Download presentation
Presentation is loading. Please wait.

1
Respiratory System Ch 22

2
Breathing (Pulmonary Ventilation) External Respiration
4 PROCESSES Breathing (Pulmonary Ventilation) External Respiration Internal Respiration Cellular Respiration
 External Respiration. Internal Respiration. Cellular Respiration.")
3
Sinus Cavity act as resonance chambers for speech
mucosa warms and moistens the incoming air lightens facial bones

4
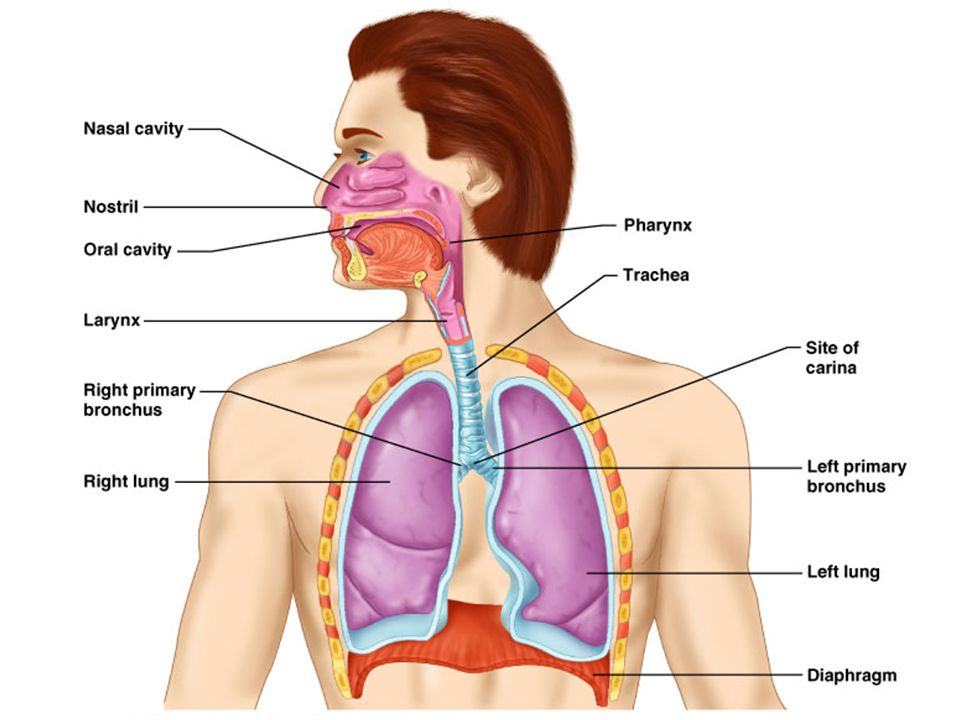
Pharynx Connects nasal cavity and mouth to larynx and esophagus
1) nasopharynx- air passage Eustatian tube Adenoids (pharyngeal) tonsils- mass of lymphoid tissue traps and destroys pathogens produces lymphocytes helps fight infection 2) oropharynx- serves as a common conduit for air and food palatine and lingual tonsils 3) laryngopharynx- accommodates both ingested food and air located at junction where tracheae and esophagus splits continuous with esophagus
 nasopharynx- air passage. Eustatian tube. Adenoids (pharyngeal) tonsils- mass of lymphoid tissue. traps and destroys pathogens. produces lymphocytes. helps fight infection. 2) oropharynx- serves as a common conduit for air and food. palatine and lingual tonsils. 3) laryngopharynx- accommodates both ingested food and air. located at junction where tracheae and esophagus splits. continuous with esophagus.")
5
Pharynx Epiglottis- flexible elastic cartilage
attached to the wall of the pharynx near the base of the tongue Larynx- voice box; thyroid cart. that attaches to hyoid bone superior and cricoid inferior Provides open airway Junction for food and air Voice production

6
Pharynx Nasopharynx Oropharynx Laryngopharynx

8
Olfactory epithelium Olfactory tract Olfactory bulb Nasal conchae Route of inhaled air

9
Trachea 16 C-shaped rings of hyaline cartilage (thyroid +cricoid + tracheal cartilage's, includes epiglottis (elastic cart) make up larynx Function- hold trachea open Laryngitis- inflammation of the vocal cords resulting in inability to speak; due to voice overuse, very dry air, bacterial infection, and inhalation of irritating chemicals

