Download presentation
Presentation is loading. Please wait.

1
BREAST LUMPS DR AMBREEN MUNIR
FRCS, BAPRAS Fellowship Breast, PG-D Bioethics Associate Professor Surgery

2
INTRODUCTION Of all breast disorders, palpable breast lump is 2nd most common presentation, pain being the first Generally a breast lump in adolescents and young female is nearly always regarded as benign at first instance and patient may falsely be reassured with the result she refrain from further consultation

3
INTRODUCTION On the other hand, all lumps are not cancers; however the possibility of cancer must always be considered, as approximately 10% of all breast lumps are finally diagnosed as cancer.

4
Case scenario A 25 year old School teacher came to you and she is worried about a lump she just found in her right breast.

5
Additional History History of trauma Is lump painful? Nipple Discharge
Any other lump? Axilla

6
Otherwise she is healthy
Her weight is stable She is married She takes OCP Her menstrual cycle is regular No family history of cancer

7
Triple Assessment Examination Imaging Cytology/ Biopsy

8
Breast Examination Inspection- sitting position
symmetry, level of both breasts, Contour, skin changes Ask her to lift arms, put arms against waist Palpate the axilla in sitting position Palpate supraclavicular lymph nodes

9
Palpation of breast- supine position with hands above head
Examine both breasts Normal first Examine with the flat of the hand to avoid pinching up tissue

10
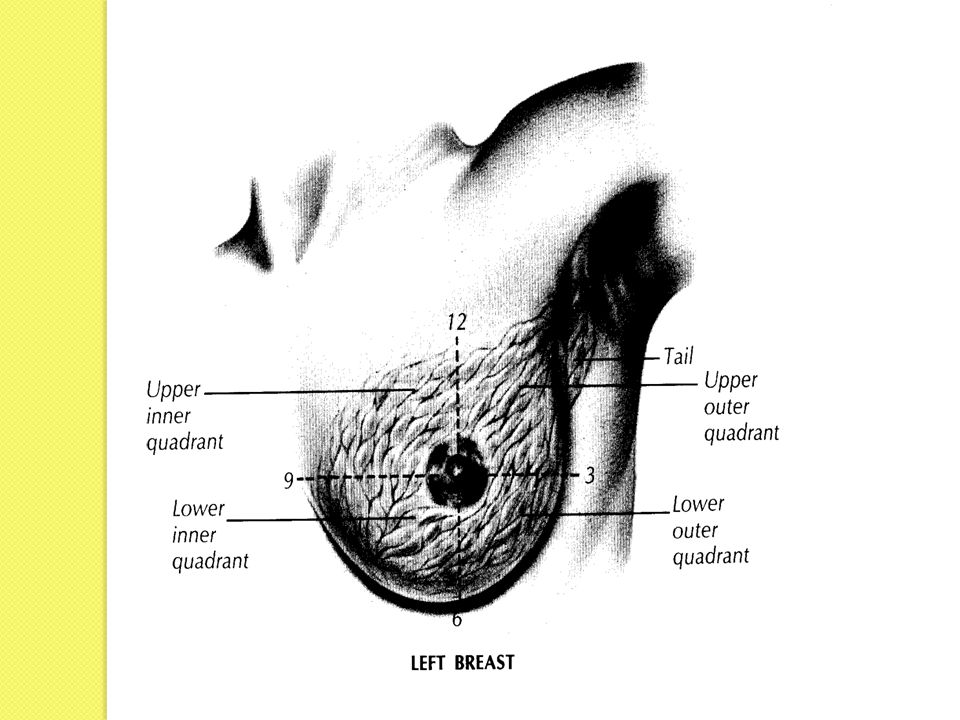
Four quadrants in clockwise direction
Nipples & areola If you have difficulty finding a discrete lump, ask the patient to demonstrate it for you

11
About Lump Site - describe the location of the lump as a position on a clockface i.e. 'A firm mass is felt at 2 o'clock'. Size Shape Surface/ Overlying skin Tenderness Consistency

12
Mobility and attachment
If you are unable to move the skin over the lump it implies fixation or tethering If patient mentioned nipple discharge ask her to squeeze nipple for a sample of the discharge

