Download presentation
Presentation is loading. Please wait.

1
Squamous Cell H&N Cancer Hypopharynx Therapeutic Approach Ricardo Hitt MD, PhD Hospital Universitario 12 Octubre MADRID STATEMENTS 2008

2
Squamous Cell H&N Cancer Hypopharynx The majority of hypopharyngeal lesions originate in the pyriform sinus. On admission, 75% of the patients have clinically positive nodes. clinically positive nodes. There is no difference in the risk of neck metastases by T stage. metastases by T stage.

3
HN surgeon Decision making Medical oncologist Treatment of Head and Neck Cancer Multidisciplinary Radiation oncologist

4
Decision making CLINICAL TRIAL STANDARD TREATMENT Treatment of Head and Neck Cancer Multidisciplinary

7
HYPOPHARYNGEAL CANCER HEAD AND NECK CANCER OROPHARYNX ORAL CAVITY LARYNXHIPOPHARYNX

8
HYPOPHARYNGEAL CANCER OBJECTIVES CURE ORGAN PRESERVATION QUALITY OF LIFE

9
HYPOPHARYNGEAL CANCER TODAY,WITH MEDICAL TREATMENT ORGAN PRESERVATION OVERALL SURVIVAL NEW OBJECTIVEIncrease Overall Survival and Organ Preservation NEW OBJECTIVE: Increase Overall Survival and Organ Preservation HOW???

10
J. L. Lefebvre, D. Chevalier, B. Luboinski, L. Traissac, G. Andry, D. De Raucourt, L. Collette, J. Bernier, EORTC Head and Neck Cancer Cooperative Group. F R A N C E Is Laryngeal Preservation (LP) With Induction Chemotherapy (ICT) Safe in the Treatment of Hypopharyngeal SCC? Final Results of the Phase III EORTC 24891 Trial. Last Update: ASCO 2004
 With Induction Chemotherapy (ICT) Safe in the Treatment of Hypopharyngeal SCC. Final Results of the Phase III EORTC Trial. Last Update: ASCO")
11
STUDY DESIGN Surgery + RT LP: PF + RT R Primary endpoint: OS (non-inferiority of LP) Secondary endpoints: PFS, larynx preservation Lefebvre JL, et al. JNCI 1996; 88:890-8; Lefebvre JL, et al. ASCO 2004: Abstract 5531. N = 94 N = 100 Cycle 1 PD* CR* PR* NC* Cycle 2 NC/PD* CR* PR*Cycle 3CR* PR/NC/PD* RXT 70 Gy ± salvage surgery Surgery + Postoperative RXT

12
Surgery (No CT) (N=94) (%) Larynx Preservation (N=100)(%) Stage Stage II67 Stage III5459 Stage IV3934 Site of primary Pyriform sinus7978 Aryepiglottic fold2122 PATIENT CHARACTERISTICS Lefebvre JL, et al. ASCO 2004: Abstract 5531.

13
(years) 0246810121416 0 10 20 30 40 50 60 70 80 90 100 ONNumber of patients at risk : 819449362614953 8310062472717841 Surgery LP Overall survival Larynx preservation HR: 0.88 (95% CI: 0.65 - 1.19) P=0.0015 for non-inferiority of LP Surgery Median, 44 mo Median, 25 mo (years) 0246810121416 0 10 20 30 40 50 60 70 80 90 100 ONNumber of patients at risk : 88943725166510 8810047321910521 Surgery Preservation Disease-free survival Larynx preservation Surgery Hazard Ratio: 0.83 (95% CI: 0.62-1.12) Lefebvre JL, et al. ASCO 2004: Abstract 5531. OVERALL SURVIVAL AND DFS

14
Devita. 7th Edition SURVIVAL PHARYNGEAL SCC

15
Devita. 7th Edition SURVIVAL PHARYNGEAL SCC

16
Historical standard treatment (80') for locally advanced squamous cell carcinoma of the head and neck (SCCHN) Surgery radiation (RT) Inoperable disease Operable disease Background RT (5 yr surv. 10%-20%) Concomitant CT/RT standard for inop. Pts (90’) (5yr surv. 20%- 30% )
 Concomitant CT/RT standard for inop. Pts (90’) (5yr surv. 20%- 30% ).")
17
35 previously untreated pts: 3 cycles cisplatin-5FU (CF) Response > 50% 94 % Complete response 63 % Decker D et al. ASCO Annual Meeting. Saint Louis 1982, Abstract C-757 Decker DA et al. Cancer 1983;51:1353-5 60 tumors treated with platinum-based chemotherapy Ensley J et al. ASCO Annual Meeting. Saint Louis 1982, Abstract C-767 Ensley JF et al. Cancer 1984;54:811-4 42 responses > 50% 97 % after RT 18 responses < 50% 6%6% after RT ASCO 1982: The Platinum Revolution