10
The Trachea lumen posterior anterior esophagus hyaline cartilage ring
Mucus membrane submucosa adventitia anterior

11
Trachea

12
The Trachea

13
Epithelial Lining of the Trachea
mucus cilia

14
Vocal Cords True vocal cords are inferior to false vocal cords
Sound is produced when expelled air is passing through the larynx over the vocal cords

15
Lungs

16
Alveoli

17
Alveoli

18
Alveoli

19
Thoracic Cavity

20
Thoracic Cavity

21
Partial Pressure Gradients

22
Ventilation-Perfusion Coupling

23
Mechanics of Breathing
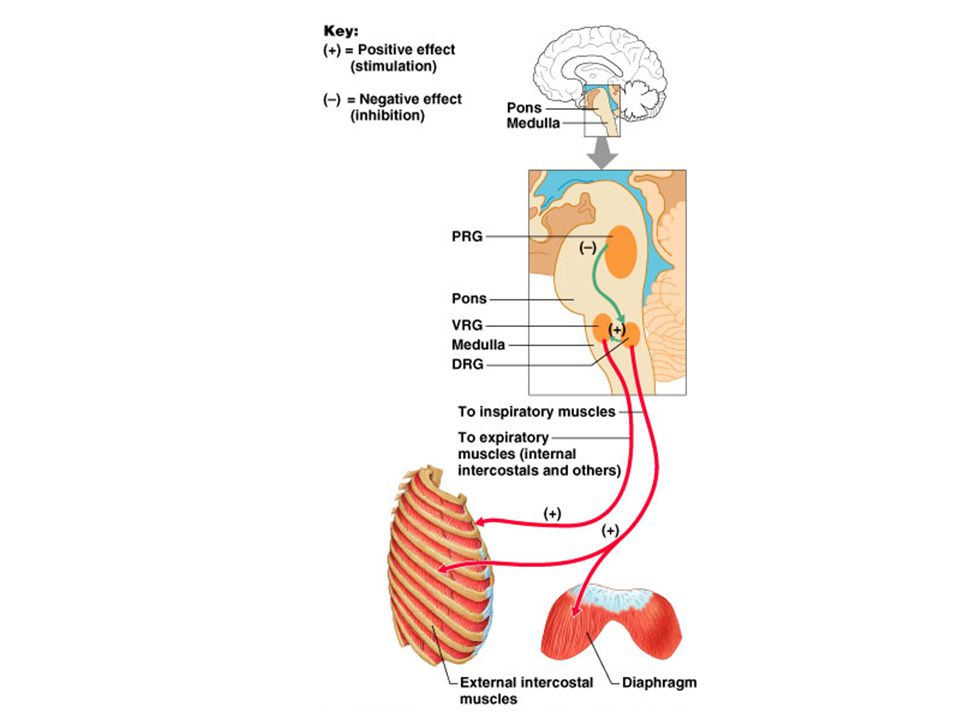
2 muscles involved with breathing: external intercostal muscles diaphragm Breathing controlled by: phrenic nerve from medulla pons

