loading. Please wait.

1
Primary hyperaldosteronism (Conn’s syndrome): An underdiagnosed disorder in both humans and cats Michiel Kerstens and Hans Kooistra
: An underdiagnosed disorder in both humans and cats Michiel Kerstens and Hans Kooistra")
3
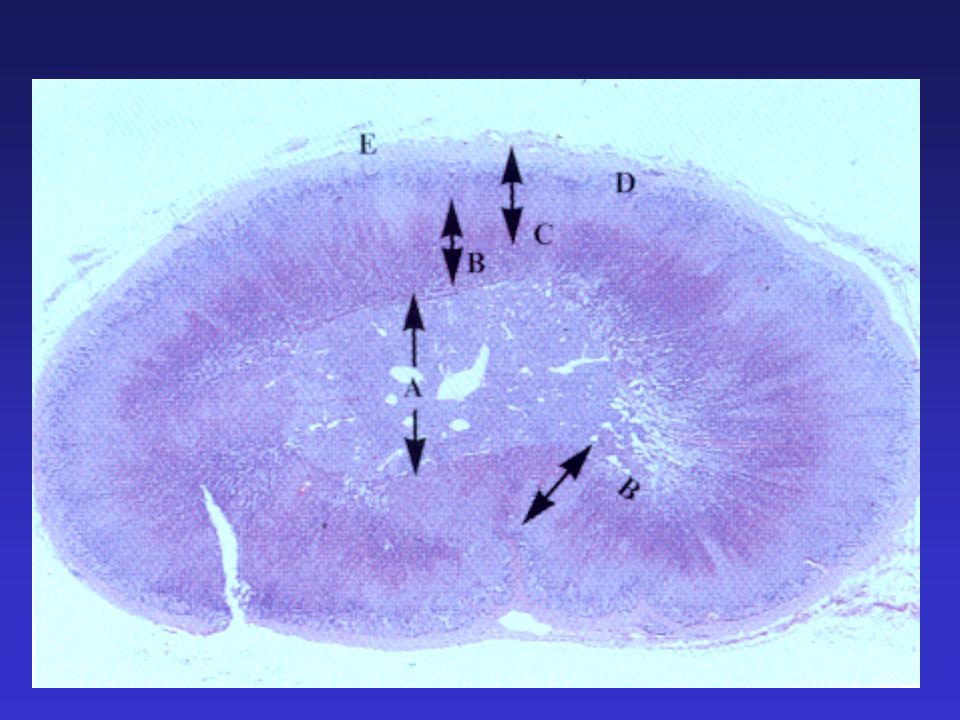
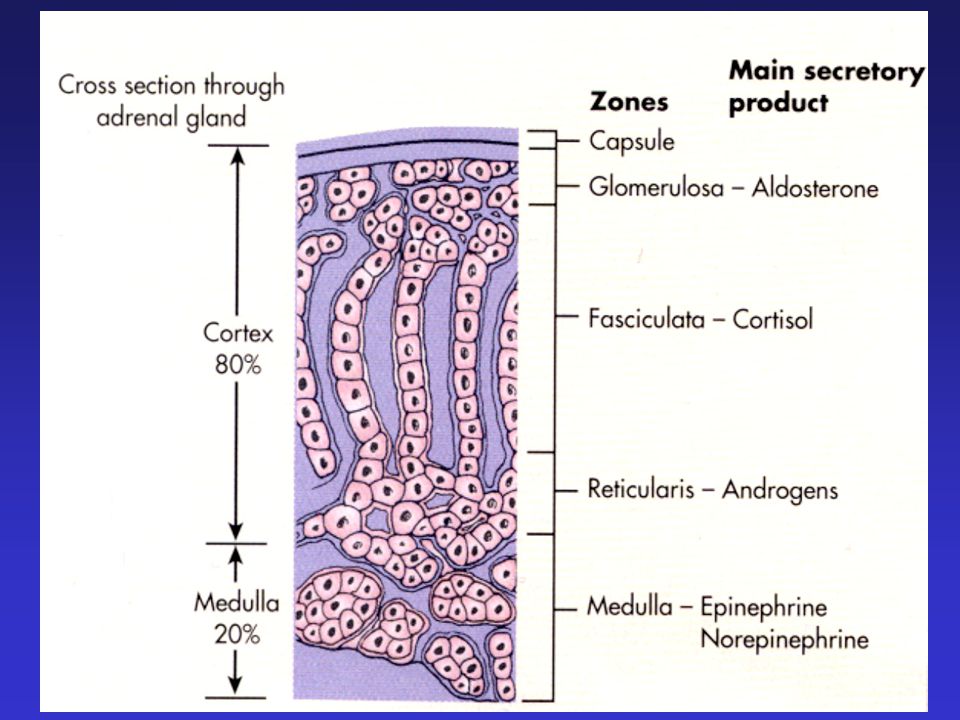
Zona Glomerulosa Zona fasiculata Zona Reticularis Adrenal gland

