Download presentation
Presentation is loading. Please wait.

1
Rheumatology Board Review Presentation-1
Vikas Majithia

2
Guarantees If you listen and remember today:
>80% of Q of rheum in board >90% correct (Backed By Dinner at CHAR) - Something special
 - Something special.")
3
Game-Plan Stimulate your mind and think with me Highlight the topics
Go over “educational objectives” These are potential questions/test pertinent areas Participate If you want write, Use the handout from today otherwise just listen I can not teach you anything but I can help you think/learn

4
Questions – Technique to Decipher
OBJECTIVE 1 STEP 2 STEP WHAT YOU SEE IS WHAT YOU GET NO AMBIGUITY SPECIFIC INFORMATION IN VIGNETTE LIKELY ANSWERS (Confounding) OVERVIEW/REVIEW
 OVERVIEW/REVIEW.")
5
Q A 46-year-old man is evaluated because of acute pain and swelling in his right knee. He was recently diagnosed with hypertension and started on hydrochlorothiazide, 25 mg/d. He smokes 1 pack of cigarettes daily, and consumes 6 to 12 cans of beer on the weekends. On physical examination, he weighs kg (220 lb). His temperature is °F, pulse rate is 90/min, and blood pressure is 180/90 mm Hg. There is effusion of the knee along with surrounding redness and it is exquisitely tender. He has no other systemic findings. An arthrocentesis resulted in 30 cc of cloudy fluid. Preliminary report shows needle shaped crystals which are yellow when parallel to polarizer and a negative gram stain. What is the next best step in the management of his condition? Treat him with Allopurinol 300 mg/day. Treat him with oral erythromycin 375 mg BID. Treat him with a combination of colchicine and naproxen. Do nothing as you have done a therapeutic arthrocentesis. Order an MRI of the knee to rule out meniscal tear
. His temperature is °F, pulse rate is 90/min, and blood pressure is 180/90 mm Hg. There is effusion of the knee along with surrounding redness and it is exquisitely tender. He has no other systemic findings. An arthrocentesis resulted in 30 cc of cloudy fluid. Preliminary report shows needle shaped crystals which are yellow when parallel to polarizer and a negative gram stain. What is the next best step in the management of his condition Treat him with Allopurinol 300 mg/day. Treat him with oral erythromycin 375 mg BID. Treat him with a combination of colchicine and naproxen. Do nothing as you have done a therapeutic arthrocentesis. Order an MRI of the knee to rule out meniscal tear.")
6
Q A 46-year-old man is evaluated because of acute pain and swelling in his right knee. He was recently diagnosed with hypertension and started on hydrochlorothiazide, 25 mg/d. He smokes 1 pack of cigarettes daily, and consumes 6 to 12 cans of beer on the weekends. On physical examination, he weighs kg (220 lb). His temperature is °F, pulse rate is 90/min, and blood pressure is 180/90 mm Hg. There is effusion of the knee along with surrounding redness and it is exquisitely tender. He has no other systemic findings. An arthrocentesis resulted in 30 cc of cloudy fluid. Preliminary report shows intracellular needle shaped crystals which are yellow when parallel to polarizer and a negative gram stain. What is the next best step in the management of his condition? Treat him with Allopurinol 300 mg/day. Treat him with oral erythromycin 375 mg BID. Treat him with a combination of colchicine and naproxen. Do nothing as you have done a therapeutic arthrocentesis. Order an MRI of the knee to rule out meniscal tear
. His temperature is °F, pulse rate is 90/min, and blood pressure is 180/90 mm Hg. There is effusion of the knee along with surrounding redness and it is exquisitely tender. He has no other systemic findings. An arthrocentesis resulted in 30 cc of cloudy fluid. Preliminary report shows intracellular needle shaped crystals which are yellow when parallel to polarizer and a negative gram stain. What is the next best step in the management of his condition Treat him with Allopurinol 300 mg/day. Treat him with oral erythromycin 375 mg BID. Treat him with a combination of colchicine and naproxen. Do nothing as you have done a therapeutic arthrocentesis. Order an MRI of the knee to rule out meniscal tear.")
7
Rheumatoid Arthritis Epidemiology
Etiology: Role of genetic and environmental factors (HLA-DR4). Pathology: Role of inflammation, cytokines, cells and histopathology. Pathogenesis: Molecular mimicry, Role of infections. Clinical Manifestations: Articular and extra- articular involvement, Pattern of involvement. Laboratory Findings: routine laboratory changes, inflammatory markers, rheumatoid factor and anti-CCP antibody. Radiographic Evaluation: Findings. Clinical course and prognosis: course, disability, chronicity, effect on lifestyle, risk for family members.
. Pathology: Role of inflammation, cytokines, cells and histopathology. Pathogenesis: Molecular mimicry, Role of infections. Clinical Manifestations: Articular and extra- articular involvement, Pattern of involvement. Laboratory Findings: routine laboratory changes, inflammatory markers, rheumatoid factor and anti-CCP antibody. Radiographic Evaluation: Findings. Clinical course and prognosis: course, disability, chronicity, effect on lifestyle, risk for family members.")
8
Rheumatoid Arthritis Diagnosis: Mostly Clinical, Classification criteria helpful Morning stiffness (at least 1 hour) Arthritis of three or more joint areas Arthritis of hand joints (PIP and MCP) Symmetric arthritis, by area Subcutaneous rheumatoid nodules Positive test for rheumatoid factor Radiographic changes (hand and wrist radiography that show erosion of joints or unequivocal demineralization around joints) (First Three need to be present at least for 6 weeks) RF: May be negative in up to 1/4 patients Anti-Cyclic citrullinated peptide (anti-CCP) antibody- specific not very sensitive
 Symmetric arthritis, by area. Subcutaneous rheumatoid nodules. Positive test for rheumatoid factor. Radiographic changes (hand and wrist radiography that show erosion of joints or unequivocal demineralization around joints) (First Three need to be present at least for 6 weeks) RF: May be negative in up to 1/4 patients. Anti-Cyclic citrullinated peptide (anti-CCP) antibody- specific not very sensitive.")
9
Rheumatoid Arthritis Long term risk of CAD Clinical picture:
Articular disease- Persistent symptoms with significant morning stiffness Involvement of hands and feet (MCP, MTP, PIP) & sparing of DIP Cervical spine disease- risk of subluxation and myelopathy Extra-Articular disease Rheumatoid nodules Vasculitis Pulmonary involvement: Effusion (low glucose) and Fibrosis Felty’s syndrome: RA, Neutropenia and splenomegaly Eye involvement- Scleritis and episcleritis (not uveitis) Laboratory abnormalities Rheumatoid factor- negative in 25% cases Anti-CCP antibody- specific not very sensitive Elevated ESR and CRP Bony erosions Long term risk of CAD
 & sparing of DIP. Cervical spine disease- risk of subluxation and myelopathy. Extra-Articular disease. Rheumatoid nodules. Vasculitis. Pulmonary involvement: Effusion (low glucose) and Fibrosis. Felty’s syndrome: RA, Neutropenia and splenomegaly. Eye involvement- Scleritis and episcleritis (not uveitis) Laboratory abnormalities. Rheumatoid factor- negative in 25% cases. Anti-CCP antibody- specific not very sensitive. Elevated ESR and CRP. Bony erosions. Long term risk of CAD.")
10
©Copyright Science Press Internet Services

