Download presentation
Presentation is loading. Please wait.

1
obesity Done by: Nader Al Dajani Mohannad Al Romaih Masoud Al otaibi

2
Definition Obesity is defined as an excess accumulation of body fat This excess accumulation is the result of a positive energy balance where caloric intake exceeds caloric expenditure It is the most common nutritional disorder in industrialized countries and is becoming increasingly prevalent in developing countries due to changing lifestyles.

3
Epidemiology WHO’s latest projections indicate that globally in 2005: approximately 1.6 billion adults (age 15+) were overweight; at least 400 million adults were obese. WHO further projects that by 2015, approximately 2.3 billion adults will be overweight and more than 700 million will be obese. At least 20 million children under the age of 5 years are overweight globally in 2005.

4
Cont. In study done in Saudi Arabia it shows that the prevalence of overweight among male subjects was 29% vs. 27% among female subjects & The prevalence of obesity among female subjects was significantly higher than for male subjects (24% vs. 16%) This value is higher than that reported in the UK, Australian, US and Italian populations
 This value is higher than that reported in the UK, Australian, US and Italian populations.")
6
Etiology Multifactorial disorders Genetics: polygenic, each gene having a small contribution in the presence of precipitating environmental factors It has been long known that the tendency to gain weight runs in families. However, family members share not only genes but also diet and life style habits that may contribute to obesity. morbid obesity has a stronger genetic component than moderate level of excess overweight Energy imbalance Diet obesity is associated with increased food consumption Intake of excess dietary fat has been implicated as a major cause of obesity Exercises For a decades A strong link exists between physical inactivity and weight gain

8
Cont. Diseases Hypothyroidism, Cushing’s syndrome, pancreatic insulinoma, growth hormone deficiency, and hypothalamic insufficiency A variety of psychosocial factors contribute to the development of obesity and to difficulty losing weight Drugs antipsychotics (phenothiazines, butyrophenones); antidepressants and antiepileptics, (tricyclic antidepressants, lithium, valproate, carbamazepine); and insulin and some oral hypoglycemics. Whereas most of these medications contribute modestly to obesity, the large doses of steroids sometimes used to treat autoimmune diseases can cause true obesity
; antidepressants and antiepileptics, (tricyclic antidepressants, lithium, valproate, carbamazepine); and insulin and some oral hypoglycemics. Whereas most of these medications contribute modestly to obesity, the large doses of steroids sometimes used to treat autoimmune diseases can cause true obesity.")
9
Health Effects of Obesity Obesity is associated with more than 30 medical conditions, and scientific evidence has established a strong relationship with at least 15 of those conditions It has been established that obesity is associated with an increased prevalence of coronary artery disease, hypertension, diabetes mellitus, and other diseases. In addition, life expectancy is shown to be reduced in those who are obese or overweight.

10
Cont. Diabetes (Type 2) As many as 90% of individuals with type 2 diabetes are reported to be overweight or obese. Obesity has been found to be the largest environmental influence on the prevalence of diabetes in a population. Obesity complicates the management of type 2 diabetes by increasing insulin resistance and glucose intolerance, which makes drug treatment for type 2 diabetes less effective. A weight loss of as little as 5% can reduce high blood sugar.
 As many as 90% of individuals with type 2 diabetes are reported to be overweight or obese. Obesity has been found to be the largest environmental influence on the prevalence of diabetes in a population. Obesity complicates the management of type 2 diabetes by increasing insulin resistance and glucose intolerance, which makes drug treatment for type 2 diabetes less effective. A weight loss of as little as 5% can reduce high blood sugar..")
11
Cont. Hypertension Over 75% of hypertension cases are reported to be directly attributed to obesity. Weight or BMI in association with age is the strongest indicator of blood pressure in humans. The association between obesity and high blood pressure has been observed in virtually all societies, ages, ethnic groups, and in both genders. The risk of developing hypertension is five to six times greater in obese adult Americans, age 20 to 45, compared to non-obese individuals of the same age.

