Download presentation
Presentation is loading. Please wait.

1
Mechanisms linking obesity to insulin resistance and type 2 diabetes Reporter: Wen Ying, Chen Date: 2006, 12, 28

2
Prevalence of obesity & type 2 diabetes In the United States, only about a third of adults are considered to be of “normal” weight, and similar trends are being observed worldwide. In the United States, only about a third of adults are considered to be of “normal” weight, and similar trends are being observed worldwide. At the turn of this century 171 million individuals were estimated to have diabetes, and this is expected to increase to 366 million by 2030. At the turn of this century 171 million individuals were estimated to have diabetes, and this is expected to increase to 366 million by 2030.

3
Obesity/insulin resistance Increased β-cell function Increased β-cell growth Normal glucose tolerance Compensatory hyperinsulinaemia β-cell dysfunction β-cell apoptosis Impaired glucose tolerance Type 2 diabetes

4
Obesity Insulin resistance Type 2 diabetes Dysfunction of pancreatic islet β- cells

5
Insulin resistance and obesity Fluctuations in insulin sensitivity occur during the normal life cycle Fluctuations in insulin sensitivity occur during the normal life cycle insulin resistance --------puberty, pregnancy and aging. insulin resistance --------puberty, pregnancy and aging. lifestyle variation (increased physical activity & carbohydrate intake)--------enhance insulin sensitivity. lifestyle variation (increased physical activity & carbohydrate intake)--------enhance insulin sensitivity.
 enhance insulin sensitivity. lifestyle variation (increased physical activity & carbohydrate intake) enhance insulin sensitivity..")
6
Insulin resistance and obesity The most critical factor in the emergence of metabolic diseases is obesity. The most critical factor in the emergence of metabolic diseases is obesity. adipose tissue: non-esterified fatty acids (NEFAs), glycerol, hormones (leptin & adiponectin), proinflammatory cytokines-------modulates metabolism adipose tissue: non-esterified fatty acids (NEFAs), glycerol, hormones (leptin & adiponectin), proinflammatory cytokines-------modulates metabolism
, glycerol, hormones (leptin & adiponectin), proinflammatory cytokines modulates metabolism adipose tissue: non-esterified fatty acids (NEFAs), glycerol, hormones (leptin & adiponectin), proinflammatory cytokines modulates metabolism.")
7
Insulin resistance and obesity obesity/RBP4 Retinol-binding protein-4 (RBP4) PI3-kinase in muscle phosphoenolpyruvate carboxykinase in the liver Insulin resistance
 PI3-kinase in muscle phosphoenolpyruvate carboxykinase in the liver Insulin resistance")
8
Insulin resistance and obesity obesity/adiponectin Adiponectin (an insulin sensitizer): stimulating fatty acid oxidation in an AMP-activated protein kinase (AMPK) and peroxisome proliferator activated receptor-α (PPAR-α)-dependent manner. Adiponectin (an insulin sensitizer): stimulating fatty acid oxidation in an AMP-activated protein kinase (AMPK) and peroxisome proliferator activated receptor-α (PPAR-α)-dependent manner.
: stimulating fatty acid oxidation in an AMP-activated protein kinase (AMPK) and peroxisome proliferator activated receptor-α (PPAR-α)-dependent manner..")
9
Insulin resistance and obesity obesity/TNF-α, IL-6 Upregulation of potential mediators of inflammation that can lead to insulin resistance. C-Jun amino- terminal kinase (JNK)
.")
10
Insulin resistance and obesity obesity/NEFAs The release of NEFAs (non-esterified fatty acids) may be the single most critical factor in modulating insulin sensitivity. The release of NEFAs (non-esterified fatty acids) may be the single most critical factor in modulating insulin sensitivity. 1. inhibition of pyruvate dehydrogenase, phosphofructkinase, 1. inhibition of pyruvate dehydrogenase, phosphofructkinase, hexokinase II activity. hexokinase II activity. 2. increase in the intracellular metabolism of fatty acid metabolites (DAG, fatty acyl-CoA, ceramides)-----PI(3)K 2. increase in the intracellular metabolism of fatty acid metabolites (DAG, fatty acyl-CoA, ceramides)-----PI(3)K ------downstream of insulin-receptor signalling ------downstream of insulin-receptor signalling
 may be the single most critical factor in modulating insulin sensitivity. 1. inhibition of pyruvate dehydrogenase, phosphofructkinase, 1. inhibition of pyruvate dehydrogenase, phosphofructkinase, hexokinase II activity. hexokinase II activity. 2. increase in the intracellular metabolism of fatty acid metabolites (DAG, fatty acyl-CoA, ceramides)-----PI(3)K 2. increase in the intracellular metabolism of fatty acid metabolites (DAG, fatty acyl-CoA, ceramides)-----PI(3)K downstream of insulin-receptor signalling downstream of insulin-receptor signalling.")
11
Insulin resistance and obesity obesity/distribution of body fat The distribution of body fat is itself a critical determinant of insulin sensitivity. The distribution of body fat is itself a critical determinant of insulin sensitivity. 1. intra-abdominal fat expresses more genes encoding secretory proteins and proteins responsible for energy production. 1. intra-abdominal fat expresses more genes encoding secretory proteins and proteins responsible for energy production. 2. The amount of protein released per adipocyte also differs according to their location. The secretion of adiponectin by omental adipocytes is greater than that of subcutaneous-derived adipocytes. 2. The amount of protein released per adipocyte also differs according to their location. The secretion of adiponectin by omental adipocytes is greater than that of subcutaneous-derived adipocytes.