18
Induction CT: high RR ( 70%-80%); RC (5% - 30%) 1- 4 cycles prior to RT Subsequent RT or surgery not compromised Not clear if local control increased Response to induction CT predicts response to RT Part of a larynx preservation strategy Rationale for induction CT -1-
; RC (5% - 30%) 1- 4 cycles prior to RT Subsequent RT or surgery not compromised Not clear if local control increased Response to induction CT predicts response to RT Part of a larynx preservation strategy Rationale for induction CT -1-")
19
Induction CT reduces incidence of distant metastases Patient selection crucial (dist.met. 30%-40%) T bulky ; N (bilateral, high number, capsula rupture), Site (hypopharynx), other markers From meta-analysis: induction with PF 5% incr. OS 5yr P=0.01 2 individual studies showed survival benefit with PF (GSTTC ; GETTEC) Rationale for induction CT -2-
 T bulky ; N (bilateral, high number, capsula rupture), Site (hypopharynx), other markers From meta-analysis: induction with PF 5% incr. OS 5yr P= individual studies showed survival benefit with PF (GSTTC ; GETTEC) Rationale for induction CT -2-.")
20
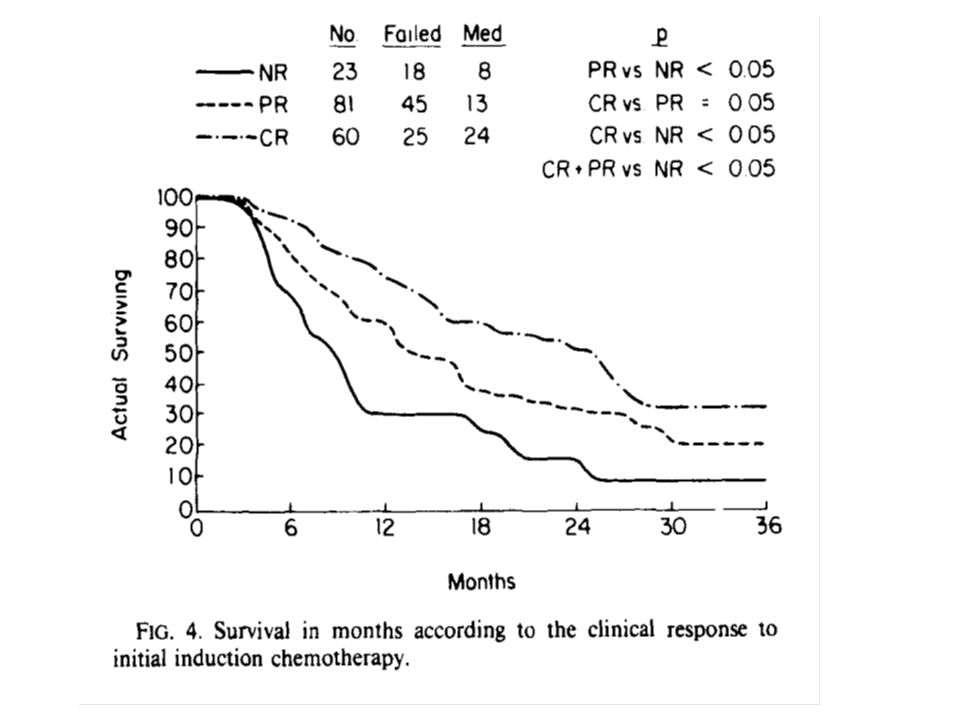
Improved Complete Response Rate and Survival in Advanced Head and Neck Cancer After Three- Course Induction Therapy With 120-Hour 5-FU Infusion and Cisplatin MICHAEL ROONEY, MD,.t JULIE KISH, MD,JOHN JACOBS, MD.( JEANNIE KINZIE, MD,ARTHUR WEAVER, MD., JOHN CRISSMAN. MD. AND MUHYl AL- SARRAF. MD Cancer 55: 1 1 23- I 1 28. 1985.