24
Mechanics of Breathing

25
Lung Ventilation Negative pressure draws air in Inspiration 760 mm Hg

26
Lung Ventilation Positive pressure forces air out 768 mm Hg Expiration

27
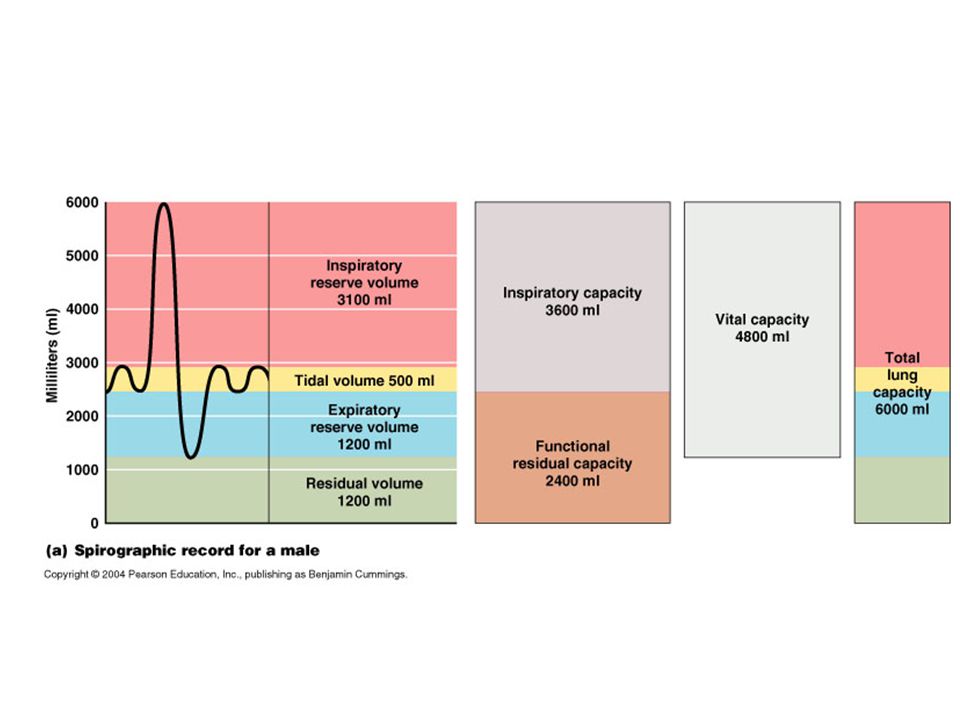
Lung Volumes Tidal Volume- 500 ml Vital Capacity- 4800 ml
Residual Volume- 1200ml Total Lung Capacity ml IRV ml ERV- 1200ml Dead Space- 150 ml TV- tidal volumes- normal breathing ~500 ml air IRV- inspiratory reserve volume- amount of air that can be forcefully inhaled after a normal tidal volume inhalation ~3100 ml ERV- expiratory reserve volume- amount of air that can be forcefully exhaled after a normal tidal volume of exhalation ~1200 ml VC- vital capacity- total amount of exchangeable air; maximum amount of air that can be forcefully exhaled after a maximal inspiration ml VC=TV + IRV +ERV RV- residual volume = air that helps keep alveoli open and prevents lung from collapsing ~1200 ml TLC- total lung capacity = TV+IRV+ERV+RV Dead space- air that never contributes to gas exchange ~ conduit ~150 ml; throat, alveoli, nasal passage What factors affect lung volume?

29
What happens to TV, IRV, ERV, & VC during exercise?
IRV and ERV TLC and VC- doesn't change

30
Breathing Centers in the Brain

32
Regulation of Breathing
medulla oblongata pons phrenic CO2 and H+ triggers breathing reflex in medulla, not presence of O2 vagus

34
Restrictive vs Obstructive Air Flow
Restrictive- more diff. to get air in to lungs Loss of lung tissue Decrease in lungs ability to expand Decrease in ability to transfer O2 and CO2 in blood Diseases: Fibrosis, sarcoidosis, muscular disease, chest wall injury, pneumonia, lung cancer, pregnancy, obesity VC, TLC, RV, FRC

35
Restrictive vs Obstructive Air Flow
Obstructive- more diff. to get air out of lungs Airway narrows Increase in time it takes to empty lungs Diseases: Emphysema, chronic bronchitis, asthma VC, TLC, RV, FRC