12
β- Cell function and mass β-cell are markedly plastic in their ability to regulate insulin release. β-cell are markedly plastic in their ability to regulate insulin release. The quantity of insulin released by β-cells varies according to nature, quantity and route of administration of the stimulus, and the prevailing glucose concentration. The quantity of insulin released by β-cells varies according to nature, quantity and route of administration of the stimulus, and the prevailing glucose concentration. Insulin sensitivity also modulates β-cell function and is almost always decreased in obesity. Insulin sensitivity also modulates β-cell function and is almost always decreased in obesity. The ability of the β-cell to adapt to changes in insulin sensitivity seems to result from two parameters: the functional responsiveness of the cell and β-cell mass. The ability of the β-cell to adapt to changes in insulin sensitivity seems to result from two parameters: the functional responsiveness of the cell and β-cell mass.

13
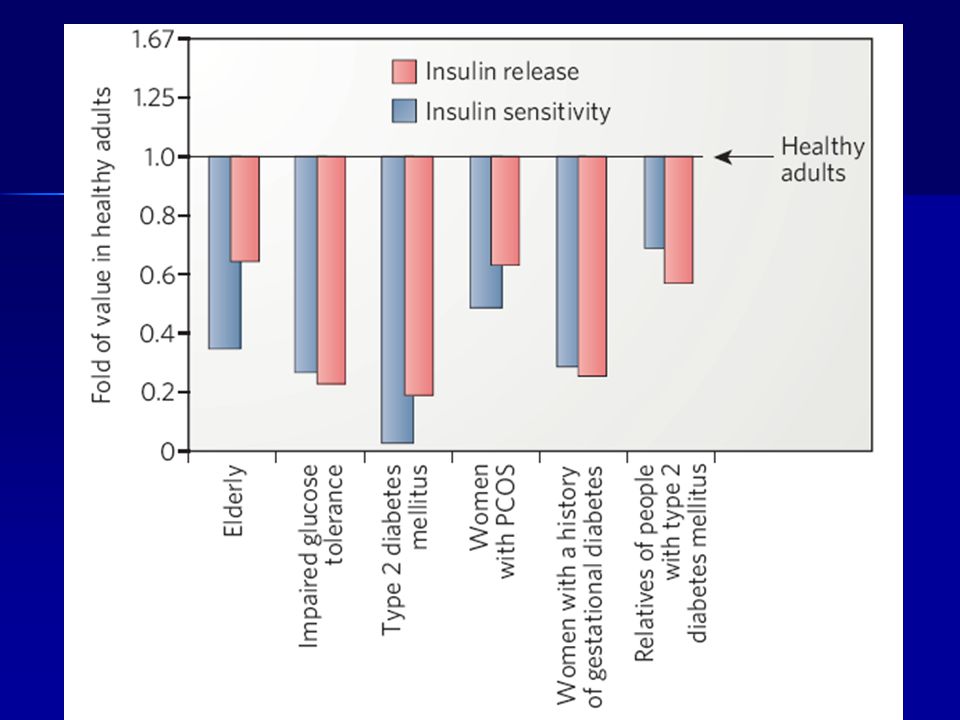
Relationship between insulin sensitivity and the β-cell insulin response in nonlinear