4
Adrenals adrenal cortex adrenal cortex mineralocorticoids: aldosterone (salt) mineralocorticoids: aldosterone (salt) glucocorticoids: cortisol (sugar) glucocorticoids: cortisol (sugar) androgens (sex) androgens (sex) adrenal medulla adrenal medulla catecholamines (adrenaline or epinephrine) catecholamines (adrenaline or epinephrine)
 mineralocorticoids: aldosterone (salt) glucocorticoids: cortisol (sugar) glucocorticoids: cortisol (sugar) androgens (sex) androgens (sex) adrenal medulla adrenal medulla catecholamines (adrenaline or epinephrine) catecholamines (adrenaline or epinephrine)")
6
Adrenocortical disorders * Adrenocortical hyper function: - mineralocorticoid excess - glucocorticoid excess - androgen excess * Adrenocortical hypo function - primary (Addison’s disease) - secondary * Non-functional adrenocortical tumors
 - secondary * Non-functional adrenocortical tumors")
7
Adrenocortical disorders * Adrenocortical hyper function: - mineralocorticoid excess = primary hyperALDOSTERONism - glucocorticoid excess - androgen excess * Adrenocortical hypo function - primary (Addison’s disease) - secondary * Non-functional adrenocortical tumors
 - secondary * Non-functional adrenocortical tumors")
8
JGC Angiotensinogen Angiotensin I Angiotensin II Renin Converting enzyme Aldosterone The Renin-Angiotensin-Aldosterone system Potassium excretion Na+ reabsorption

9
Adrenocortical disorders * Adrenocortical hyper function: - mineralocorticoid excess = primary hyperaldosteronism = Conn’s syndrome - glucocorticoid excess - androgen excess * Adrenocortical hypo function - primary (Addison’s disease) - secondary * Non-functional adrenocortical tumors
 - secondary * Non-functional adrenocortical tumors")
10
Jerome W. Conn Professor of Medicine at University of Michigan; research devoted to adaptations to tropical heat. At the Annual Meeting of the Central Society for Clinical Research (1954): “I have prepared no comprehensive review of my personal philosophy of clinical investigation. Instead, I plan to make a scientific report to you about a clinical syndrome, the investigation of which has been most exciting to me.” which has been most exciting to me.”
: I have prepared no comprehensive review of my personal philosophy of clinical investigation. Instead, I plan to make a scientific report to you about a clinical syndrome, the investigation of which has been most exciting to me. which has been most exciting to me. .")
11
Jerome W. Conn 34-year-old woman (in 1954) Since 7 years attacks of muscle spasm and muscle weakness Since 4 years: arterial hypertension (176/104 mmHg) Severe hypokalemia (K: 1.6 – 2.5 mmol/l) Slight hypernatremia (Na: 146 – 151 mmol/l) Intraperitoneal administration of urine of this women to adrenalectomized rats resulted in a 22 times greater mineralocorticoid effect than urine of healthy humans
 Since 7 years attacks of muscle spasm and muscle weakness Since 4 years: arterial hypertension (176/104 mmHg) Severe hypokalemia (K: 1.6 – 2.5 mmol/l) Slight hypernatremia (Na: 146 – 151 mmol/l) Intraperitoneal administration of urine of this women to adrenalectomized rats resulted in a 22 times greater mineralocorticoid effect than urine of healthy humans.")
12
Jerome W. Conn 34-year-old women Laparotomy: Adrenal gland tumor (right side) aldosterone-producing aldosteronoma (APA) After adrenalectomy: almost complete disappearance of signs (Hyper)Aldosteronism 20% ?? 10% ?? < 0.1% !!?? Cause of essential hypertension?
 aldosterone-producing aldosteronoma (APA) After adrenalectomy: almost complete disappearance of signs (Hyper)Aldosteronism 20% . 10% . < 0.1% !! . Cause of essential hypertension .")
13
Underdiagnosed disorder: It is there, but you have to look for it

14
Jerome W. Conn 34-year-old women Laparotomy: Adrenal gland tumor (right side) aldosterone-producing aldosteronoma (APA) After adrenalectomy: almost complete disappearance of signs (Hyper)Aldosteronism 20% ?? 10% ?? < 0.1% ?? 5-11% Cause of essential hypertension?
 aldosterone-producing aldosteronoma (APA) After adrenalectomy: almost complete disappearance of signs (Hyper)Aldosteronism 20% . 10% . < 0.1% . 5-11% Cause of essential hypertension .")
15
12-year-old castrated male shorthaired cat Emergency Not able to jumpNot able to jump Cervical ventroflexionCervical ventroflexion Falls in lateral recumbencyFalls in lateral recumbency muscle weakness hypokalemia ??? MydriasisMydriasis Blindness due to ….