12
Rheumatoid Arthritis Management:
NSAIDs: Non-selective & Cox-2 inhibitors (do not prevent joint damage) DMARDs Antimalarials: Hydroxychloroquine and chloroquine and Sulfasalazine - use in mild, non erosive disease Steroids: Low dose, Short term therapy for major flares, Bridge therapy, Vasculitis and Intra-articular injection Methotrexate: Preferred initial DMARD, Use of folate replacement, risk of hepatitis, pneumonitis and cytopenia Leflunomide: As effective as MTX, 2nd line due to cost, No lung toxicity, risk of hepatitis, Category X in pregnancy. Others — Azathioprine, Gold, D-penicillamine, cyclosporine
 DMARDs. Antimalarials: Hydroxychloroquine and chloroquine and Sulfasalazine - use in mild, non erosive disease. Steroids: Low dose, Short term therapy for major flares, Bridge therapy, Vasculitis and Intra-articular injection. Methotrexate: Preferred initial DMARD, Use of folate replacement, risk of hepatitis, pneumonitis and cytopenia. Leflunomide: As effective as MTX, 2nd line due to cost, No lung toxicity, risk of hepatitis, Category X in pregnancy. Others — Azathioprine, Gold, D-penicillamine, cyclosporine.")
13
Rheumatoid Arthritis Management: BIOLOGICs
TNF blockers- Etanercept, Infliximab, Adalimumab, Certolizumab pegol, Golimumab B cell modulator: Rituximab Co-stimulator blocker: Abatacept (Orencia) IL-6 blocker- Tocilizumab (Actemra) IL-1 blocker- Anakinra JAK inhibitor- Tofacitinib Activation of latent TB Increased risk of other infections Possible increased risk of Malignancy, demyelinating disease or other autoimmune diseases, Lipid/Liver monitoring with Il-6 blocker
 IL-6 blocker- Tocilizumab (Actemra) IL-1 blocker- Anakinra. JAK inhibitor- Tofacitinib. Activation of latent TB. Increased risk of other infections. Possible increased risk of Malignancy, demyelinating disease or other autoimmune diseases, Lipid/Liver monitoring with Il-6 blocker.")
14
DMARD Dosage Onset of Effect Adverse Events Monitoring Auranofin (Ridaura) 3-6 mg QD 4-6 months Diarrhea CBC, urinalysis (u/a) every 3 months Azathioprine (Imuran) mg QD 2-3 months GI intolerance, cytopenia, hepatitis infections, CBC, LFTs every 2-4 weeks initially, then every 2-3 months Cyclosporine (Gengraf, Neoral, generic) 2.5-5 mg QD GI intolerance, cytopenia, infections, hypertension, renal disease Creatinine (Cr) every two weeks until dose is stable, then monthly; consider CBC, LFTs, and K+ level tests D-Penicillamine (Cuprimine) mg QD 3-6 months GI intolerance, skin rash, proteinuria, Rare: cytopenia CBC- u/a every 2 weeks until dose is stable, then every 2-3 months Hydroxychloroquine (Plaquenil) mg QD 2-6 months GI intolerance, Retinal toxicity Eye examinations every 12 months IM Gold sodium thiomalate (Myochrysine) Aurothioglucose (Solganal) 25-50 mg IM every 2-4 weeks 6-8 weeks GI intolerance, skin rash, oral ulcers, proteinuria, cytopenia, CBC and u/a every 2 weeks until dose is stable, then with each injection Leflunomide (Arava) 20 mg QD 4-12 weeks GI intolerance, skin rash, hepatitis, cytopenia, highly teratogenic Hepatitis B and C serology in high-risk patients; CBC, Cr and LFTs monthly for 6 months, then 1-2 months; adjust dose or stop if LFTs elevated Methotrexate 15-25 mg orally, sc or IM every week 1-2 months GI intolerance, oral ulcers, alopecia, hepatitis, pneumonitis, cytopenia, rash, teratogenic CBC, Cr and LFTs monthly for 6 months, then every 1-2 months; adjust dose or stop if LFTs elevated Minocycline (Minocin) 100 mg BID 1-3 months Dizziness, skin pigmentation none Sulfasalazine (Azulfidine) 2-3 gm/day GI intolerance, oral ulcers, cytopenia, rash CBC every 2-3 months
 every 3 months. Azathioprine (Imuran) mg QD. 2-3 months. GI intolerance, cytopenia, hepatitis infections, CBC, LFTs every 2-4 weeks initially, then every 2-3 months. Cyclosporine (Gengraf, Neoral, generic) mg QD. GI intolerance, cytopenia, infections, hypertension, renal disease. Creatinine (Cr) every two weeks until dose is stable, then monthly; consider CBC, LFTs, and K+ level tests. D-Penicillamine. (Cuprimine) mg QD. 3-6 months. GI intolerance, skin rash, proteinuria, Rare: cytopenia. CBC- u/a every 2 weeks until dose is stable, then every 2-3 months. Hydroxychloroquine. (Plaquenil) mg QD. 2-6 months. GI intolerance, Retinal toxicity. Eye examinations every 12 months. IM Gold sodium thiomalate. (Myochrysine) Aurothioglucose. (Solganal) mg IM every 2-4 weeks. 6-8 weeks. GI intolerance, skin rash, oral ulcers, proteinuria, cytopenia, CBC and u/a every 2 weeks until dose is stable, then with each injection. Leflunomide (Arava) 20 mg QD weeks. GI intolerance, skin rash, hepatitis, cytopenia, highly teratogenic. Hepatitis B and C serology in high-risk patients; CBC, Cr and LFTs monthly for 6 months, then 1-2 months; adjust dose or stop if LFTs elevated. Methotrexate mg orally, sc or IM every week. 1-2 months. GI intolerance, oral ulcers, alopecia, hepatitis, pneumonitis, cytopenia, rash, teratogenic. CBC, Cr and LFTs monthly for 6 months, then every 1-2 months; adjust dose or stop if LFTs elevated. Minocycline (Minocin) 100 mg BID. 1-3 months. Dizziness, skin pigmentation. none. Sulfasalazine (Azulfidine) 2-3 gm/day. GI intolerance, oral ulcers, cytopenia, rash. CBC every 2-3 months.")
15
Biologic Drugs Dosage Onset of Effect Adverse Events Monitoring TNF Blockers Adalimumab (Humira) 40 mg sc EOW 2-12 weeks Injection site reaction (ISR), infection risk, TB reactivation Rare: demyelinating disorders Monitor for TB, fungal and other infections; CBC and Liver panel (LFTs) at baseline and monthly; thereafter every 2-3 months Etanercept (Enbrel) 25 mg sc twice/ week or 50 mg sc weekly ISR, infection risk, TB reactivation LFTs at baseline and monthly; thereafter every 2-3 months. Certolizumab- Cimzia 200/400 mg sc EOW/monthly Golumimab (Simponi) 50 mg sc monthly Infliximab (Remicade) 3 mg/kg at weeks 0, 2 and 4 weeks, then every 8 weeks Infusion reactions, infection risk, TB reactivation Monitor-TB, fungal and other infections; CBC, Cr and LFTs at baseline and monthly; thereafter every 2-3 months.
, infection risk, TB reactivation. Rare: demyelinating disorders. Monitor for TB, fungal and other infections; CBC and. Liver panel (LFTs) at baseline and monthly; thereafter every 2-3 months. Etanercept (Enbrel) 25 mg sc twice/ week or 50 mg sc weekly. ISR, infection risk, TB reactivation. LFTs at baseline and monthly; thereafter every 2-3 months. Certolizumab- Cimzia. 200/400 mg sc EOW/monthly. Golumimab (Simponi) 50 mg sc monthly. Infliximab (Remicade) 3 mg/kg at weeks 0, 2 and 4 weeks, then every 8 weeks. Infusion reactions, infection risk, TB reactivation. Monitor-TB, fungal and other infections; CBC, Cr and LFTs at baseline and monthly; thereafter every 2-3 months.")
16
Drug Dosage Onset of Effect Adverse Events Monitoring Other Biologics Anakinra (Kineret) – IL -1 blocker 100 mg sc QD 4-12 weeks ISR, leucopenia, Infections, Hypersensitivity CBC at baseline and every 3 months Abatacept(Orencia) – CTLA 4 Ig, Costimulator blockade mg (weight based) at 0, 2 and 4 weeks then every 4 weeks 2-12 weeks Infusion reactions, infection risk, sepsis, hypersensitivity, COPD exacerbation Monitor for TB, other infections; CBC and chemistry and LFTs at baseline and with each infusion Rituximab (Rituxan)- B-cell inhibitor 1000 mg at 0 and 15 days Infusion reactions, infection risk, reactivation and new viral infections, respiratory difficulty, cytopenia Monitor for TB, other infections; CBC and chemistry and LFTs at baseline and 2 weeks; thereafter every 2-3 months Tocilizumab (Actemra)- IL-6 blocker 4 mg/kg or 8 mg/kg (weight based) every 4 weeks Infusion reactions, infection risk, sepsis, cytopenia, hepatitis, hypersensitivity, Lipid abnormalities, GI perforation Tofacitinib (XelJanz) – JAK Kinase inhibitor Oral daily- 5 mg or 10 mg BID 8-12 weeks Infection risk, sepsis, cytopenias, hepatitis, hypersensitivity, GI perforation Monitor for TB, other infections; CBC and chemistry and LFTs at baseline and periodically.
 – CTLA 4 Ig, Costimulator blockade mg (weight based) at 0, 2 and 4 weeks then every 4 weeks weeks. Infusion reactions, infection risk, sepsis, hypersensitivity, COPD exacerbation. Monitor for TB, other infections; CBC and chemistry and LFTs at baseline and with each infusion. Rituximab (Rituxan)- B-cell inhibitor mg at 0 and 15 days. Infusion reactions, infection risk, reactivation and new viral infections, respiratory difficulty, cytopenia. Monitor for TB, other infections; CBC and chemistry and LFTs at baseline and 2 weeks; thereafter every 2-3 months. Tocilizumab (Actemra)- IL-6 blocker. 4 mg/kg or 8 mg/kg (weight based) every 4 weeks. Infusion reactions, infection risk, sepsis, cytopenia, hepatitis, hypersensitivity, Lipid abnormalities, GI perforation. Tofacitinib (XelJanz) – JAK Kinase inhibitor. Oral daily- 5 mg or 10 mg BID weeks. Infection risk, sepsis, cytopenias, hepatitis, hypersensitivity, GI perforation. Monitor for TB, other infections; CBC and chemistry and LFTs at baseline and periodically.")
17
Rheumatoid Arthritis Questions asked
1. Patient scenario: middle aged female, outpatient 2. Comes with polyarthritis, failed NSAIDs. What to do next? 3. Inadequate response to MTX/plaquenil 4. What test to do before starting a biologic agent 5. Patient on MTX comes with cough. What to do next? 6. RA Patient (on/not on) MTX/biologic agent comes with single joint pain/swelling. What to do next?
 MTX/biologic agent comes with single joint pain/swelling. What to do next")
18
Rheumatoid Arthritis Questions asked
7. Patient on leflunomide. Wants to become pregnant. 8. RA Patient on MTX/biologic agent comes with cough, weight loss. What to do next? 9. RA Patient has unilateral calf swelling? Likely diagnosis 10. RA patient going for surgery? What test to do? 11. RA patient with paraesthesia, dizziness. What test to do? 12. RA patient with replaced hip/knee? Come with pain in the prosthetic joint. What to do next?