36
Chronic Obstructive Pulmonary Diseases

37
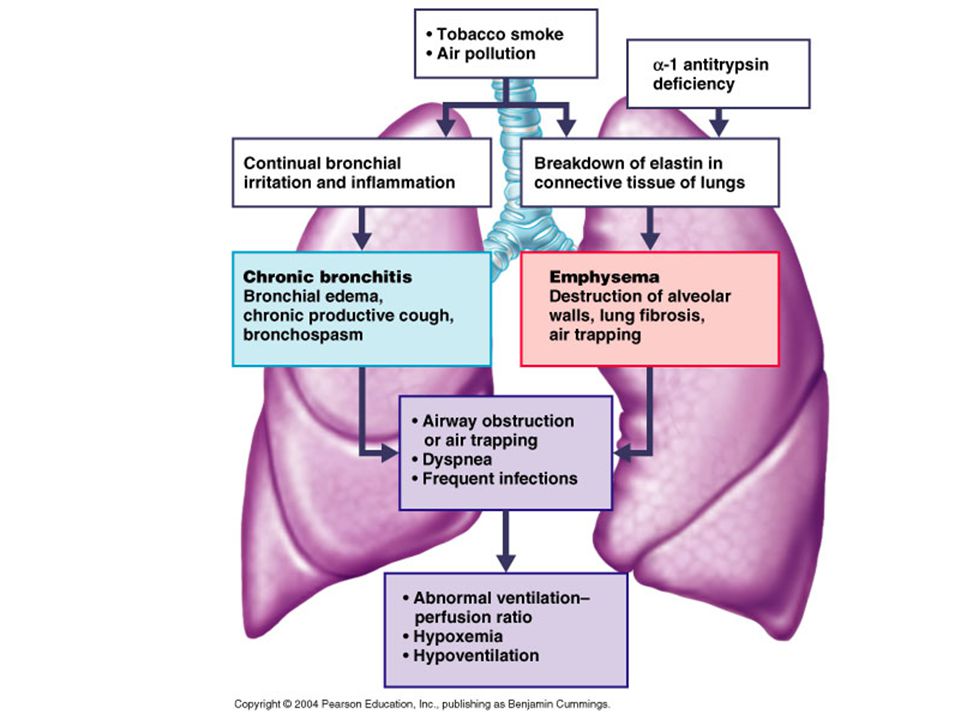
COPD Chronic bronchitis- (obstructive) inhaled irritants lead to chronic excessive mucous production and inflammation and fibrosis of that mucosa; the amt of air that can be inhaled; use bronco- dilators and inhalers Emphysema- (obstructive and restrictive) enlargement of alveoli; alveolar tissue is destroyed resulting in fewer and larger alveoli; inefficient air exchange; smoker's disease; amt of air that can be exhaled Asthma- (obstructive disorder) cold, exercise, pollen and other allergens; from the number of asthmatic deaths doubles
 inhaled irritants lead to chronic excessive mucous production and inflammation and fibrosis of that mucosa; the amt of air that can be inhaled; use bronco- dilators and inhalers. Emphysema- (obstructive and restrictive) enlargement of alveoli; alveolar tissue is destroyed resulting in fewer and larger alveoli; inefficient air exchange; smoker s disease; amt of air that can be exhaled. Asthma- (obstructive disorder) cold, exercise, pollen and other allergens; from the number of asthmatic deaths doubles.")
38
COPD Tuberculosis (TB)- (restrictive) infectious disease cause by bacterium Mycobacterium tuberculosis. Spread through air borne bacteria from infected person's cough. Total lung capacity declines Symptoms: fever night sweats, wt. loss, racking cough, and spitting up blood Polio- TLC declines (restrictive) Eliminated in U.S. and Western Hemisphere Still exists in Africa Lung cancer- promoted by free radicals and other carcinogens; very aggressive and metastasizes rapidly
- (restrictive) infectious disease cause by bacterium Mycobacterium tuberculosis. Spread through air borne bacteria from infected person s cough. Total lung capacity declines. Symptoms: fever night sweats, wt. loss, racking cough, and spitting up blood. Polio- TLC declines (restrictive) Eliminated in U.S. and Western Hemisphere. Still exists in Africa. Lung cancer- promoted by free radicals and other carcinogens; very aggressive and metastasizes rapidly.")
39
Smoker’s lung Normal lung