16
Membrane potentials in nerve fibers and skeletal muscle fibers Na/K-ATPase:Na/K-ATPase: Membrane potential of –90 mVMembrane potential of –90 mV Action potentials:Action potentials: –Depolarization –Repolarization

17
Feline primary hyperaldosteronism clinical manifestations Plasma [K + ] ≈ 2.5 mmol/l
![Feline primary hyperaldosteronism clinical manifestations Plasma [K + ] ≈ 2.5 mmol/l](http://images.slideplayer.com/17/5306830/slides/slide_17.jpg "Feline primary hyperaldosteronism clinical manifestations Plasma [K + ] ≈ 2.5 mmol/l")
19
Afbeelding: http://www.fabcats.org

20
12-year-old castrated male shorthaired cat [K + ]1.6(3.4 – 5.2)mmol/l
![12-year-old castrated male shorthaired cat [K + ]1.6(3.4 – 5.2)mmol/l](http://images.slideplayer.com/17/5306830/slides/slide_20.jpg "12-year-old castrated male shorthaired cat [K + ]1.6(3.4 – 5.2)mmol/l")
21
[K + ] < 3.4 mmol/l K shift ECF ICF e.g. insulin therapy and alkalosis K shift ECF ICF e.g. insulin therapy and alkalosis Inadequate intake: Fasting Inadequate intake: Fasting Gastrointestinal losses: Vomiting Diarrhea Gastrointestinal losses: Vomiting Diarrhea Excessive renal losses Major causes of hypokalemia in cats
![[K + ] < 3.4 mmol/l K shift ECF ICF e.g. insulin therapy and alkalosis K shift ECF ICF e.g.](http://images.slideplayer.com/17/5306830/slides/slide_21.jpg "insulin therapy and alkalosis Inadequate intake: Fasting Inadequate intake: Fasting Gastrointestinal losses: Vomiting Diarrhea Gastrointestinal losses: Vomiting Diarrhea Excessive renal losses Major causes of hypokalemia in cats.")
22
JGC Angiotensinogen Angiotensin I Angiotensin II Renin Converting enzyme Aldosterone The Renin-Angiotensin-Aldosterone system Potassium excretion Na+ reabsorption

23
12-year-old castrated male shorthaired cat Not able to jump Cervical ventroflexion Falls in lateral recumbency hypokalemia !!! due to hyperaldosteronism??? Mydriasis Blindness due to …. arterial hypertension ???

25
12-year-old castrated male shorthaired cat Not able to jump Cervical ventroflexion Falls in lateral recumbency hypokalemia !!! due to hyperaldosteronism??? Mydriasis Blindness due to hypertension! due hyperaldosteronism???

26
JGC Angiotensinogen Angiotensin I Angiotensin II Renin Converting enzyme Aldosterone The Renin-Angiotensin-Aldosterone system Potassium excretion Na+ reabsorption

27
12-year-old castrated male shorthaired cat with arterial hypertension [K + ]1.6(3.4 – 5.2)mmol/l Aldosterone12450(60 – 630)pmol/l Renin< 20(110 – 540)fmol/l/s PAC/PRA6225(0.3 – 3.8) Primary hyperaldosteronism: renal Na + retention arterial hypertension blindness Increased renal K + excretion hypokalemia muscle weakness Metastasised malignant aldosteronoma
![12-year-old castrated male shorthaired cat with arterial hypertension [K + ]1.6(3.4 – 5.2)mmol/l Aldosterone12450(60 – 630)pmol/l Renin< 20(110 – 540)fmol/l/s PAC/PRA6225(0.3 – 3.8) Primary hyperaldosteronism: renal Na + retention arterial hypertension blindness Increased renal K + excretion hypokalemia muscle weakness Metastasised malignant aldosteronoma](http://images.slideplayer.com/17/5306830/slides/slide_27.jpg "12-year-old castrated male shorthaired cat with arterial hypertension [K + ]1.6(3.4 – 5.2)mmol/l Aldosterone12450(60 – 630)pmol/l Renin< 20(110 – 540)fmol/l/s PAC/PRA6225(0.3 – 3.8) Primary hyperaldosteronism: renal Na + retention arterial hypertension blindness Increased renal K + excretion hypokalemia muscle weakness Metastasised malignant aldosteronoma")
28
Malignant aldosteronoma

30
Underdiagnosed disorder: It is there, but you have to look for it

Similar presentations





>")




 are the triangle-shaped and orange- colored endocrine.>")




… gluconeogenesis in the liver.. Hyperglycemia… increased insulin output…>")

, Department of Surgery, Faculty of Medicine,>")


>")
