Download presentation
Presentation is loading. Please wait.

1
TB vaccines and diagnostics

2
Introduction

3
An estimated 15 million active cases, leading to….. An estimated 9 million new infections Approx 2 million deaths Approx 2 Billion USD in direct control costs And an uncounted indirect cost in lost lives and productivity Global burden of tuberculosis (The economist’s view)
.")
4
Tuberculosis: Transmission Exposure/Infection 10% Clearance 70% TB Infection (2 bill, ~ 9 mill/yr) Primary infection Death ~2 mill 30% Latent TB 90% Reactivation 5-15% First 2yrs highest chance of developing TB disease Treatment with several drugs for 6 months or more can cure more than 95% of patients If not treated 60 % dies
 Primary infection Death ~2 mill 30% Latent TB 90% Reactivation 5-15% First 2yrs highest chance of developing TB disease Treatment with several drugs for 6 months or more can cure more than 95% of patients If not treated 60 % dies")
5
TB At present tuberculosis kills more people than any other infectious disease about 3 million people a year, including almost 300,000 children under 15, and is producing over 7,000 deaths and over 24,000 new cases every day. No new drugs have been added to the first-line treatment regimen for TB for >30 yrs. There is a clear synergy between M. tuberculosis and HIV, and active TB increases HIV-related immunodeficiency and mortality. TB remains the largest attributable cause of death in HIV- infected individuals and is responsible for 32% of the deaths of HIV-infected individuals in Africa. The neediest populations, in countries where TB incidence is highest, do not have access to treatment and, furthermore, in many cases, anti-TB drugs are ineffective.

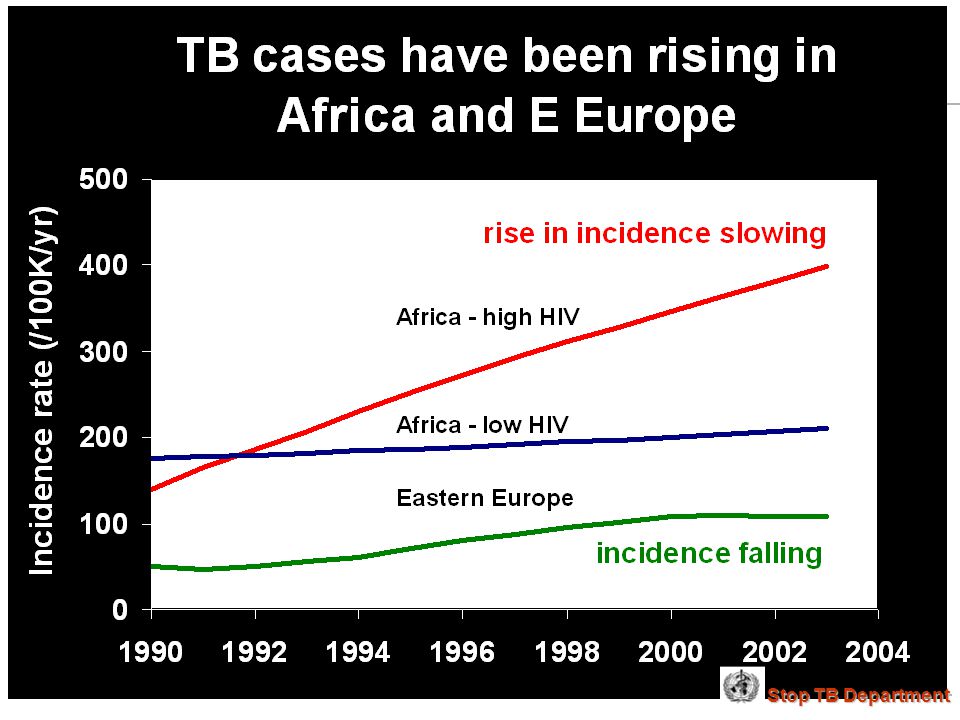
6
Highest TB rates per capita are in Africa linked to HIV/AIDS 25 to 49 50 to 99 100 to 299 < 10 10 to 24 300 or more No Estimate per 100 000 population The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. © WHO 2002 Stop TB Department