19
Rheumatoid Arthritis Questions asked
13. RA patient on plaquenil, presents with blurred vision. Likely cause: retinal toxicity. 14. Long-standing RA Patient on treatment presents with fever, weight loss, SOB, distended neck veins. What to do next? 15. Long-standing RA Patient on treatment presents with intermittent fever, weight loss, diarrhoea, What to do next? 16. Long-standing RA Patient on treatment presents with fever, weight loss, skin ulcers, foot drop. What to do next? 17. RA patient on MTX asks risk of liver toxicity and monitoring 18. Patient with intermittent migratory pain swelling. Likely diagnosis? 19. long-standing RA Patient with early satiety, weight loss, skin ulcers, LUQ fullness. What to do next? 20. Young male patient with fever, evanescent rash, sore throat, arthralgia, lymphadenopathy and hepatosplenomegaly. Typically –ve RF

20
Q A 52-year-old woman who has had rheumatoid arthritis for two years comes to your office for a scheduled health evaluation. She reports that she feels well and has minimal morning stiffness. Current medications are leflunomide, 20 mg daily, and ibandronate 150 mg monthly. Physical examination reveals swelling of the second and fifth right MCPs and the third left MCP; and swelling of the first and fourth right PIPs and the second left PIP with minimal tenderness. The right wrist and left knee are slightly swollen, and range of motion (ROM) is slightly painful. Tenderness to palpation of the MTPs is noted. Radiographs of the feet obtained one year ago show erosions of the fourth and fifth right MTPs and the fourth left MTP. Laboratory studies: Hematocrit 11.1% , Hemoglobin 33 g/dL, Erythrocyte sedimentation rate 31 mm/hr, Liver function tests Normal, Disease activity score shows moderate activity. Which of the following is the appropriate management at this time? (A) No further change in therapy (B) Add etanercept, 50 mg weekly (C) Add prednisone, 10 mg daily (D) Add hydroxychloroquine, 200 mg daily (E) Discontinue leflunomide; add methotrexate, 20 mg weekly
 is slightly painful. Tenderness to palpation of the MTPs is noted. Radiographs of the feet obtained one year ago show erosions of the fourth and fifth right MTPs and the fourth left MTP. Laboratory studies: Hematocrit 11.1% , Hemoglobin 33 g/dL, Erythrocyte sedimentation rate 31 mm/hr, Liver function tests Normal, Disease activity score shows moderate activity. Which of the following is the appropriate management at this time (A) No further change in therapy. (B) Add etanercept, 50 mg weekly. (C) Add prednisone, 10 mg daily. (D) Add hydroxychloroquine, 200 mg daily. (E) Discontinue leflunomide; add methotrexate, 20 mg weekly.")