12
Cont. Cardiovascular Disease (CVD) Obesity increases CVD risk due to its effect on blood lipid levels. Weight loss improves blood lipid levels by lowering triglycerides and LDL (“bad”) cholesterol and increasing HDL (“good”) cholesterol. Weight loss of 5% to 10% can reduce total blood cholesterol. The effects of obesity on cardiovascular health can begin in childhood, which increases the risk of developing CVD as an adult. Overweight and obesity increase the risk of illness and death associated with coronary heart disease. Obesity is a major risk factor for heart attack, and is now recognized as such by the American Heart Association.
 Obesity increases CVD risk due to its effect on blood lipid levels. Weight loss improves blood lipid levels by lowering triglycerides and LDL ( bad ) cholesterol and increasing HDL ( good ) cholesterol. Weight loss of 5% to 10% can reduce total blood cholesterol. The effects of obesity on cardiovascular health can begin in childhood, which increases the risk of developing CVD as an adult. Overweight and obesity increase the risk of illness and death associated with coronary heart disease. Obesity is a major risk factor for heart attack, and is now recognized as such by the American Heart Association..")
13
Cont. Stroke Elevated BMI is reported to increase the risk of ischemic stroke independent of other risk factors including age and systolic blood pressure. Abdominal obesity appears to predict the risk of stroke in men. Obesity and weight gain are risk factors for ischemic and total stroke in women.

14
Osteoarthritis (OA) Obesity is associated with the development of OA of the hand, hip, back and especially the knee. At a Body Mass Index (BMI) of > 25, the incidence of OA has been shown to steadily increase. Modest weight loss of 10 to 15 pounds is likely to relieve symptoms and delay disease progression of knee OA.
 of > 25, the incidence of OA has been shown to steadily increase. Modest weight loss of 10 to 15 pounds is likely to relieve symptoms and delay disease progression of knee OA..")
15
Sleep Apnea Obesity, particularly upper body obesity, is the most significant risk factor for obstructive sleep apnea. There is a 12 to 30-fold higher incidence of obstructive sleep apnea among morbidly obese patients compared to the general population. Among patients with obstructive sleep apnea, at least 60% to 70% are obese.

16
Cont. Cancers Carpal Tunnel Syndrome (CTS) Chronic Venous Insufficiency (CVI) & Deep Vein Thrombosis (DVT) Gallbladder Disease Gout abdominal hernias
 Chronic Venous Insufficiency (CVI) & Deep Vein Thrombosis (DVT) Gallbladder Disease Gout abdominal hernias.")
17
Cont. Impaired Respiratory Function Infertility Liver Disease Low Back Pain Surgical Complications Daytime Sleepiness

18
HISTORY

19
History : You must take full Hx with out forgetting to ask about obesity cause(s) … ( Etiology ) -Energy imbalance -familial -Diseases -Medications
 … ( Etiology ) -Energy imbalance -familial -Diseases -Medications")
20
And ask about diseases which arising from obesity like: DM II HTN CVD OA Sleep apnea…. & Other diseases

21
All of the systems that make the body function are affected by morbid obesity

22
Cardiovascular System Digestive System Endocrine System Musculoskeletal System Nervous System Reproductive System Respiratory System Urinary System Dermatology System (Skin) Immune System
 Immune System")
23
There are many different presentations of obese patients… Some of them are Healthy But the others may already have many complications from obesity.

24
Examination

25
Examination: 1st impressions. Vital signs: PR RR BP and Temperature General examination. Size of thyroid size of abdominal organs e.g. liver… Heart and lung sounds.

26
Evaluation : Also you must evaluate the patient obesity by calculating BMI. BMI = weight (kg) / [ height (m) ]²
 / [ height (m) ]².")
27
BMI RangeWeight Classification Risk of Illness Less than 18.5 UnderweightIncreased 18.5 – 24.9 Ideal weightNormal 25 – 29.9 OverweightIncreased 30 – 39.9 ObeseHigh 40 – 50 Morbid obeseVery high 50 Or greater Super obeseExtremely high

28
Investigations

29
Laboratory Data:

30
ParameterNormal Range Blood glucose80-120 mg/dl Cholesterol< 200 mg/dl Triglycerides< 150 mg/dl HDL40 - 60 mg/dl LDL< 100 mg/dl Hemoglobin13-16 mg/dl Hematocrit36-44% TSH0.35-5.50 Cortisole5-25 am 3-16 pm µg/dl Serum iron40-140 mg/dl Uric acid(3.5-7.8) Hemoglobin A1c*4.8-6.3%
 Hemoglobin A1c* %")
31
Additional Tests : ECG x-ray U.S

32
Treatment of obesity

33
Treatment of obesity comes into three categories: 1-behavior modification. {diet and exercise} 2-pharmacotherapy 3-surgical intervention.

