Download presentation
Presentation is loading. Please wait.

2
Examination of periodontium
Prof. Magdy K. Hamam Prof. of Oral Medicine O Principles of Oral Diagnosis: Gary C. Coleman John F. Nelson 1st Ed (1993)
")
3
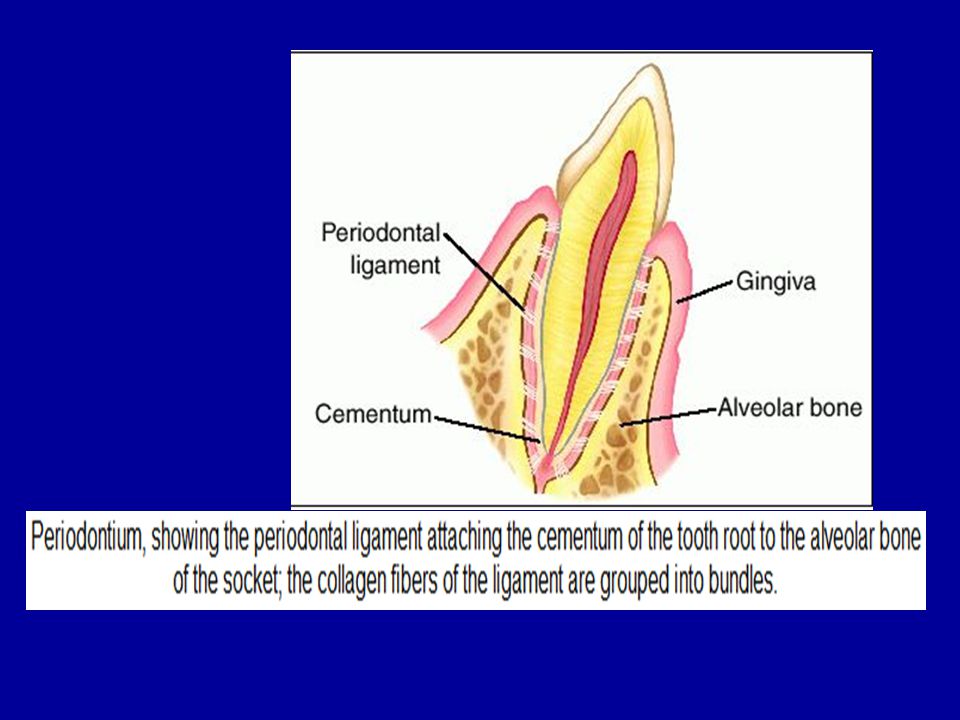
1- The periodontium 1- gingiva 2- periodontal ligament 3- alveolar bone 4- cementum 11- Tooth mobility