21
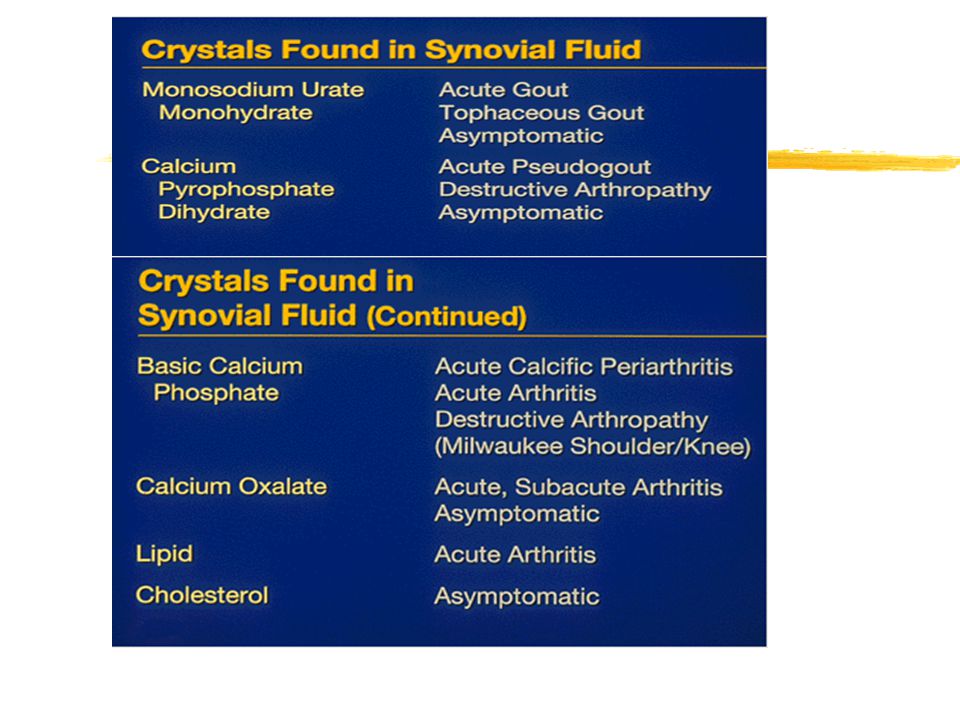
Crystal Induced Arthritis
Epidemiology Crystals: Gout (monosodium urate), Psudogout (Ca pyrophosphate), Basic calcium phosphate Etiology: Role of metabolic factors (overproduction or underexcretion of uric acid) and genetic associations. Crystal analysis: shape, birefringence and color Clinical Manifestations: Articular and extra- articular involvement, Pattern of involvement Laboratory Findings: Hyperuricemia (suggestive not diagnostic) Radiographic Evaluation: Findings Clinical course and prognosis
, Psudogout (Ca pyrophosphate), Basic calcium phosphate. Etiology: Role of metabolic factors (overproduction or underexcretion of uric acid) and genetic associations. Crystal analysis: shape, birefringence and color. Clinical Manifestations: Articular and extra- articular involvement, Pattern of involvement. Laboratory Findings: Hyperuricemia (suggestive not diagnostic) Radiographic Evaluation: Findings. Clinical course and prognosis.")
22
Synovial Fluid Analysis
Normal Inflammatory Septic Hemorrhagic Crystal Induced Clear/Yellow Transparent Yellow/ White Translucent/ opaque Yellow/White Opaque Red Yellow/ White, Translucent/opaque <2K 2K-50K >50K N/a 10K-50K -ve Gm stain & Culture (Cx) -ve Gm stain & Culture +/- Gm stain, +/- Culture -ve Gm stain, Cx. + Crystals
 -ve Gm stain & Culture. +/- Gm stain, +/- Culture. -ve Gm stain, Cx. + Crystals.")
24
Gout Clinical picture:
Usually adult men, If occurs in adolescent- underlying enzyme disorders, Rare in pre-menopausal women Articular disease- Acute gouty arthritis Intercritical (or interval) gout Chronic tophaceous gout Intermittent, recurrent attacks Involvement of 1st MTP is typical, Any joint can be involved. Spine disease: Can involve any level
 gout. Chronic tophaceous gout. Intermittent, recurrent attacks. Involvement of 1st MTP is typical, Any joint can be involved. Spine disease: Can involve any level.")
25
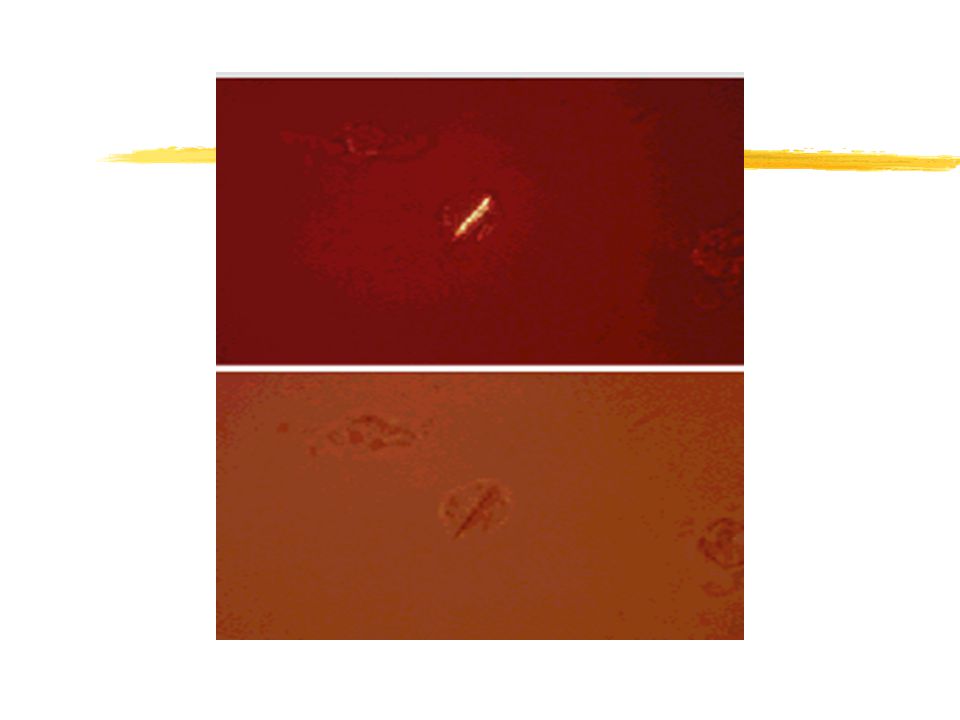
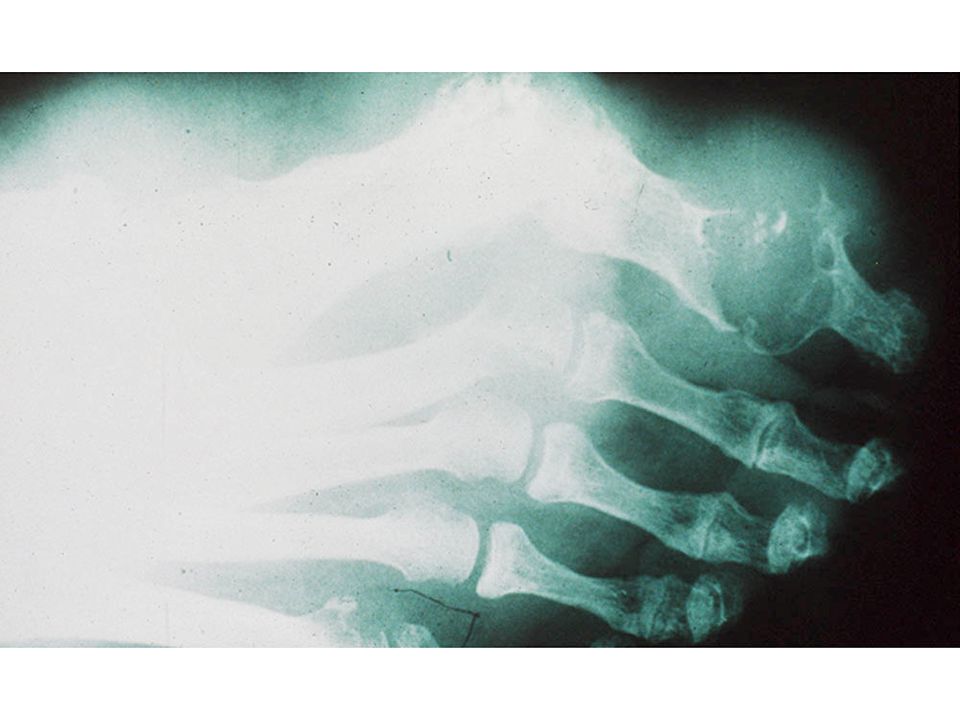
Gout Clinical picture: Extra-Articular disease Tophi
Renal disease: Uric acid nephrolithiasis and interstitial nephropathy Laboratory abnormalities Hyperuricemia: helpful not diagnostic Crystal analysis: negatively birefringence, needle shaped, yellow when parallel