8
Exposure Health y (95%) Year 1 Year 2 Year 3 thereafter TB (5%) Health y (92%) TB (3%) Health y (91%) TB (1%) Healthy (approx. 90%) TB (less than 0.1%/year) Development of Tuberculosis (the clinician’s view)
 TB (less than 0.1%/year) Development of Tuberculosis (the clinician’s view).")
9
Early bacterial growth arrested at early time point. May (or may not) result in latent infection Initial exposure Early bacterial growth not contained. Leads to clinical illness Subsequent bacterial growth contained. Symptoms abate but latent infection established. Bacterial growth not contained. Progressive disease unless treated Reactivation of latent infection at a later point in life 33% 67% 9% 24% 2% Remain healthy but latently infected 22% These individuals do not apparently skin-test convert These individuals generally skin-test convert. They often have characteristic patterns on X-ray. Response to infection (the immunologist’s view)
 result in latent infection Initial exposure Early bacterial growth not contained. Leads to clinical illness Subsequent bacterial growth contained. Symptoms abate but latent infection established. Bacterial growth not contained. Progressive disease unless treated Reactivation of latent infection at a later point in life 33% 67% 9% 24% 2% Remain healthy but latently infected 22% These individuals do not apparently skin-test convert These individuals generally skin-test convert. They often have characteristic patterns on X-ray. Response to infection (the immunologist’s view).")
10
TB vaccines (BCG) A 60-year follow-up study of American Indians reported the long- term efficacy of BCG to be 52%. The reasons for the low efficacy of the BCG vaccine may be generic differences in the BCG strains, differences in immunological properties of study populations or exposure to environmental factors such as mycobacteria. Today, most of the world's population is vaccinated with BCG. It is generally accepted that BCG protects against childhood TB but this immunity wanes with age, resulting in no or insufficient protection against TB. Among new vaccine candidates are live attenuated Mycobacterium tuberculosis vaccines, recombinant BCG, DNA vaccines, subunit vaccines and fusion proteins with novel adjuvants and delivery systems. Some of these vaccines are now in clinical trials.

11
Stop TB Department

12
TB-specific antigens M. tuberculosis Atypical mycobacteria BCG M.tuberculosis specific Antigens (100+): ESAT-6 Common mycobacterial Antigens (1000+) Ag85A/B Rv2031c Shared TB complex Antigens (4000+)
: ESAT-6 Common mycobacterial Antigens (1000+) Ag85A/B Rv2031c Shared TB complex Antigens (4000+).")
13
TB diagnostics Left untreated, each person with active TB disease will infect on average between 10 and 15 people every year.

14
Risk of TB in ESAT+ healthy contacts from Ethiopia Doherty et al., JCM, Feb. 2002 PPD: skin test (Purified Protein Derivative)
.")
15
High ESAT-6 immune reactivity reflects high levels of M. tuberculosis replication CFU Time after infection “positivity” threshold People who fail to control bacterial replication become ESAT+ and get TB People who fail to control initial bacterial replication become ESAT+, but if they control later infection, become latently infected People who control initial bacterial replication remain ESAT-, and may or may not be latently infected “Clinical disease” threshold

16
Early bacterial growth arrested at early time point. May (or may not) result in latent infection Initial exposure Early bacterial growth not contained. Leads to clinical illness Subsequent bacterial growth contained. Symptoms abate but latent infection established. Bacterial growth not contained. Progressive disease unless treated Reactivation of latent infection at a later point in life 33% 67% 9% 24% 2% Remain healthy but latently infected 22% These individuals do not apparently skin-test convert or become ESAT-6 positive These individuals generally skin-test convert and become ESAT-6 positive. They often have characteristic patterns on X-ray. Immunologically these individuals tend to express elevated levels of IL-4 and in advanced disease, decreased IFN- and IL-12 Immunologically, these individuals tend to express elevated levels of IFN- and IL-12, and while IL-4 often remains slightly increased, its antagonist IL-4 2 is greatly increased Immunologically, little is known about these individuals as they cannot be distinguished from uninfected individuals Response to infection (the immunologist’s view)
 result in latent infection Initial exposure Early bacterial growth not contained. Leads to clinical illness Subsequent bacterial growth contained. Symptoms abate but latent infection established. Bacterial growth not contained. Progressive disease unless treated Reactivation of latent infection at a later point in life 33% 67% 9% 24% 2% Remain healthy but latently infected 22% These individuals do not apparently skin-test convert or become ESAT-6 positive These individuals generally skin-test convert and become ESAT-6 positive. They often have characteristic patterns on X-ray. Immunologically these individuals tend to express elevated levels of IL-4 and in advanced disease, decreased IFN- and IL-12 Immunologically, these individuals tend to express elevated levels of IFN- and IL-12, and while IL-4 often remains slightly increased, its antagonist IL-4 2 is greatly increased Immunologically, little is known about these individuals as they cannot be distinguished from uninfected individuals Response to infection (the immunologist’s view).")
17
Acute infection Latent infection Expression of early phase Expression of late phase genes genes such as Ag85 such as -crystallin and and ESAT-6 the DosR regulon CFU Acute Disease Reactivation of infection Years after exposure 1-34-50 Elimination? Latent infection Immune conversion Latency? Bacterial response to infection