22
MACH-NC Collaborative Group: Effect of Chemotherapy on 5-Year Survival Monnerat C, et al. Ann Oncol. 2002;13:995. [Review] Pignon JP, et al. Lancet. 2000;355:949. Meta-analyses of individual patient data from randomized trial that recruited patients from 1965 to 1993 PF induction conferred a 5% survival gain at 5-years CRT conferred an 8% survival improvement at 5-years CRT=chemoradiotherapy; PF=cisplatin+5-FU. Trial CategoryNo. of TrialsNo. of PtsDifference, %p-Value All6510850+4<0.0001 Adjuvant81854+10.74 Induction315269+20.10 PF152487+50.01 Other chemotherapy16278200.91 Concomitant CRT 263727+8<0.0001

23
SCCHNC HOW CAN WE IMPROVE THESE RESULTS? Change the schedule of ICT Change the approach of treatment

24
Induction CT + Locoregional RT Remenar E, et al. ASCO 2006, abstract 5516. Bernier J, et al. ASCO 2006, abstract 5522. Vermorken JB, et al. ASCO 2004, abstract 5508. EORTC 24971/TAX 323 - Study Design Neck Dissection InoperableSCCHN Stage 3-4. Stratification: 1º tumor site Institution TPF arm (n=177) Docetaxel (75 mg/m²) Cisplatin (75 mg/m²) 5-FU (750 mg/m²/dx5) Q 3 weeks x 4 cycles PF arm (n=181) Cisplatin (100 mg/m²) 5-FU (1000 mg/m²/dx5) Q 3 weeks x 4 cycles Radiotherapy (~70 Gy over 7 weeks) Follow up Surgery for Residual Disease Treatment arms were well balanced in baseline characteristics Primary Objective: PFS
 Docetaxel (75 mg/m²) Cisplatin (75 mg/m²) 5-FU (750 mg/m²/dx5) Q 3 weeks x 4 cycles PF arm (n=181) Cisplatin (100 mg/m²) 5-FU (1000 mg/m²/dx5) Q 3 weeks x 4 cycles Radiotherapy (~70 Gy over 7 weeks) Follow up Surgery for Residual Disease Treatment arms were well balanced in baseline characteristics Primary Objective: PFS.")
25
Overall Survival EORTC 24971/TAX 323 (months) 0 0 10 20 30 40 50 60 70 80 90 100 61218243036424854606672 Treatment PF TPF Remenar E, et al. ASCO 2006, abstract 5516. Bernier J, et al. ASCO 2006, abstract 5522. Vermorken JB, et al. ASCO 2004, abstract 5508. PFTPF Median OS, mo14.218.6 Hazard ratio (95% CI)0.71 (0.56, 0.90) P-value0.0055
0.71 (0.56, 0.90) P-value")
26
Induction CT CRT Surgery Posner RM, et al. ASCO 2006, abstract SPS24. TAX 324 - Study Design Treatment arms were well balanced in baseline demographic and disease characteristics Primary Objective: Primary Objective: OS Radiotherapy (70Gy d1-5) + Weekly Carboplatin (AUC 1.5 7) Surgery is needed PF arm (n=246) Cisplatin (100 mg/m²/d1) 5-FU (1000 mg/m²/d 5) Q 3 weeks x 3 cycles TPF arm (n=255) Docetaxel (75 mg/m²) Cisplatin (100 mg/m²d1) 5-FU (1000 mg/m²/d 4) Q 3 weeks x 3 cycles N=538 Stage III/IV Epidermoidcarcinoma, no prior surgery, no hospitalization for COPD 1y Stratification: Center Center N status N status Primary site Primary site
 + Weekly Carboplatin (AUC 1.5 7) Surgery is needed PF arm (n=246) Cisplatin (100 mg/m²/d1) 5-FU (1000 mg/m²/d 5) Q 3 weeks x 3 cycles TPF arm (n=255) Docetaxel (75 mg/m²) Cisplatin (100 mg/m²d1) 5-FU (1000 mg/m²/d 4) Q 3 weeks x 3 cycles N=538 Stage III/IV Epidermoidcarcinoma, no prior surgery, no hospitalization for COPD 1y Stratification: Center Center N status N status Primary site Primary site.")
27
Posner RM, et al. ASCO 2006, abstract SPS24. TAX 324 - Study Design Primary Endpoint: Overall Survival 061218243036 42 4854606672 0 3-Year OS TPF 62% PF 48% 2-Year OS TPF 67% PF 54% Survival Time (months) Log-Rank p =.0058 Hazard ratio = 0.70 TPF (n=255) PF (n=246) TPF significantly improved overall survival vs PF 30% reduction in mortality Survival Probability (%) 10 20 30 40 50 60 70 80 90 100
 Log-Rank p =.0058 Hazard ratio = 0.70 TPF (n=255) PF (n=246) TPF significantly improved overall survival vs PF 30% reduction in mortality Survival Probability (%)")
28
HNSCC: Taxotere in Locally-Advanced Disease Posner et al. ASCO 2006. Remenaer et al., ASCO 2006 Overall Survival 061218243036424854606672 50 0 10 20 30 40 60 70 80 90 100TPF PF 061218243036424854606672TPF PF Survival Time (months) Survival Probability (%) Survival Time (months) TAX 324 30% reduction in risk of death TAX 323 29% reduction in risk of death
 Survival Probability (%) Survival Time (months) TAX % reduction in risk of death TAX % reduction in risk of death.")
29
Hitt R, et al. ASCO 2006, abstract 5515. Phase III Trial PF ± Docetaxel CRT vs CRT Study Design Primary endpoint phase III: TTF SCHNN Stage III, IV (locally advanced) Unresectable PF 3 cycles q 21 days Cisplatin Infusional 5-FU (N=440) TPF 3 cycles q 21 days Docetaxel Cisplatin Infusional 5-FU CRT
 Unresectable PF 3 cycles q 21 days Cisplatin Infusional 5-FU (N=440) TPF 3 cycles q 21 days Docetaxel Cisplatin Infusional 5-FU CRT.")
30
Phase III Trial PF ± Docetaxel CRT vs CRT RESPONSE RATE BY ARM TPF/CRT CRT CRT CR (complete response) 70 % 49.48 % p = 0.0080 EFFICACY Hitt R, et al. ASCO 2006, abstract 5515.