27
a↑ b→

29
Gout Unusual presentations: Poly-articular gout Transplantation gout:
Typically patient on cyclosporine Rapid progression of gout Common in cardiac transplantation Moonshine gout (saturnine gout)
")
30
Gout Treatment: Acute Attacks
NSAIDs: Any NSAID works fine ( Indomethacin is NOT the preferred agent) Colchicine: remember colchicine associated GI events and neuro-myopathy Steroids: Systemic and Intraarticular
 Colchicine: remember colchicine associated GI events and neuro-myopathy. Steroids: Systemic and Intraarticular.")
31
Gout Treatment: Management of Hyperuricemia:
Allopurinol: Remember hypersensitivity syndrome and dose adjustment in renal disease, prophylaxis with colchicine initially to avoid acute attack Uricosuric agents: probenecid and sulfinpyrazone (Ineffective in Renal insufficiency, do not use in patients with renal stones) Uloric/Febuxostat (XO blocker). Lower risk of hypersenstivity Pegloticase (Krystexxa -recombinant porcine like uricase)
 Uloric/Febuxostat (XO blocker). Lower risk of hypersenstivity. Pegloticase (Krystexxa -recombinant porcine like uricase)")
32
Gout Questions asked Patient scenario: middle aged male, outpatient, acute illness inpatient: Post MI, post surgical, ESRD Read the Q- Scenarios-acute attack, asymptomatic, chronic state Role of 24 hour urine collection. Patient with sudden swollen single joint. What to do? Aspiration reveals crystals: findings diagnostic of an acute attack Co-existent infection with the crystals: Gm stain

33
Gout Questions asked Patient with HTN and gout. What medication he is likely on? What to do? Treatment of acute attack. Choices? Long term management when asymptomatic? When to use - steroids in treatment of an acute attack? Treatment of tophaceous gout? Allopurinol dose adjustment in renal insufficiency?

34
Gout Questions asked Allopurinol/Feboxustat-in a transplant patient? Interaction with what drug? What to substitute? Patient with heme malignancy planning chemo. What drug used for prophylaxis? Patient on Allopurinol comes with skin rash, cough? What test to do? Management? Drug of choice in patient with renal stones, renal insufficiency? Not to start what drug during an acute attack?

35
Q A 60-year-old man is referred to you for management of gouty arthritis. Episodic attacks of acute arthritis involving the feet and ankles began nine years ago and were confirmed by urate crystal identification. Initially, the attacks responded to nonsteroidal anti-inflammatory drugs, but symptoms became more frequent and are now chronic. Medical history includes hypertension, non–insulin-dependent diabetes mellitus, and coronary artery disease. For three years the patient has taken colchicine, 0.6 mg every two days; and allopurinol, 300 mg daily. Other current medications are furosemide, 20 mg daily; and amlodipine, 10 mg daily. Laboratory studies: Hematocrit 34% Hemoglobin 11.6 g/dL, Platelet count 504,000/cu mm Erythrocyte sedimentation rate 60 mm/hr, Blood urea nitrogen 45 mg/dL Serum creatinine 2.5 mg/dL Serum potassium 5.1 mEq/L Serum uric acid 8.5 mg/dL Serum C-reactive protein 3.8 mg/dL Creatinine clearance 25 mL/min Physical examination reveals blood pressure of 128/72 mm Hg. The ankles and feet are minimally swollen. Tophaceous deposits are present in the outer helix of the right ear and left olecranon bursa. Which of the following is the best treatment now to manage this patient’s gout? (A) Add fenofibrate, 600 mg twice daily, to the current drug regimen (B) Add probenecid, 500 mg twice daily, to the current drug regimen (C) Change allopurinol to oxypurinol, 100 mg daily (D) Increase allopurinol to 400 mg daily
 Add fenofibrate, 600 mg twice daily, to the current drug regimen. (B) Add probenecid, 500 mg twice daily, to the current drug regimen. (C) Change allopurinol to oxypurinol, 100 mg daily. (D) Increase allopurinol to 400 mg daily.")
36
CPPD 5 patterns: pseudogout, pseudo-rheumatoid, pseudo-OA, pseudo- AS, Pseudo-neuroarthritis. Involves larger joints: typically knee. Positively birefringent, rhomboid shaped crystals, bluish when parallel.