14
Examination Findings Solitary 1.5 cm mass of right breast, upper outer quadrant at 10 oclock Mass is non-tender Lesion is freely movable No obvious skin changes over the lesion No nipple discharge No axillary masses

15
Possibilities Fibroadenoma Fibrocystic disease Simple cyst
Fat necrosis Cancer

16
Benign Breast diseases
ANDI Infections Trauma

17
Fibroadenoma Benign overgrowth of one lobule of the breast, usually isolated, may be multiple or giant Composed of both stromal and epithelial elements in the breast Well-defined, mobile, painless, discrete Common in younger women, and is most common tumor in women younger than age 30 years

18
Fibrocystic disease Combination of localized fibrosis, inflammation, cyst formation and hormone driven breast pain Occurs almost exclusively between menarche and menopause Causing cyclical pain and swelling, lumpy breasts, multiple breast cysts

19
Cysts Fluid-filled, epithelium-lined cavities often associated with FBD Common after age 35, and rare before 25 Round symmetrical lumps, may be discrete or multiple, occasionally painful Three types Simple cyst, clear or green fluid and is benign. Milk-filled cyst, called galactocele and is benign. Bloody cyst is a cause of concern for malignancy.

20
Infections & Inflammations
Lactational Mastitis Due to acute staphylococcal infection of mammary ducts Breast Abscess When infection progress

21
Infections & Inflammations
Mammary duct ectasia Due to dilated, scarred, chronically inflammed subareolar mammary ducts Recurrent yellow green nipple discharge or recurrent breast abscess Mondor’s disease Phlebitis of the thoracoepigastric vein Palpable, visible, tender cord along lower quadrants

22
Fat Necrosis Associated with trauma or radiation therapy to breast
There is organization of acute traumatic injury by fibrosis, organized haematoma & occasionally calcification Can simulate cancer with mass or skin retraction

23
Next step in assessment
Imaging- choice of imaging modality depends on specific characteristics of the patient e.g. age, and findings on clinical examination Ultrasound scan or Mammography MRI of breast

24
Indications of U/S To evaluate the breast in patients who are under the age of 35 years To differentiate solid and cystic lesions Women who are pregnant and cannot have mammography To complement mammography To guide fine needle aspiration and core biopsies

25
Next step in this case

26
Solid lesions- have internal echoes
Benign tumours have isoechoic or hypoechoic patterns, smooth well defined borders Malignant tumours have hypoechoic areas,interspersed between brighter echoes, irregular edges Cysts- Smooth walls, sharp anterior and posterior borders, black hypoechoic centres without internal echoes

27
U/S report in this case is benign solid lesion U2

28
To complete the triple assessment, this lesion needs to be biopsied
There are a number of different types of biopsy( cytological or histopathological)
")
29
Fine needle aspiration (FNA)
")
30
Core biopsy

31
FNA-Sensitivity is 80-98%, specificity 100%
False negatives are 2-10% Core Biopsy-More tissue, however still possibility of false negative and could represent sampling error Incisional biopsy- For large (>4 cm) lesions for whom pre-op chemotherapy or radiation will be desirable Excisional biopsy-Removal of entire lesion and a margin of normal breast parenchyma
 lesions for whom pre-op chemotherapy or radiation will be desirable. Excisional biopsy-Removal of entire lesion and a margin of normal breast parenchyma.")
32
Triple Assessment gives confident diagnosis in 95% of cases
On other hand, Triple assessment is not always needed to investigate breast lumps, as it would be viable to diagnose a breast cyst purely on ultrasound A solid lump will require a core biopsy to confirm its benign or malignant state

33
Treatment Most benign breast lumps will not require treatment. This is especially true of small fibroadenomas,If they are increasing in size they may be removed FNA is used for simple and recurrent cysts. In this case FNA would be used as a treatment rather than a diagnostic tool. Complete resolution, follow up to ensure it does not recur,Incomplete resolution treat as breast mass and excise

34
Treatment Mondor’s disease
Treatment self-limited, can use NSAIDs if necessary Antibiotics can be used to treat infections of the breast and abscesses are treated by incision & drainage