4
1- gingiva Inspection The periodontium consists of tissues :-
2 soft tissues ( gingiva & periodontal ligament ) 2 hard tissues ( cementum & alveolar bone ) 1- gingiva It divided into ( free gingiva , interdental papilla and attached gingiva ) Inspection Colour is pink with stippling Level of attachment of gingiva ( Stippling is a consequence of the microscopic elevations and depressions of the surface of the gingival tissue due to the connective tissue projections within the tissue. "The degree of keratinization and the prominence of stippling appear to be related."To be more specific, stippling occurs at sites of fusion of the epithelial ridges (also known as rete pegs) and correspond to the fusion of the valleys created by the connective tissue papillae )
 2 hard tissues ( cementum & alveolar bone ) 1- gingiva. It divided into ( free gingiva , interdental papilla and attached gingiva ) Inspection. Colour is pink with stippling. Level of attachment of gingiva. ( Stippling is a consequence of the microscopic elevations and depressions of the surface of the gingival tissue due to the connective tissue projections within the tissue. The degree of keratinization and the prominence of stippling appear to be related. To be more specific, stippling occurs at sites of fusion of the epithelial ridges (also known as rete pegs) and correspond to the fusion of the valleys created by the connective tissue papillae )")
5
Palpation Consistency ( firm and resilient ) Consistency is assessed by firmly passing the gloved finger all over the gingival tissue and the vestibule ( maxillary tubersity area of one side to other side then from mand.third region of one side to other side )
")
7
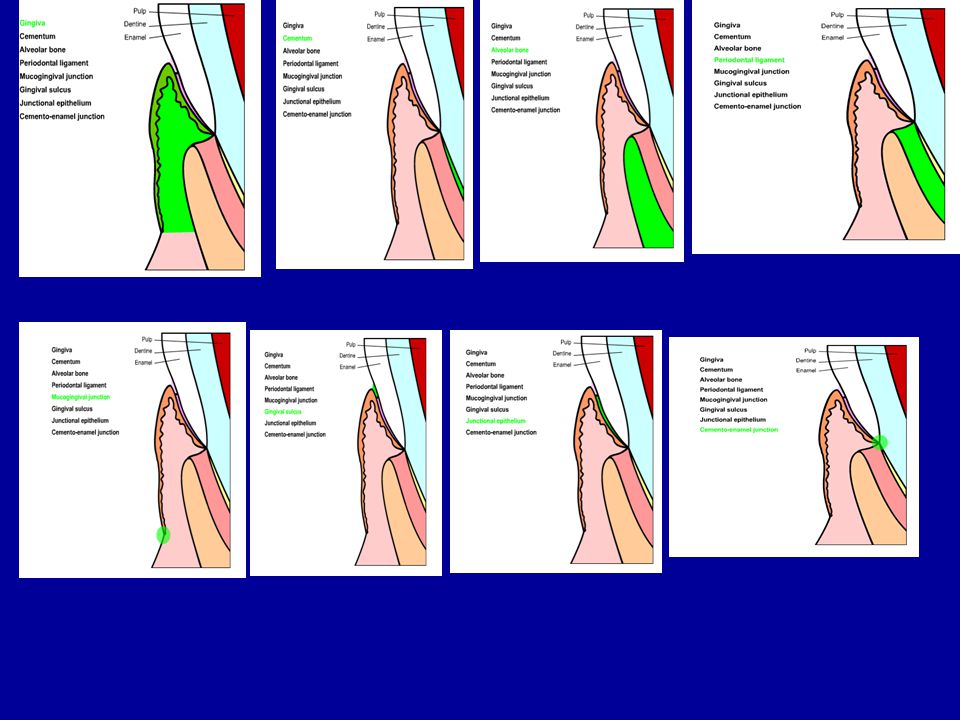
The gingiva is divided anatomically into :-
A- marginal gingiva B- attached gingiva C- interdental papillae A- Marginal ‘’ unattached ‘’ gingiva ( it is the border of the gingiva surrounding the teeth in collar – like fashion ) a shallow linear depression demarcating the marginal gingiva from the attached gingiva is the ‘’ free gingival groove ‘’ it forms the soft tissue wall of the gingival sulcus . The gingival sulcus is the shallow space around the tooth bounded by the surface of the tooth on one side and the epithelium lining the free margin of the gingival on the other . It is v-shaped and permits the entrance of a periodontal probe .
 a shallow linear depression demarcating the marginal gingiva from the attached gingiva is the ‘’ free gingival groove ‘’ it forms the soft tissue wall of the gingival sulcus . The gingival sulcus is the shallow space around the tooth bounded by the surface of the tooth on one side and the epithelium lining the free margin of the gingival on the other . It is v-shaped and permits the entrance of a periodontal probe .")
9
B- the attached gingiva
It is continuous with the marginal gingiva . It is firm , resilient and tightly bound to the underlying alveolar bone . The facial part of the attached gingiva extends to a loose and movable alveolar mucosa from which it is demarcated by the mucogingival junctional. C- the interdental gingiva It occupies the interproximal space beneath the area of the tooth contact ( original embrasure ) It usually consists of tow papillae , one facial and lingual and ‘’ col ‘’ Col which is a valley – like depression ,immediately comes under the contact points of the teeth This area is believed to be the initial site of periodontal diseases .
 It usually consists of tow papillae , one facial and lingual and ‘’ col ‘’ Col which is a valley – like depression ,immediately comes under the contact points of the teeth. This area is believed to be the initial site of periodontal diseases .")
11
Abnormalities The following abnormalities should be noted :-
Gingivitis Periodontitis Pericoronitis Gingival recession Gingival abscesses Gingival growths Exostoses on the attached gingiva Gingival enlargements Gingival bleeding Gingival ulcerative lesions Gingival desquamation Gingival blisters Black racial pigmentation