31
Al Sarraf Cancer 1985 Does the Complete Response to Induction Chemotherapy/CRT have the same benefit in survival ?

32
CHEMORADIOTHERAPY HNC STANDARD TREATMENT STANDARD TREATMENT OLD STANDARD CRT GOLD STANDARD ICT/CRT

33
CONCLUSIONS (1) Hypopharyngeal SCC has a bad prognostic with conventional treatment The objective of treatment can be : cure-quality of life For Medical Oncologist Hypopharyngeal Cancer= SCCHN To day is possible Larynx Preservation without damage OS Induction chemotherapy is feasible in a set of the patients Chemoradiotherapy can be a Radical Treatment
 Hypopharyngeal SCC has a bad prognostic with conventional treatment The objective of treatment can be : cure-quality of life For Medical Oncologist Hypopharyngeal Cancer= SCCHN To day is possible Larynx Preservation without damage OS Induction chemotherapy is feasible in a set of the patients Chemoradiotherapy can be a Radical Treatment")
34
CONCLUSIONS (2) When is possible: Salvage Surgery is recommended Now we have data about the superiority of TPF as ICT Complete Response to TPF/CRT might be a parameter as overall survival Induction TPF plus CRT might be the next standard Selection of patients is the key for treatment selection RESECTABLE////UNRESECTABLE TUMORSRESECTABLE////UNRESECTABLE TUMORS
 When is possible: Salvage Surgery is recommended Now we have data about the superiority of TPF as ICT Complete Response to TPF/CRT might be a parameter as overall survival Induction TPF plus CRT might be the next standard Selection of patients is the key for treatment selection RESECTABLE////UNRESECTABLE TUMORSRESECTABLE////UNRESECTABLE TUMORS")
Similar presentations


 CISPLATIN 40 mg/m2 Days 1 2 22 36 50 64 92 E V A L U A.>")




 versus FOLFOX4 in Patients with Advanced Colorectal Carcinoma Previously Treated.>")






 P =.024 Larynx and Hypopharynx Overall Survival 166 Patients.>")




adjuvant chemo-radiotherapy for locally advanced rectal cancer: Long term results.>")