35
Treatment Mondor’s disease
Treatment self-limited, can use NSAIDs if necessary Antibiotics can be used to treat infections of the breast and abscesses are treated by incision & drainage

36
BREAST CANCER DR AMBREEN MUNIR
FRCS, BAPRAS Fellowship Breast, PG Diploma Bioethics Associate Professor Surgery

37
Overview The most common form of cancer among women
The second most common cause of cancer related mortality One out of nine Pakistani women is likely to suffer from Breast Cancer at some point of life

38
Overview Highest incidence of Breast cancer in the Asia
At Least 90,000 Women Suffer From Breast Cancer In Pakistan Every Year 40,000 Deaths Per Year, Which Is Alarming

39
Risk factors Female Aging First degree Relative Menstrual history
early onset late menopause Child birth After the age of 30

40
Risk Factors Hormonal replacement therapy(HRT)
30% increased risk with long term use Oral Contraceptives(OC) risk slight risk returns to normal once the use of OC’s has been discontinued Radiation exposure
 risk slight. risk returns to normal once the use of OC’s has been discontinued. Radiation exposure.")
41
Risk Factors Breast disease Atpyical Hyperplasia
Intraductal carcinoma in situ Intralobular carcinoma in situ Obesity Diet Fat Alcohol

42
Genetic Risk Factors BRCA-1 BRCA-2 P53 Her-2/neu

43
Because of enhanced Public awareness, number of patients reporting with complaints of breast diseases has increased in recent years

44
Breast diseases are common in females because of more complex structure of female breast, greater volume and influence of various hormones Subjected to constant physiological changes throughout reproductive life and beyond. These changes lead to a number of conditions

45
Mostly these conditions are benign e. g
Mostly these conditions are benign e.g. bilateral nodularity, tender lumpy breasts Our aim should be to exclude cancer That aim is achieved through proper assessment

46
Triple Assessment Clinical History Examination Imaging Ultrasound
Mammography Histopathology FNAC Trucut Biopsy

47
History Age Family history of breast and other cancers with emphasis on gynaecological cancers

48
History Reproductive history age at menarche age at first delivery
number of pregnancies, children and miscarriages age at onset of menopause history of hormonal use including: contraceptive pills (type and duration) hormonal replacement therapy (type and duration)
 hormonal replacement therapy (type and duration)")
49
Signs/Symptoms Any new discrete breast lump
Any new lump in a pre-existing nodularity Recurrent breast cysts Unilateral axillary lump Unusual increase in the size of one breast

50
Signs/Symptoms Persistent or unilateral breast pain
Pain associated with a lump

51
Signs/Symptoms Nipple discharge other than breast milk Blood stained
Single duct Bilateral troublesome discharge in more than 50 years New nipple retraction Nipple eczema if not elsewhere or unresponsive to steroids

52
Signs/Symptoms A puckering of skin of breast
Skin irritation or dimpling Redness, scaling or thickening of skin of breast Swelling of arm

54
Clinical Examination Annually for women over 40
At least every 3 years for women between 20 and 40 More frequent examination for high risk patients

55
Clinical examination Breast Sitting Supine
Both Axillae & Supraclavicular fossae Local examination of possible metastatic sites