37
CPPD Typical Presentations: Acute inflammation of knee in elderly.
Post-op acute synovitis in elderly OA in unusual sites Associations with CPPD: 4 H – hypophosphatesia, hypomagnesimia, hemochromatosis, hyperpathyroidism Treatment: NSAIDs, Intra-articular steroids, No long term metabolic management

39
Basic Calcium Phosphate disease
Patterns Acute calcific-periarthritis, Tendonitis, bursitis Idiopathic destructive arthritis of shoulder (Milwaukee shoulder): typically elderly women with bilateral pain, swelling and loss of joint function, large effusion with severe destruction on radiograph. Crystals: appear as clumps, Alizarin red S staining. Treatment: NSAIDs, Intra-articular steroids, No long term metabolic management
: typically elderly women with bilateral pain, swelling and loss of joint function, large effusion with severe destruction on radiograph. Crystals: appear as clumps, Alizarin red S staining. Treatment: NSAIDs, Intra-articular steroids, No long term metabolic management.")
40
Crystal Arthritis Questions asked
Patient scenario: elderly male, multiple medical problems, outpatient, acute inpatient Abnormal Xray: CPPD deposition, crystal analysis. 55 year old patient with DM, episodic pain in wrist, knees, fatigue and decreased libido. Next test? Likely diagnosis? Treatment of acute attack. Choices? Long term management ? Patient with severe R shoulder pain. Xrays show destruction. Likely diagnosis? Differential diagnosis?

41
Autoantibodies

42
SLE Epidemiology Etiology: Role of genetic and environmental factors. DR3 association. Pathology: Role of B-cells and autoantibodies. Clinical Manifestations: Systemic manifestations with commonly involved organs, types of skin involvement (discoid, sub-acute cutaneous and others), renal involvement and types, articular involvement. Laboratory Findings: Laboratory Findings: routine laboratory changes, inflammatory markers, autoantibody profiles, evaluation of pro-coagulation factors. Clinical course and prognosis: course, morbidity and mortality, prognosis, risk for family members.
, renal involvement and types, articular involvement. Laboratory Findings: Laboratory Findings: routine laboratory changes, inflammatory markers, autoantibody profiles, evaluation of pro-coagulation factors. Clinical course and prognosis: course, morbidity and mortality, prognosis, risk for family members.")
43
SLE MNEMONIC DOPAMIN RASH 4 or more positive criteria DISCOID RASH
ORAL ULCERS PHOTOSENSITIVITY ANA MALAR RASH IMMUNOLOGICAL PHENOMENON(Le Cell, Ds DNA, Sm, APL ab, false + RPR, ) NEUROLOGICAL(Seizures,Psychosis) RENAL(Nephrotic,Nephritic) ARTHRITIS SEROSITIS HEMATOLOGICAL (Leukopenia, Thrombocytopenia, anemia) 4 or more positive criteria
 NEUROLOGICAL(Seizures,Psychosis) RENAL(Nephrotic,Nephritic) ARTHRITIS. SEROSITIS. HEMATOLOGICAL (Leukopenia, Thrombocytopenia, anemia) 4 or more positive criteria.")
44
Malar Rash in SLE ©Copyright Science Press Internet Services

45
Discoid lupus erythematosus
©Copyright Science Press Internet Services

46
SLE Clinical picture: Articular disease - Non erosive, diffuse, +morning stiffness, Involvement of hands and feet. RASH: malar eruption, discoid rash, sub-acute cutaneous LE. Cardiopulmonary: pleuritis/effusion, pericarditis, also remember pneumonitis and alveolar hemorrhage can occur. Renal: nephritis or nephrosis ( active urine sediment / proteinuria), 6 different pathological classes upon biopsy. CNS: Seizures or psychosis, vasculitis/ cereberitis can occur Hematological: (Leukopenia, ITP, hemolytic )
, 6 different pathological classes upon biopsy. CNS: Seizures or psychosis, vasculitis/ cereberitis can occur. Hematological: (Leukopenia, ITP, hemolytic )")
47
SLE Clinical picture: Immunological studies:
ANA + in high titer (100 %), Anti-Ds DNA (60-70%), Anti Smith (30 %). Hypo-complementemia- low c3, c4. High ESR
, Anti-Ds DNA (60-70%), Anti Smith (30 %). Hypo-complementemia- low c3, c4. High ESR.")
48
SLE Management: NSAIDs: Steroids:
Used for a number of manifestations, (remember elevated creatinine can occur due to their use too in addition to the disease itself) Steroids: Initially higher dose with taper to low dose maintenance, Short term therapy for major flares. IV pulse therapy – initial and for flares (?intermittent) Remain very important for management. Highlight risks and adverse events
 Steroids: Initially higher dose with taper to low dose maintenance, Short term therapy for major flares. IV pulse therapy – initial and for flares ( intermittent) Remain very important for management. Highlight risks and adverse events.")
49
SLE DMARDs Antimalarials: Hydroxychloroquine and chloroquine - helpful in all mild disease, adjunct in moderate/severe disease. Azathioprine: Preferred immunosuppressive in moderate/severe disease, monitor for cytopenia and hepatitis. Mycophenolate: Increasingly popular especially in renal disease. Methotrexate: used in arthritis. Cyclophosphamide: IV preferred over oral, Used in nephritis and CNS disease, Also useful in any severe/life-threatening manifestation. ( remember risk of hemorrhagic cystitis and bladder cancer, urine monitoring for this). Biologics Belumimab: Anti-Blys, useful in mild to moderate disease in combination with DMARDs, IV monthly. No additional evaluation/monitoring. Risk of infection, TB, cytopenias, PML?
. Biologics. Belumimab: Anti-Blys, useful in mild to moderate disease in combination with DMARDs, IV monthly. No additional evaluation/monitoring. Risk of infection, TB, cytopenias, PML")
50
SLE- special Circumstances
Drug-induced LE Common drug associations: procainamide, hydralazine, isoniazid, PTU and minocycline. Positive anti-histone specificity Neonatal LE Transient rash, antibodies disappear by 6 months Associated with positive SS-A and SS-B Congenital heart block Associated with positive SS-A and SS-B too Risk is less than 5% Monitor for fetal heart rate around weeks Can be treated with dexamethasone/betamethasone if detected early.