40
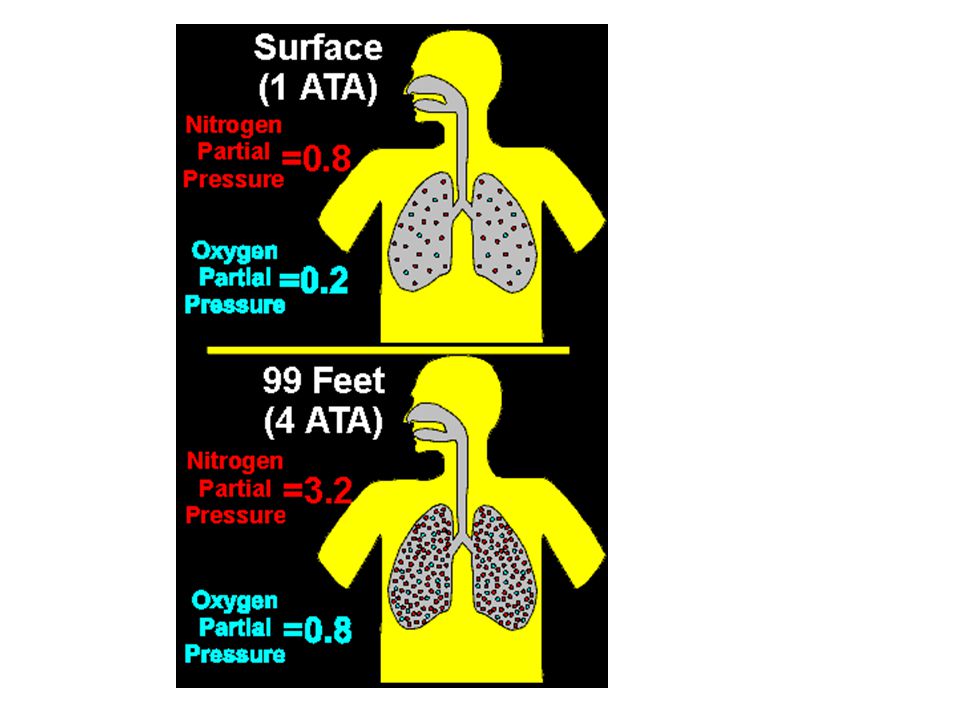
Dalton's Law of Partial Pressure
The total pressure of a gas exerted by a mixture of gas is the sum of the gases exerted independently. Air % partial pressure (mm Hg) N O CO H2O Total Dalton's law states that the individual gases of any gas mixture will have the same pressure alone or as part of the mixture. Thus, at sea level, the oxygen component of air by itself will support a mercury column mm high, and the nitrogen component will support a mercury column mm high. At depth all pressures increase, for both air as a mixture and for its component gases. For example, a doubling of ambient air pressure, which occurs at just 33 fsw, will double the partial pressure of oxygen, nitrogen, and other component gases. At 66 fsw, the ambient pressure is tripled, along with the partial pressure of oxygen, nitrogen and other gases inhaled at that depth. Partial pressure is directly related to its % in the total gas mixture. E.g., at 1 atm PO2 = 159 mm Hg
 N O CO H2O Total Dalton s law states that the individual gases of any gas mixture will have the same pressure alone or as part of the mixture. Thus, at sea level, the oxygen component of air by itself will support a mercury column mm high, and the nitrogen component will support a mercury column mm high. At depth all pressures increase, for both air as a mixture and for its component gases. For example, a doubling of ambient air pressure, which occurs at just 33 fsw, will double the partial pressure of oxygen, nitrogen, and other component gases. At 66 fsw, the ambient pressure is tripled, along with the partial pressure of oxygen, nitrogen and other gases inhaled at that depth. Partial pressure is directly related to its % in the total gas mixture. E.g., at 1 atm PO2 = 159 mm Hg.")
41
Henry's Law When a mixture of gas is in contact w/a liquid, each gas will dissolve in the liquid in proportion to its partial pressure. Gasses can go in and out of solution e.g., open soda, get CO2 bubbles (CO2 is under pressure)
")
42
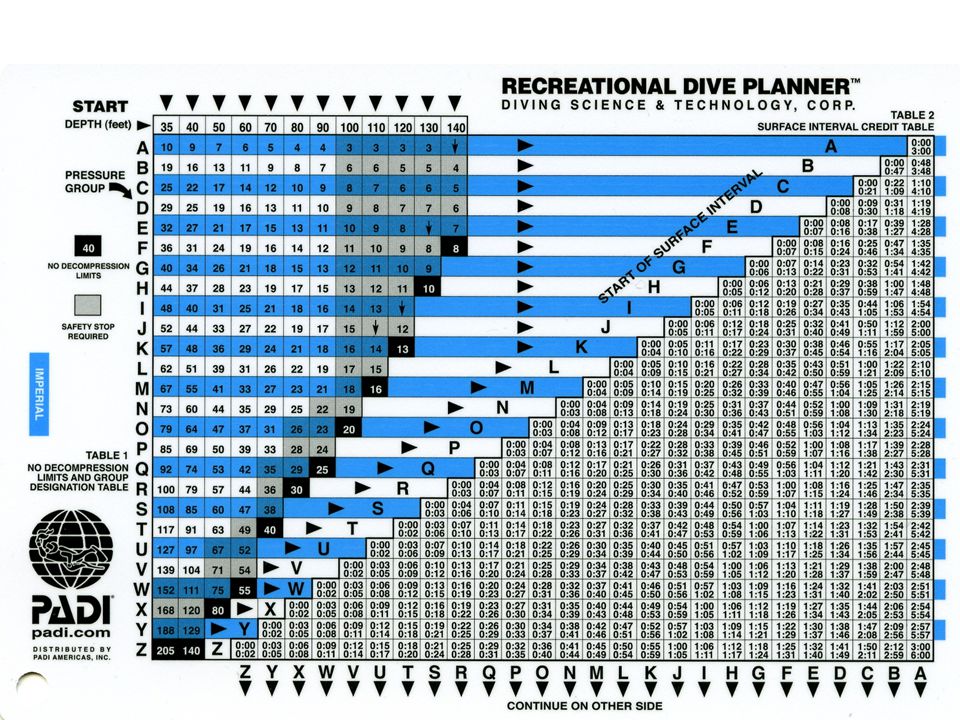
Decompression Sickness
It is caused when N2 enters the blood circulation and the tissues. When extra N2 leaves the tissues, large bubbles form. N2 bubbles can travel throughout the system and into the lungs and blood routes. Treatment: hyperbaric chamber The increased pressure of each gas component at depth means that more of each gas will dissolve into the blood and body tissues, a physical effect predicted by Henry's Law. To review, Henry's law states that the amount of gas dissolving into any liquid or tissue with which it is in contact is proportional to the partial pressure of that gas. Inhaled gases are in close contact with blood entering the lungs. Hence, the greater the partial pressure of any inhaled gas, the more that gas will diffuse into the blood. Together, Boyle's and Henry's laws explain why, as a diver descends while breathing compressed air: 1) inhaled PO2 and PN2 increase and 2) the amount of nitrogen and oxygen entering the blood and tissues also increase.
 inhaled PO2 and PN2 increase and. 2) the amount of nitrogen and oxygen entering the blood and tissues also increase.")
45
Hyperbaric Chamber