18
10 100 1000 10000 TBHHCLTBI p<0.001 Rv2031c response in clinical groups 10 100 1000 10000 TBHHCLTBI ESAT-6 response in clinical groups IFN- (pg/ml) Alteration of antigen recognition as disease progresses (ET)
 Alteration of antigen recognition as disease progresses (ET)")
19
Alteration of antigen recognition as disease progresses (Ga and NL) Slope of linear regression no. of spots from ESAT-6 stimulation vs Rv2031c Slope of linear regression no. of spots from ESAT-6 stimulation vs Rv2031c Slope of linear regression IFN- from ESAT-6 stimulation vs Rv2031c

20
A lowered ratio of ESAT-6 immune reactivity to Rv2031c reactivity reflects a shift from acute to latent TB CFU Time after infection “positivity” threshold People who fail to control bacterial replication become ESAT+ and get TB People who fail to control initial bacterial replication become ESAT+, but if they control later infection, become latently infected People who control initial bacterial replication remain ESAT-, and may or may not be latently infected “Clinical disease” threshold ESAT-6Rv2031c ESAT-6Rv2031c ESAT-6Rv2031c

21
Early bacterial growth arrested at early time point. May (or may not) result in latent infection Initial exposure Early bacterial growth not contained. Leads to clinical illness Subsequent bacterial growth contained. Symptoms abate but latent infection established. Bacterial growth not contained. Progressive disease unless treated Reactivation of latent infection at a later point in life 33% 67% 9% 24% 2% Remain healthy but latently infected 22% These individuals do not apparently skin-test convert or become ESAT-6 positive These individuals generally skin-test convert and become ESAT-6 positive. They often have characteristic patterns on X-ray. Immunologically these individuals tend to express elevated levels of IL-4 and in advanced disease, decreased IFN- and IL-12. They weakly recognise Rv2031c Immunologically, these individuals tend to express elevated levels of IFN- and IL-12, and while IL-4 often remains slightly increased, its antagonist IL-4 2 is greatly increased. They strongly recognise Rv2031c Immunologically, little is known about these individuals as they cannot be distinguished from uninfected individuals Response to infection (the immunologist’s view)
 result in latent infection Initial exposure Early bacterial growth not contained. Leads to clinical illness Subsequent bacterial growth contained. Symptoms abate but latent infection established. Bacterial growth not contained. Progressive disease unless treated Reactivation of latent infection at a later point in life 33% 67% 9% 24% 2% Remain healthy but latently infected 22% These individuals do not apparently skin-test convert or become ESAT-6 positive These individuals generally skin-test convert and become ESAT-6 positive. They often have characteristic patterns on X-ray. Immunologically these individuals tend to express elevated levels of IL-4 and in advanced disease, decreased IFN- and IL-12. They weakly recognise Rv2031c Immunologically, these individuals tend to express elevated levels of IFN- and IL-12, and while IL-4 often remains slightly increased, its antagonist IL-4 2 is greatly increased. They strongly recognise Rv2031c Immunologically, little is known about these individuals as they cannot be distinguished from uninfected individuals Response to infection (the immunologist’s view).")
22
Summary Immunity to M. tuberculosis is dependent on the generation of Th1 immunity, particularly IL-12, IFN-g and TNF-a As the bacteria persists in the face of this Th1 response, it begins to alter its proteome towards a pattern characteristic of latency, downregulating some antigens, upregulating others At the same time, a Th2 response seems to develop Susceptibility to infection therefore appears to correlate not so much with inability to generate a Th1 response, as with inability to maintain it long term, or perhaps inability to direct it to relevant antigens We are starting to see evidence that M. tuberculosis-derived antigens are driving some of this Th2 response