34
National institutes of health guidelines for treatment of overweight and obesity: surgeryEndoscp ic balloon pharmac otherapy Behavior mod. BMI range No Yes*25-26.9 No Yes* 27-29.9 NoYes 30-34.9 NoYes 35-39.9 YesYes*Yesyes40 or more comorbidities present *

35
Behavior modification: A multibillion dollar commercial industry Tow forms of modification : 1- diet 2- exercise Dietary modification is an effective means of inducing weight loss.

36
Dietary modification tow forms: Low calorie diet (LCD) Aims for an energy deficit ranging from 500 to 1000 kcal/day LCD is a low fat diet LCD Helps losing 0.5 kg/week That lead to a 10% weight loss over 6 months Very low calorie diet (VLCD) VLCD is high protein diet with less fat &no carbohydrate Limits energy intake to fewer than 800kcal/day VLCD helps losing 1-1.5 kg/week
 Aims for an energy deficit ranging from 500 to 1000 kcal/day LCD is a low fat diet LCD Helps losing 0.5 kg/week That lead to a 10% weight loss over 6 months Very low calorie diet (VLCD) VLCD is high protein diet with less fat &no carbohydrate Limits energy intake to fewer than 800kcal/day VLCD helps losing kg/week")
37
Cont….. Short term weight loss with VLCD is dramatic with some people losing up to 20kg in 3 months. But long term doesn’t differ from LCD VLCD require physician supervision

38
Increasing energy expenditure: exercise is very effective in preventing long term weight regain. At least,doing exercise 3 times /week for 45 minute Or doing 20 minute exercise each day

39
Pharmacotherapy: Currently tow drugs are used 1- sibutramine 2- orlistat

40
Sibutramine Appetite suppressant Mechanism of action is serotonin & norepinephrine uptake inhibitor 10 mg/day Side effect :tachycardia, hypertension, headache, and insomnia Long term 5%to 10% weight loss Weight regain happens after stopping the drug

41
Orlistat Potent inhibitor of lipase activity Binds fats Efficacy of the drug &its side effect increase with higher fat content in the food Side effect: fecal leakage, bloating,and increase flatulance. Long term 10% weight loss 120 mg/day 3 times a day

42
Surgical intervention: Must be psychologically stable and wiling to follow postoperative diet instruction No endocrine cause for obesity Surgical intervention work by decreasing energy intake Most common types 1- gastric banding 2-roux-en-y gastric bypass procedure

43
Adjustable gastric banding: Work by restrictive operations Creation of a proximal gastric pouch by inflatable band and placement of an access port 45% to 55% EBW over the first two years