46
Erythrocytes Function- transport respiratory gases
Lack mitochondria. Why?

47
Hemoglobin Structure Hemoglobin- quaternary structure
2 chains and 2 chains Hemoglobin Structure 1 RBC contains 250 million hemoglobin molecules

48
Uptake of Oxygen by Hemoglobin in the Lungs
O2 binds to hemoglobin to form oxyhemoglobin High Concentration of O2 in Blood Plasma High pH of the Blood Plasma oxyhemoglobin O2

49
O2 pickup CO2 release

50
Unloading of Oxygen from Hemoglobin in the Tissues
When O2 is releaseddeoxyhemoglobin Low Concentration of O2 in Blood Plasma Lower pH of the Blood Plasma

51
O2 release CO2 pickup

52
Carbon Dioxide Chemistry in the Blood
CO2 + H2O H2CO3 HCO H+ bicarbonate ion carbonic acid enzyme = carbonic anhydrase

53
Transport of Carbon Dioxide from the Tissues to the Lungs
60-70% as bicarbonate dissolved in the plasma (slow reaction) 7-10% dissolved in the plasma as CO2 20-30% bound to hemoglobin as HbCO2 CO2 + hemoglobin HbCO2
 7-10% dissolved in the plasma as CO % bound to hemoglobin as HbCO2. CO2 + hemoglobin HbCO2.")
54
Haldane Effect Haldane Effect- the amt of CO2 transported in the blood is markedly affected by the degree of oxygenation of the blood The lower the PO2 and hemoglobin saturation w/O2, the more CO2 that can be carried by the blood.