23
Identification of CD8+ epitopes Vaccines4TB Vaccines against tuberculosis are urgently needed. CD4 T cell responses play a major role in the generation of acquired immunity against M. tuberculosis. However, it is increasingly recognised that CD8 cytotoxic T cells (CTL) also contribute to optimal host defence against mycobacteria. Unfortunately, relatively few CTL responses against TB have been identified. http://ec.europa.eu/research/health/poverty- diseases/projects/110_en.htm Sheila Tang
 also contribute to optimal host defence against mycobacteria. Unfortunately, relatively few CTL responses against TB have been identified. diseases/projects/110_en.htm Sheila Tang.")
24
Cellular immune response Tubercle bacilli enter aveoli Infect* macrophages Within few weeks Th1 immune response CD4+/CD8 + T cells Recruit to lung Cytokines: IL-2, TNFa and IFN-y Tubercle bacilli MACROPHAGE Lysosome +TB ER TB peptide TCR CD8 T cells IFN-g

25
Granulomas prevent spread of infection by confining bacteria within a compact collection of several types of immune cells and activated macrophages Role of these cells: specific ways to isolate inhibit the replication of, and destroy the bacteria Cellular immune response Bacilli engulfed by macrophages Replicate within the macrophages 2-3 weeks before spreading throughout the body 95% contain the bacteria in macrophages But due to Mtb. complex waxy cell wall the bacteria are protected inside the macrophages http://www.granuloma.homestead.com/tb_microscopic.html

26
TB genome. Where to look?

27
Epitope Prediction TBVAC epitopes(14) Proteins with CD8 epitopes(25) Proteins from vaccine trials (Michel Klein WP3) Selected in proteins - previously described by other groups to have CTL epitopes (Michel Klein WP3) 3 epitopes/protein used in vaccine trials (21) Additional epitopes from proteins with CD8 epitopes (43)
 Proteins with CD8 epitopes(25) Proteins from vaccine trials (Michel Klein WP3) Selected in proteins - previously described by other groups to have CTL epitopes (Michel Klein WP3) 3 epitopes/protein used in vaccine trials (21) Additional epitopes from proteins with CD8 epitopes (43)")
28
Peptides TBVAC peptides: Ag85A/B, ESAT6, PPE, HBHA TB-CD8 peptides: Mycobacteria tuberculosis H37Rv strain

29
Analysing peptide screening CD3 CD8 CD4+CD8 cells CD8+ antigen Specific cells

30
CD8 T cell proliferation to A2 motif bearing peptides

32
CD8 T cell proliferation to A3 motif bearing peptides

33
A3-peptides. Binding versus peptide immunogenicity 3/5 donor recognition

34
CD8 T cell proliferation to B7 motif bearing peptides

35
B7-peptides Binding versus peptide immunogenicity

36
PPD-ve individuals do not respond to peptides PPD responses < 1% cfse+ve No responses to peptides A2 donorsA3 donors B7 donors

37
Peptides Recognised by CD8 T cells A2 peptides A3 peptides B7 peptides 4/11 (36%) 9/13 (70%) 6/14 (43%)
 9/13 (70%) 6/14 (43%)")
38
SUMMARY 19/38 predicted peptides induced a CD8 proliferative response The frequency of proliferating CD8 T cell response to peptides varied between individuals Heterogeneous response to peptides For A3-peptide responses, 3/5 donors recognised the same peptide: QINELHHSK (CD8-#108-76), suggesting it may be immunodominant peptide
, suggesting it may be immunodominant peptide")
39
Acknowledgements. Vaccines4TB Prof. Dr. Tom Ottenhoff Tuberculosis group Immunohematology and Blood Transfusion Leiden University Medical Center Leiden, Netherlands Proliferation assays, FACS analysis and IFN-g-ELISA Leucosep Isolation of PBMC Immunological bioinformatic group CBS-BioCentrum, DTU Techinical University of Denmark In silico peptide prediction, NetCTL Fatima Kazi Pascale van Weeren And the rest of the Ottenhoff’s group Michel Klein Tom Søren Buus, MD, Ph.D Prof. IMMI, University of Copenhagen MHC binding Ugur Sahin Ganymed Genetic library

Similar presentations















>")
 update ACSM workshop, Amman, Jordan April 13-17, 2008 Dr. Sevil Huseynova.>")
Caused by Mycobacterium.>")