51
SLE Questions asked Patient scenario: middle aged female, AA, both outpatient and inpatient Lupus patient with psychosis, No other active symptoms, signs. Likely cause? Patient presents with rash, polyarthritis, recently on plaquenil. What to do next? Lupus patient with abnormal urine. Next diagnostic test? Biopsy shows Class IV disease. Appropriate treatment? Lupus patient (longer duration) presents with chest pain. Next test? Likely diagnosis? Cause of death?
 presents with chest pain. Next test Likely diagnosis Cause of death")
52
SLE Questions asked SLE patient now pregnant: what drugs to stop/continue? Lupus pregnancy: monitor for-----? SLE patient presents with hip pain: diagnostic test of choice? Diagnosis? Most specific autoantibody with SLE. Female patient with cough, hemoptysis, +ve ANA. Likely diagnosis? Drug induced lupus.

53
SLE Questions asked Patient with ITP also has arthralgia, fever. Next test? Patient with +ve ANA, fatigue presents with weakness of lower extremities, BB incontinence. Next Test? Diagnosis? Lupus nephritis patient treated with cyclophophamide. Presents with hematuria (+ UA). Cause & Next test? SLE patient presents with high fever, SOB, changing heart murmur. Diagnosis? SLE patient with shortness of breath and diffuse reticular infiltrates on chest Xray/CT. Diagnosis?
. Cause & Next test SLE patient presents with high fever, SOB, changing heart murmur. Diagnosis SLE patient with shortness of breath and diffuse reticular infiltrates on chest Xray/CT. Diagnosis")
54
Q A 43-year-old woman is evaluated for increasing headaches and memory problems. She has had systemic lupus erythematosus (SLE) for ten years. Currently, she has a moderately active level of SLE with malar rash, arthritis, proteinuria, and serum creatinine of 1.8 mg/dL. Her medical history includes lupus nephritis for which she was treated with prednisone and mycophenolate mofetil. She has multiple medication allergies including sulfa, penicillin, hydrochlorothiazide, and angiotensin-converting enzyme inhibitors. Magnetic resonance imaging (MRI) of the brain is ordered to assess the patient’s neurologic symptoms. Later in the day, the neuroradiologist requests that MRI be performed without contrast. For which of the following complications is the patient at risk if she has an MRI with contrast? (A) Renal failure (B) Contrast allergic reaction (C) Hypotension (D) Nephrogenic systemic fibrosis 54
 for ten years. Currently, she has a moderately active level of SLE with malar rash, arthritis, proteinuria, and serum creatinine of 1.8 mg/dL. Her medical history includes lupus nephritis for which she was treated with prednisone and mycophenolate mofetil. She has multiple medication allergies including sulfa, penicillin, hydrochlorothiazide, and angiotensin-converting enzyme inhibitors. Magnetic resonance imaging (MRI) of the brain is ordered to assess the patient’s neurologic symptoms. Later in the day, the neuroradiologist requests that MRI be performed without contrast. For which of the following complications is the patient at risk if she has an MRI with contrast (A) Renal failure. (B) Contrast allergic reaction. (C) Hypotension. (D) Nephrogenic systemic fibrosis. 54.")
55
Sjogren’s syndrome Classification criteria: Ocular symptoms: dry eyes
Oral symptoms: Xerostomia Abnormal Schirmer's test. Five millimeters of unstimulated wetting of filter paper in 5 minutes Rose bengal staining of the cornea Abnormal parotid salivary flow rate Abnormal radio nuclide scan of the parotid glands Abnormal parotid gland sialography Abnormal Biopsy of minor salivary glands (usually lip biopsy). Positive SS-A and SS-B
. Positive SS-A and SS-B.")
56
Sjogren’s syndrome Systemic manifestations: Treatment:
Articular disease Hyperglobulinemia Leukocytoclastic vasculitis Peripheral neuropathy/ MS like illness Cryoglobulinemia Risk of lymphoma Treatment: Careful management of oral and ocular symptoms NSAIDS and Plaquenil

57
Antiphospholipid Antibody syndrome
Classification criteria: Definite APS = 1 clinical + 1 laboratory criteria Clinical — 1 or more episodes of venous, arterial, or small vessel thrombosis and/or Pregnancy morbidity — 1. Otherwise unexplained death at 10 weeks gestation of a morphologically normal fetus, or 2. One or more premature births before 34 weeks gestation because of eclampsia, preeclampsia, or placental insufficiency, or 3. Three or more embryonic (<10 week gestation) unexplained pregnancy losses. Laboratory — The presence of aPL , on two or more occasions at least 12 weeks apart and no more than five years prior to clinical manifestations, as demonstrated by one or more of the following - 1. Positive IgG and/or IgM anticardiolipin antibody 2. Positive Antibodies to ß2-glycoprotein I of IgG or IgM isotype 3. Positive lupus anticoagulant Treatment: Lifelong anticoagulation goal of INR is close to 3 or higher Use heparin or LMW heparin during pregnancy to avoid morbidity associated with it Plaquenil may be helpful
 unexplained pregnancy losses. Laboratory — The presence of aPL , on two or more occasions at least 12 weeks apart and no more than five years prior to clinical manifestations, as demonstrated by one or more of the following - 1. Positive IgG and/or IgM anticardiolipin antibody 2. Positive Antibodies to ß2-glycoprotein I of IgG or IgM isotype 3. Positive lupus anticoagulant. Treatment: Lifelong anticoagulation goal of INR is close to 3 or higher. Use heparin or LMW heparin during pregnancy to avoid morbidity associated with it. Plaquenil may be helpful.")
58
Catastrophic Anti-phospholipid Antibody syndrome
-Associated with high morbidity and mortality -Treatment requires anticoagulation and Possibly plasmapharesis, IVIG, IV cyclophosphamide

59
SLE and related syndromes
Questions asked. Female patient with fatigue, arthralgia, dry eyes, dry mouth. What test to order next? Likely diagnosis? Confirmatory test? 2. Patient with Sjogren’s presents with fever, weight loss, LN +. What to do next? 3. Symptomatic treatment of dry eyes, dry mouth. 4. Male patient with parotid swelling, Biopsy CD 8+ lymphocytic infiltrate. Test? Diagnosis? 5. Pregnant patient has fetal bradycardia- CHB, what test to do & RX? 6. Pregnant patient with 2nd or later pregnancy loss. what test to do? 7. Patient with APLS on coumadin now wants to be pregnant. What is appropriate therapy?