55
Carbon Monoxide Poisoning
CO poisoning (hypoxemia hypoxia) CO binds 200x more readily w/hemoglobin acts as a competitive inhibitor symptoms: cherry red lips, confused, headache does not produce characteristic signs of hypoxia (cyanosis and respiratory distress) treatment: hyperbaric chamber
 CO binds 200x more readily w/hemoglobin. acts as a competitive inhibitor. symptoms: cherry red lips, confused, headache. does not produce characteristic signs of hypoxia (cyanosis and respiratory distress) treatment: hyperbaric chamber.")
56
Mammalian Dive Reflex Heart rate slows
Blood flow to extremities constricted Blood and water allowed to pass through organs and circulatory walls to chest cavity. The first two items begin to happen as soon as the face hits cold water. The slowing heart rate is almost instantaneous, the constricted blood flow happens more gradually. Both responses are more extreme with more extreme temperatures. The slowed heart rate is generally a useful feature as it actively serves to conserve oxygen depletion and increase the available time underwater without dramatically harming performance. Yeah! You’re holding your breath, so obviously there are limits to the effectiveness! The decreased blood flow provides more of a long-term (minutes-hours) survival benefit, but is detrimental to performance. If you were diving for food, you’d quickly find that your limbs turn into numb rocks in cold water. The third response is a bit more scary. Essentially, the body intentionally allows fluid to fill the lungs and chest cavity to prevent organs from being crushed from extreme pressure. For surface dwelling mammals, this serves a survival function. It only kicks in as depths become extreme. Mammalian Dive Reflex First observed in sea mammals, this reflex (MDR) is effectively what allows freedivers to do what they do. It wasn't until the 1950's that this reflex was shown to be possessed by people and not just whales, seals and our cretacious cousins, the dolphins. Prior to this discovery and even in the era of Jaques Mayol, scientists thought it was impossible for a freediver to dive much over 40m without being killed. The MDR consists of a number of immediate physiological changes: bradycardia (the slowing of the heart), splenic contraction and blood shift. a) Bradycardia (slowing of the heart) Because the heart, as the biggest muscle in the body, uses oxygen every time it beats, the slower it beats, the less oxygen it uses, allowing the diver to stay underwater for extended periods. b) Splenic contraction Water pressure squeezes the spleen, reducing its size by up to 20%. This effectively squeezes blood rich in red blood-cells into the circulatory system, increasing hemoglobin concentration by up to 10%. c) Blood shift Blood shift, or "blood shunt", is a movement of blood from the peripheral areas such as the limbs, to the core areas of heart, lungs and brain. It is caused through peripheral vasoconstriction of skin vessels, as well as big intra-thoracic vessels. For these organs, oxygen is an obvious priority. So by this redistribution of blood, and therefore oxygen, from the nonessential areas to those areas involved in maintaining consciousness, the freediver is able to stay conscious longer. Another advantage offered by blood shift is that, because there is less blood flowing to the legs, when they are used during fining they are forced to work primarily anaerobically and therefore use less oxygen than they otherwise would. Blood shift also allows divers do dive well beyond residual volume (30-40m) without suffering "lung squeeze" as the lungs pool with blood, thereby mitigating the increasing vacuum effect caused by ribs inability to flex inwards and the diaphragm to move up as the pressure differential between the air in the lungs and the surrounding water increase. Blood does not actually enter the lungs air space. Rather it is the capillaries that intrude into the lungs' airspace and expand as they become engorged with blood. This is termed "pulmonary erection". Only if negative pressure becomes extreme will plasma and then even blood (pulmonary edema) enter the airspace and be coughed up. Martin Stepanek, during static apnea alone, is said to have such a strong blood shift that his legs and arms go visibly white and his torso red. This shows that although blood shift is usually triggered by pressure, it is also triggered by the "breath-hold reflex", the two reflexes being inextricably linked. The degree of dive reflex: It varies from person to person. Fortunately it is trainable to a large degree. The more often you dive, the more accustomed the body gets to engage the various mechanisms involved. It's almost as if the brain, knowing what is about to happen next, can quicker and more effectively trigger the necessary physiological chances. A simple static then becomes enough to trigger the entire MDR. Facial immersion: Apart from increased ambient hydrostatic pressure and breath-holding, the other very important trigger of the MDR is facial immersion in water. Dr Erica Schagatay found that the main trigger was cold water, colder the better. She also managed to show that the areas which needed to be exposed to the cold water were on the face, specifically nerves around the eyes and upper lip. This is the reason behind doing a warm-up static face down and without a mask before a big dive, and if there is a thermocline available, a static bellow the thermocline without a mask. It's also the reason why many freedivers prefer wearing goggles over masks during statics.