14
β-cell can increase insulin release to levels fourflod to fiveflod higher than in insulin- sensitive individuals, whereas β-cell In response to the insulin resistance observed in obesity, puberty and pregnancy, human β-cell can increase insulin release to levels fourflod to fiveflod higher than in insulin- sensitive individuals, whereas β-cell volume is only by about 50%.

15
β- Cell function and mass The intergration of the β- cell’s response to changes in insulin sensitivity probably involves increased cellular glucose metabolism, NEFA signalling and sensitivity to incretins. The intergration of the β- cell’s response to changes in insulin sensitivity probably involves increased cellular glucose metabolism, NEFA signalling and sensitivity to incretins. Glucose-stimulated insulin secretion Glucose-stimulated insulin secretion the metabolism of glucose ----- generation of ATP---- increase in the ATP/ADP ratio triggers the closure of the ATP-sensitive potassium (K + ATP ) channel----- depolarization of the cell membrane and influx of calcium through voltage-dependent calcium channels----- insulin granule exocytosis. the metabolism of glucose ----- generation of ATP---- increase in the ATP/ADP ratio triggers the closure of the ATP-sensitive potassium (K + ATP ) channel----- depolarization of the cell membrane and influx of calcium through voltage-dependent calcium channels----- insulin granule exocytosis.
 channel----- depolarization of the cell membrane and influx of calcium through voltage-dependent calcium channels----- insulin granule exocytosis. the metabolism of glucose generation of ATP---- increase in the ATP/ADP ratio triggers the closure of the ATP-sensitive potassium (K + ATP ) channel----- depolarization of the cell membrane and influx of calcium through voltage-dependent calcium channels----- insulin granule exocytosis..")
16
GLP-1: glucagon- like peptide-1

17
β- Cell function and mass A: increase in β- cell glucose metabolism increase in the activity of glucokinase increase in the activity of glucokinase B: anaplerosis: glucose-----pyruvate----TCA cycle ------pyruvate ------pyruvate F: humoral factor----intestinal mucosa production-- ----incretin hormons

18
β- Cell function and mass NEFAs are important for normal β- cell function. D: NEFAs + G-protein-coupled receptor GPR40 activation of intracellular signalling ----increase in the intracellular calcium -----insulin granule exocytoisis. activation of intracellular signalling ----increase in the intracellular calcium -----insulin granule exocytoisis. E: generation of fatty acyl-CoA by PKC activation----insulin granule exocytoisis. by PKC activation----insulin granule exocytoisis.