12
2- periodontal ligament ( P.L )
It is composed of tissues that surround the root of the tooth and serve as the attachment of the tooth to the alveolar bone Principal collagen fibers of the periodontal ligament :- ( alveolar crestal fibers – horizontal fibers – oblique fibers - apical fibers ) Functions of periodontal ligament :- 1- mechanical 2- formative 3- nutritive 4- sensory
 Functions of periodontal ligament :- 1- mechanical. 2- formative. 3- nutritive. 4- sensory.")
13
1- Sopt probing Periodontal Probing
Probing of the gingival sulcus depth by 6 point per tooth format is usually performed .there are 2 methods 1- Sopt probing Is the insertion and withdrawal of the probe at each of the six depth reading areas . Inaccurate reading are obtained when sub gingival sulcus is present . 2- Circumferential probing Is the placing of the probe in the sulcus at the distobuccal line angle and following the sulcus around to the mesial noting the depth reading . Six reading on each tooth , 3 buccal and 3 lingual Bleeding upon probing should be recorded for each tooth ,then the bleeding index can be calculated .

14
3- The alveolar bone ●It is made up of bony processes project that project from the basal portions of the mandible and maxilla . ●These processes are composed of cancellous or spongy bone covered With cortical bone ●The alveolar bone form is present as the teeth develop and erupt into the oral cavity, following teeth extraction they gradually resorb. ●The spaces in the alveolar bone that accommodate the roots of the teeth are known alveoli. The alveoli are lined with a layer of bone called alveolar bone proper or cribriform plate. ● This layer of bone appears as white line on the radiograph and known as lamina dura ● This layer of bone covers the crest of the interproximal bone and called crystal lamina dura

16
● The cancellous and cortical bone that surrounds the alveolar bone proper is known supporting alveolar bone. ● The bone located between the roots of the adjacent teeth called interproximal bone or interdental septum . ● The bone located between the roots of multicoated teeth is known as the inter-radicular bone. ● The alveolar process located on the facial or lingual surfaces of the roots of teeth is known as the radicular bone.

17
4- Cementum: Cementum is calcified tissue that cover the root of the tooth and provides a means of attachment for attachment for the periodontal ligament fibers to the tooth. Cementum is continuously formed on root surfaces that are in Contac with the periodontal ligament or gingival fibers.

18
New cementum cannot be formed on root surfaces that have been denuded of their connective tissues attachment because cells in the periodontal ligament form it. The cementum composition makes it slightly harder than bone. The width of cementum varies from 16-60um in the coronal half of the root, its much thicker, on the apical third of the root, being um.

19
Periodontal examination and diagnosis
The importance of periodontal examination is to determine the following: Whether the patient periodontium is healthy or diseased. The extent of the tissue damaged if pathological change is present. The characteristics of the periodontal disease that well enable the determination of the diagnosis, etiology, prognosis and treatment plane. Means of clinical examination: I- Inspection: Gingival colour: pink, red, bluish red or other colour variation. Gingival contour “Both marginal and papillary”: normal, rounded, crater or other anatomical variation. Gingival size: normal size, gingival enlargement or gingival recession. Position of the gingival: Adjacent to cemento-enamel junction or receded coronal to cement enamel junction.

20
II- Palpation: Gingival consistency: Normal, edematous, fibrotic or fiber edematous bidigital or bimanual palpation. Gingival texture “stippling”: normal, decrease, increase or lack of stippling. Tooth mobility: by using the handles of two dental instruments apply alternate pressure on the buccal or lingual surface of each tooth. Migration: migration is a pathological movement of the teeth in labial, distal, mesial or supra occlusion. Migration is common feature of some periodontal disease e.g aggressive periodontal, it may relate to some habit e.g. tongue thrusting.

21
The tooth mobility is usually related to one or more of the following:
1- Periodontal inflammation 2- Bone loss “bone resorption”. 3- The presence of occlusal trauma Classification of tooth mobility: Grade I: Slight mobility but the patient is not aware of it. Grade II: Moderate mobility but the patient know it and not feel discomfort during eating. Grade III: Severe mobility and the patient feel discomfort during eating.

22
III- Probing: Bleeding on probing: No or yes if yes slight, moderate or severe. Evaluation of probing depth: By use of the calibrated periodontal probe the Clinician can evaluate the depth of the periodontal pocket and attachment level.

23
Roentgenographic evaluation
Evaluation of bone involvement by x-ray examination may reveal one of the following: Cup shape resorption of the alveolar crest “horizontal resorption” is an indication for the presence of periodontal destruction e.g. chronic periodontitis. Vertical bone resorption usually associated with aggressive periodontitis.

Similar presentations



 (cont.)>")










 Bone and alveolar bone Dr Jamal Naim>")
.>")