44
Advantages of AGB Easy applied Day surgery Done Laparoscopically no complications

48
Disadvantage of AGB: Esophageal dilatation Gastric prolapse Band erosion

49
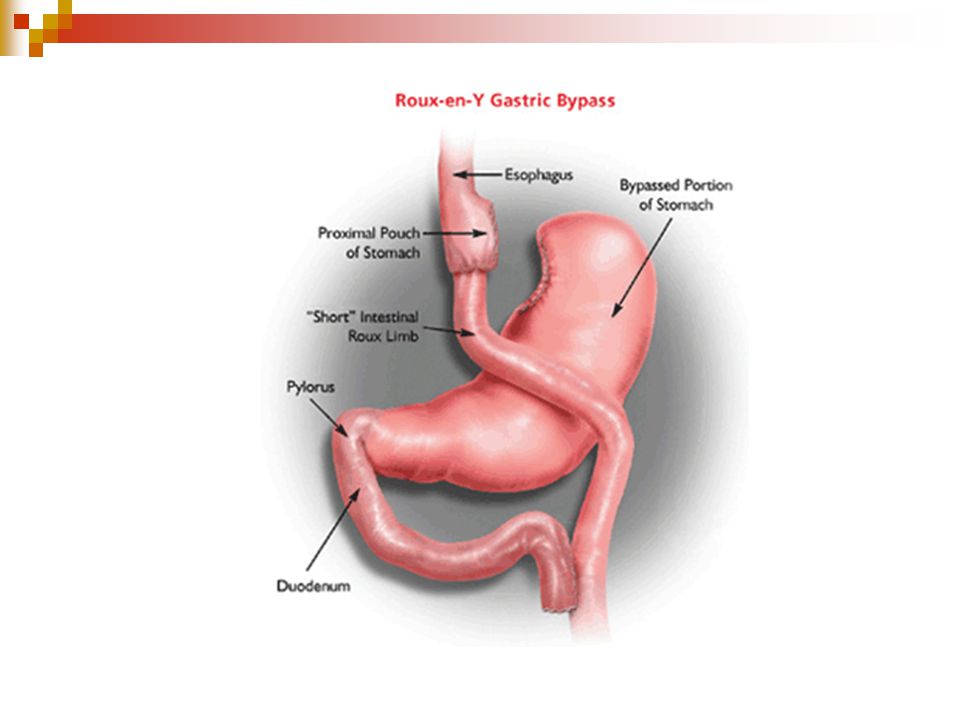
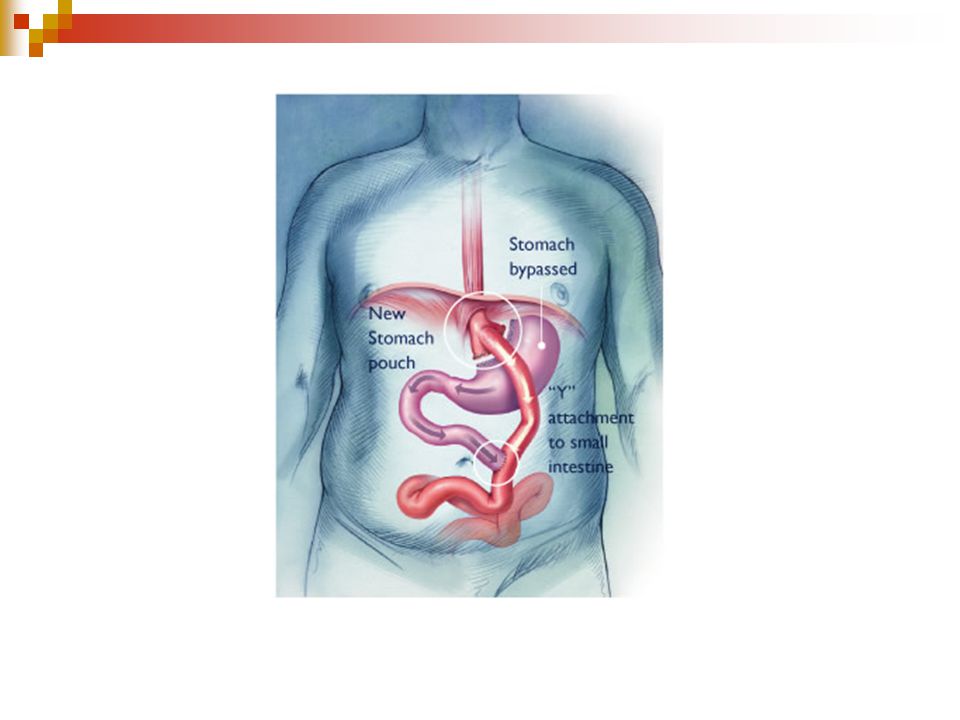
Roux-en-y gastric bypass procedure: Combine restrictive and malabsorptive operation Most common operative intervention in USA Work by creation of a small proximal gastric pouch with roux-en-y gastrojejunostomy 75% to 85% EBW within a couple years

52
Disadvantage of RNYGB Anastomotic leak 20% Stricture 10% Nutritional disturbances Especially, vitamine B12,iron &calcium cholelithiasis

Similar presentations