60
Systemic Sclerosis and related syndromes

61
Systemic Sclerosis One major criterion or two or more minor criteria were found to be 97% sensitive & 98% specific. Major criterion: Proximal scleroderma (skin thickening) is the single major criterion (proximal to MCPs). Minor Criteria: Sclerodactyly, Digital pitting scars of fingertips or loss of substance of the finger pad, Bilateral basilar pulmonary fibrosis.
 is the single major criterion (proximal to MCPs). Minor Criteria: Sclerodactyly, Digital pitting scars of fingertips or loss of substance of the finger pad, Bilateral basilar pulmonary fibrosis.")
62
Systemic Sclerosis Clinical picture:
Skin: Proximal skin thickening ( above wrists and below neck) Articular disease - Non erosive, diffuse Vascular: Raynaud’s – severe, pitting, ulcerations and necrosis. Nailfold capillary abnormalities Pulmonary: ILD and Fibrosis with abnormal CT scan and restrictive pattern on PFT Cardiac: conduction system fibrosis with arrhythmias Renal: Remember SCLERODERMA RENAL CRISIS and its features ( rapid rise in creatinine, severe HTN and bland urine sediment, onion skinning on pathology) GI System: esophageal dysmotility, intestinal dysmotility and wide mouth diverticulae. Immunological studies: ANA +ve (70-80%), Anti SCL-70 +ve (30-60%).
 Articular disease - Non erosive, diffuse. Vascular: Raynaud’s – severe, pitting, ulcerations and necrosis. Nailfold capillary abnormalities. Pulmonary: ILD and Fibrosis with abnormal CT scan and restrictive pattern on PFT. Cardiac: conduction system fibrosis with arrhythmias. Renal: Remember SCLERODERMA RENAL CRISIS and its features ( rapid rise in creatinine, severe HTN and bland urine sediment, onion skinning on pathology) GI System: esophageal dysmotility, intestinal dysmotility and wide mouth diverticulae. Immunological studies: ANA +ve (70-80%), Anti SCL-70 +ve (30-60%).")
64
Sclerodactyly ©Copyright Science Press Internet Services

65
Limited Systemic Sclerosis
Limited skin involvement: Distal to MCPs (still systemic disease-organs involved) Non-CREST syndrome CREST syndrome: association with anti- centromere antibody. Calcinosis Raynaud’s phenomemnon Esophageal dysmotility Sclerodactyly Telengeactasias
 Non-CREST syndrome. CREST syndrome: association with anti- centromere antibody. Calcinosis. Raynaud’s phenomemnon. Esophageal dysmotility. Sclerodactyly. Telengeactasias.")
66
Mat-like telangiectasia
©Copyright Science Press Internet Services

67
Systemic Sclerosis Management:
Avoid high dose steroids ( > 15 mg) unless absolutely needed Organ based therapy: Raynaud’s phenomenon: Lifestyle changes, Calcium channel blockers, Sympathectomy, endothelin-1 blockers Renal disease: ACE inhibitors (remember continue despite early elevation in creatinine during renal crisis) GI disease: PPIs, Prokinetic agents, Flagyl as needed Arthritis: Methotrexate
 unless absolutely needed. Organ based therapy: Raynaud’s phenomenon: Lifestyle changes, Calcium channel blockers, Sympathectomy, endothelin-1 blockers. Renal disease: ACE inhibitors (remember continue despite early elevation in creatinine during renal crisis) GI disease: PPIs, Prokinetic agents, Flagyl as needed. Arthritis: Methotrexate.")
68
Systemic Sclerosis Management: Specific Therapy:
Alveolitis: Corticosteroids, IV Cyclophosphamide, Azathioprine. Pulmonary Hypertension: Endothelin-1 receptor antagonists: Bosentan, Sitaxsentan Prostacyclin analogues: Epoprostenol, Treprostinil, iloprost – I.V. and inhaled Phosphodiesterase type 5 inhibitors: Sildenafil- Revatio Lung Transplantation

69
Systemic Sclerosis and related syndromes
Questions asked Patient scenario: middle aged female Patient presents with skin thickening, cough, + ANA. Work-up should include? Antibody? Likely diagnosis? Pulmonary findings Patient with scleroderma, presents with HTN. Drug of choice? Same patient comes with severe HTN, MS changes and renal failure. Diagnosis? Treatment?

70
Systemic Sclerosis and related syndromes
Questions asked Primary Raynaud’s vs Secondary Patient with Raynaud’s, skin thickening, GERD. Antibody? Also has syncope and SOB. What test? Diagnosis? Treatment? Patient with Raynaud’s. Treatment? Lifestyle changes? Raynaud’s patient asks about long term prognosis? Findings on examination/office based testing associated with a worse prognosis?

71
Systemic Sclerosis and related syndromes
Questions asked SS patient with weight loss, bloating, BM irregularity, foul smelling stools. Diagnosis? Findings on a radiographic test? SS patient with abnormal PFT. What is the worse prognosis finding? Pulmonary HTN: treatment. Raynaud’s+arthritis+myositis= what overlap syndrome? Associated antibody? Typical pulmonary finding? Male patient with swollen arms, legs, orange peel appearance. Next test? Diagnosis? Patient with DM- swelling/skin thickening on the back. Diagnosis?

72
Q A 35-year-old woman has been under your care for nine months for systemic sclerosis characterized by Raynaud’s phenomenon, sclerodactyly, esophageal reflux, hypopigmentation of the upper back and chest, and arthralgias of the elbows and hands.One month ago, physical examination showed pulse rate was 70 per minute and blood pressure was 114/70 mm Hg. Diffuse subcutaneous thickening of the skin on the trunk and extremities was noted, as well as a small ulcer over right index finger pulp. Nailfold capillaroscopy showed dilated peripheral capillary loops. All laboratory studies were normal. She now presents for a follow-up visit, and reports malaise and fatigue. Blood pressure is 138/88 mm Hg, but results of her physical examination are otherwise unchanged from those of her previous visit. Laboratory studies: Hemoglobin 10.2 g/dL, Leukocyte count 7500/cu mm, Platelet count 105,000/cu mm, Blood urea nitrogen 12 mg/dL, Serum creatinine 0.9 mg/dL, Peripheral blood film RBC fragmentation; helmet cells; basophilic stippling Direct (Coombs’ test) Negative, VWF protein Normal, U/A Trace protein; 0–2 RBC/hpf Which of the following complications is most likely to occur in this patient now? A. Cerebral thrombosis B. Macrophage activation syndrome C. Pulmonary alveolar hemorrhage D. Pulmonary hypertension E. Renal crisis
 Negative, VWF protein Normal, U/A Trace protein; 0–2 RBC/hpf. Which of the following complications is most likely to occur in this patient now A. Cerebral thrombosis. B. Macrophage activation syndrome. C. Pulmonary alveolar hemorrhage. D. Pulmonary hypertension. E. Renal crisis.")
Similar presentations


 CBC with differential.>")




>")

3-6 mg QD4-6 monthsDiarrheaCBC, urinalysis.>")


 Etiology is.>")