 survival benefit, but is detrimental to performance. If you were diving for food, you’d quickly find that your limbs turn into numb rocks in cold water. The third response is a bit more scary. Essentially, the body intentionally allows fluid to fill the lungs and chest cavity to prevent organs from being crushed from extreme pressure. For surface dwelling mammals, this serves a survival function. It only kicks in as depths become extreme. Mammalian Dive Reflex. First observed in sea mammals, this reflex (MDR) is effectively what allows freedivers to do what they do. It wasn t until the 1950 s that this reflex was shown to be possessed by people and not just whales, seals and our cretacious cousins, the dolphins. Prior to this discovery and even in the era of Jaques Mayol, scientists thought it was impossible for a freediver to dive much over 40m without being killed. The MDR consists of a number of immediate physiological changes: bradycardia (the slowing of the heart), splenic contraction and blood shift. a) Bradycardia (slowing of the heart) Because the heart, as the biggest muscle in the body, uses oxygen every time it beats, the slower it beats, the less oxygen it uses, allowing the diver to stay underwater for extended periods. b) Splenic contraction. Water pressure squeezes the spleen, reducing its size by up to 20%. This effectively squeezes blood rich in red blood-cells into the circulatory system, increasing hemoglobin concentration by up to 10%. c) Blood shift. Blood shift, or blood shunt , is a movement of blood from the peripheral areas such as the limbs, to the core areas of heart, lungs and brain. It is caused through peripheral vasoconstriction of skin vessels, as well as big intra-thoracic vessels. For these organs, oxygen is an obvious priority. So by this redistribution of blood, and therefore oxygen, from the nonessential areas to those areas involved in maintaining consciousness, the freediver is able to stay conscious longer. Another advantage offered by blood shift is that, because there is less blood flowing to the legs, when they are used during fining they are forced to work primarily anaerobically and therefore use less oxygen than they otherwise would. Blood shift also allows divers do dive well beyond residual volume (30-40m) without suffering lung squeeze as the lungs pool with blood, thereby mitigating the increasing vacuum effect caused by ribs inability to flex inwards and the diaphragm to move up as the pressure differential between the air in the lungs and the surrounding water increase. Blood does not actually enter the lungs air space. Rather it is the capillaries that intrude into the lungs airspace and expand as they become engorged with blood. This is termed pulmonary erection . Only if negative pressure becomes extreme will plasma and then even blood (pulmonary edema) enter the airspace and be coughed up. Martin Stepanek, during static apnea alone, is said to have such a strong blood shift that his legs and arms go visibly white and his torso red. This shows that although blood shift is usually triggered by pressure, it is also triggered by the breath-hold reflex , the two reflexes being inextricably linked. The degree of dive reflex: It varies from person to person. Fortunately it is trainable to a large degree. The more often you dive, the more accustomed the body gets to engage the various mechanisms involved. It s almost as if the brain, knowing what is about to happen next, can quicker and more effectively trigger the necessary physiological chances. A simple static then becomes enough to trigger the entire MDR. Facial immersion: Apart from increased ambient hydrostatic pressure and breath-holding, the other very important trigger of the MDR is facial immersion in water. Dr Erica Schagatay found that the main trigger was cold water, colder the better. She also managed to show that the areas which needed to be exposed to the cold water were on the face, specifically nerves around the eyes and upper lip. This is the reason behind doing a warm-up static face down and without a mask before a big dive, and if there is a thermocline available, a static bellow the thermocline without a mask. It s also the reason why many freedivers prefer wearing goggles over masks during statics.")
57
Hyperventilation Short term, rapid, deep breathing beyond the need for the activity Lowers the level of CO2 in blood (hypocapnia or hypocarbia) Short term, rapid, deep breathing beyond the need for the activity Lowers the level of CO2 in blood (hypocapnia or hypocarbia)
")
58
Shallow Water Blackout

59
INQUIRY Identify the lipoprotein molecule that reduces surface tension within the alveoli so they do not collapse during exhalation. Even after the most forceful exhalation, a certain volume of air remains in the lungs. What is the volume of air called? Describe the physical structure of alveoli. What structures warm and moisten incoming air? What body cavity are the lungs located? What tissue lines the lungs? What stimulates the breathing response? Calculate total lung capacity given: RV= 1000, TV = 500, ERV = 1100, IRV = 2500, VC= 4100

Similar presentations









 2. Nasal cavity. Nasal cavity is lined with ciliated, mucosal epithelial tissue.>")