19
β- Cell function and mass G: parasympathetic stimulation acetylcholine + M2 muscarinic receptor----- insulin release acetylcholine + M2 muscarinic receptor----- insulin release H: sympathetic nervous system increased activity of the α 2-adrenergic component -----decreased insulin release increased activity of the α 2-adrenergic component -----decreased insulin release increased activity of the β -adrenergic component ----- enhances insulin output increased activity of the β -adrenergic component ----- enhances insulin output

20
β- Cell function and mass I: insulin/insulin-like growth factor 1 (IGF-1) J: incretin GLP-1 (glucagon-like peptide-1) an insulin secretagogue an insulin secretagogue increasing β –cell proliferation increasing β –cell proliferation reducing β –cell apoptosis reducing β –cell apoptosis
 J: incretin GLP-1 (glucagon-like peptide-1) an insulin secretagogue an insulin secretagogue increasing β –cell proliferation increasing β –cell proliferation reducing β –cell apoptosis reducing β –cell apoptosis")
21
β-cell dysfunction First: the β- cell is unable to release insulin rapidly in response to intravenous glucose, despite the fact that β –cells in to intravenous glucose, despite the fact that β –cells in type 2 diabetes clearly contain insulin. type 2 diabetes clearly contain insulin. Second: delivery of non-glucose secretagogues can acutely increase insulin release but dose not result in equivalent increase insulin release but dose not result in equivalent responses to those seen with similar stimulation in responses to those seen with similar stimulation in healthy subjects. healthy subjects. Third: although the number of β- cell is clearly reduced by about 50% in type 2 diabetes, this degree of β- cell about 50% in type 2 diabetes, this degree of β- cell loss cannot fully account for the change in the secretory loss cannot fully account for the change in the secretory function, because by the time the diagnostic level for function, because by the time the diagnostic level for diabetes occurs, the cell is operating at 25% or loss of its diabetes occurs, the cell is operating at 25% or loss of its functional capacity. functional capacity.

22
Type 2 diabetes is progression, and one of the main factors responsible for this is a continued decline in β –cell function Glucotoxic effects Elevated blood glucose Lipotoxic effects Elevated plasma NEFA glucolipotoxicity

23
Pathogenesis of type 2 diabetes β-cell function is decreased by about 75% when fasting hyperglycaemia is present. β-cell function is decreased by about 75% when fasting hyperglycaemia is present. Even when the glucose levels is still within the normal range, β-cell function decreases progressively as the fasting glucose level increases. Even when the glucose levels is still within the normal range, β-cell function decreases progressively as the fasting glucose level increases.

25
Genes and environment Many genes interact with the environment to produce obesity and diabetes. Many genes interact with the environment to produce obesity and diabetes. In the case of obesity/ gene mutation In the case of obesity/ gene mutation 1. melanocortin-4 receptor---most frequent mutations 1. melanocortin-4 receptor---most frequent mutations 2. leptin & leptin receptor 2. leptin & leptin receptor 3. prohormone convertase 1 (PC1) 3. prohormone convertase 1 (PC1) 4. pro-opiomelanocortin (POMC) 4. pro-opiomelanocortin (POMC) In the case of obesity/ environmental factors In the case of obesity/ environmental factors increase fat/calories & decrease physical activity ----- increase fat/calories & decrease physical activity ----- over-nutrition over-nutrition
 3. prohormone convertase 1 (PC1) 4. pro-opiomelanocortin (POMC) 4. pro-opiomelanocortin (POMC) In the case of obesity/ environmental factors In the case of obesity/ environmental factors increase fat/calories & decrease physical activity increase fat/calories & decrease physical activity over-nutrition over-nutrition.")
26
Genes and environment PC1: prohormone convertase 1 POMC: pro-opiomelanocortin MC4: melanocortin-4

27
A possible unifying mechanism Having a single mechanism to explain the link between obesity, insulin resistance and type 2 diabetes would be ideal. Having a single mechanism to explain the link between obesity, insulin resistance and type 2 diabetes would be ideal. A defect in insulin release could by the β– cell could be crucial. A defect in insulin release could by the β– cell could be crucial.

28
A possible unifying mechanism

29
Thank You!

Similar presentations
 ELISA ‘Total Amide’ ‘Active’.>")
 CARBOHYDRATE LECTURE ONE>")

![Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]](/15/4663650/big_thumb.jpg "Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]>")



 muscle proteins liver glycogen fat lipids glucose.>")








 state>")