57
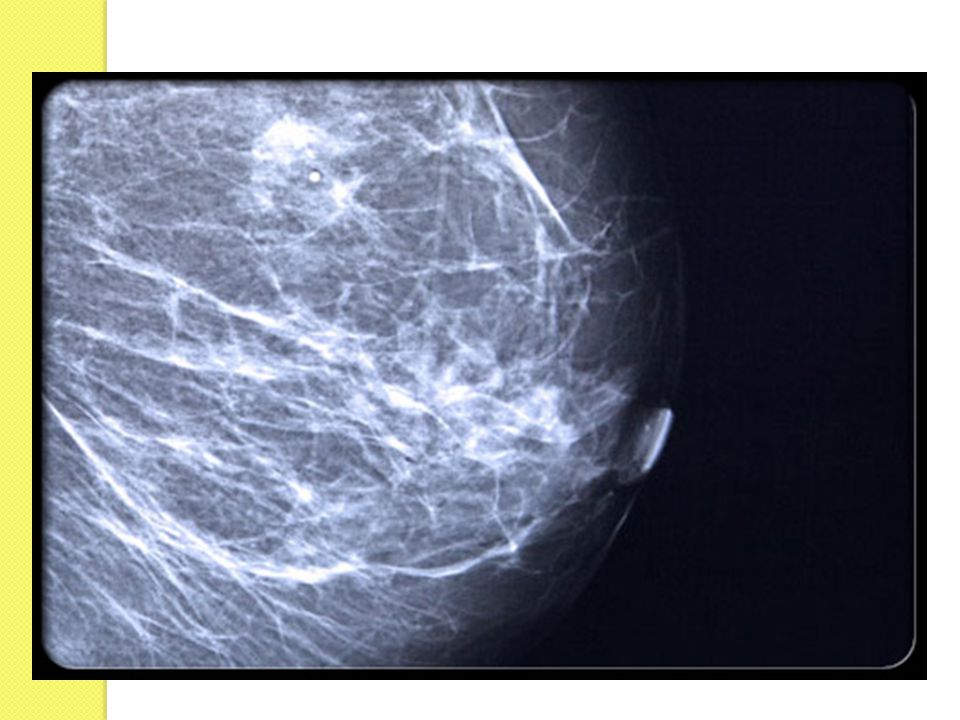
Mammography Not recommended under the age of 35 unless there is a strong clinical suspicion of cancer Mammography allows for efficient diagnosis of breast cancers at an earlier stage Normal mammogram does not rule out possibility of cancer completely

58
Mammogram Two of the most important mammographic indicators of breast cancers Masses Microcalcifications: Tiny flecks of calcium – like grains of salt – in the soft tissue of the breast that can sometimes indicate an early cancer.

59
Malignant masses have a more spiculated appearance

63
Calcifications show up as white spots on a mammogram
Round well-defined, larger calcifications are more likely benign Tight cluster of tiny, irregularly shaped calcifications may indicate cancer

65
Breast Ultrasound To see whether the lump is solid or cystic
Margins, complexity For aspiration or biopsy

66
Histopathology Fine needle aspiration cytology
performed with 5 cc disposable needle as outpatient procedure Trucut biopsy performed with core cut needle under local anaesthesia

67
Treatment Based on many factors
Varies from reassurance to radical Surgery

68
TNM Staging TX: primary tumor cannot be assessed
T0: no evidence of tumor Tis: carcinoma in situ T1: tumor <2 cm T2: tumor 2-5 cm T3: tumor >5 cm T4: direct extension to chest wall or skin

69
TNM staging NX:regional nodes cannot be assessed
N0: negative lymph nodes N1: metastases to moveable ipsilateral axillary lymph nodes N2: metastases to fixed ipsilateral N3: metastases to ipsilateral internal mammary nodes

70
TNM staging MX: distant sites cannot be assessed
M0: no distant metastases M1: distant metastases

71
Breast cancer treatment
Breast Conserving surgery Mastectomy Axillary sampling( Sentinel node biopsy) Axillary clearance Chemotherapy Radiotherapy Hormone Therapy
 Axillary clearance. Chemotherapy. Radiotherapy. Hormone Therapy.")
72
Oncoplastic Surgery The combination of reconstructive surgery in cancer surgery. Immediate breast reconstruction following partial or total Mastectomy

73
Oncoplastic Tumours smaller than 3 cm Nodal status-N0, N1
Peripheral tumors Large breasts

74
Conclusion The diagnosis of breast cancer is devastating for most women and is compounded by mental anguish associated with the anticipated changes in their appearance

75
Conclusion As clinical breast examination (CBE) may play a positive role in detecting cancer earlier, especially in reducing tumour size from 5 cm to 2 cm at presentation in developing countries without a mammography screening programme, the practice of CBE by doctors and trained nurses should be encouraged.
 may play a positive role in detecting cancer earlier, especially in reducing tumour size from 5 cm to 2 cm at presentation in developing countries without a mammography screening programme, the practice of CBE by doctors and trained nurses should be encouraged.")
76
Conclusion If breast cancer patients are offered breast oncoplasty procedures, more women are likely to come forward for treatment at an early stage.

Similar presentations