Download presentation
Presentation is loading. Please wait.

1
Introduction to Survival Analysis

2
Early example of survival analysis, 1669
Christiaan Huygens' 1669 curve showing how many out of 100 people survive until 86 years. From: Howard Wainer STATISTICAL GRAPHICS: Mapping the Pathways of Science. Annual Review of Psychology. Vol. 52:

3
Early example of survival analysis
Roughly, what shape is this function? What was a person’s chance of surviving past 20? Past 36? This is survival analysis! We are trying to estimate this curve—only the outcome can be any binary event, not just death.

4
What is survival analysis?
Statistical methods for analyzing longitudinal data on the occurrence of events. Events may include death, injury, onset of illness, recovery from illness (binary variables) or transition above or below the clinical threshold of a meaningful continuous variable (e.g. CD4 counts). Accommodates data from randomized clinical trial or cohort study design.
 or transition above or below the clinical threshold of a meaningful continuous variable (e.g. CD4 counts). Accommodates data from randomized clinical trial or cohort study design.")
5
Randomized Clinical Trial (RCT)
Intervention Control Disease Random assignment Disease-free Target population Disease-free, at-risk cohort Disease Disease-free TIME

6
Randomized Clinical Trial (RCT)
Treatment Control Cured Random assignment Not cured Target population Patient population Cured Not cured TIME

7
Randomized Clinical Trial (RCT)
Treatment Control Dead Random assignment Alive Target population Patient population Dead Alive TIME

8
Cohort study (prospective/retrospective)
Disease Exposed Disease-free Target population Disease-free cohort Disease Unexposed Disease-free TIME

9
Examples of survival analysis in medicine

10
RCT: Women’s Health Initiative (JAMA, 2001)
On hormones On placebo Cumulative incidence

11
WHI and low-fat diet… Control Low-fat diet
Prentice, R. L. et al. JAMA 2006;295: Control Low-fat diet

12
Retrospective cohort study: From December 2003 BMJ: Aspirin, ibuprofen, and mortality after myocardial infarction: retrospective cohort study

13
Why use survival analysis?
1. Why not compare mean time-to-event between your groups using a t-test or linear regression? -- ignores censoring 2. Why not compare proportion of events in your groups using risk/odds ratios or logistic regression? --ignores time 1. If no censoring (everyone followed to outcome-of-interest) than ttest on mean or median time to event is fine. 2. If time at-risk was the same for everyone, could just use proportions.
 than ttest on mean or median time to event is fine. 2. If time at-risk was the same for everyone, could just use proportions.")
14
Survival Analysis: Terms
Time-to-event: The time from entry into a study until a subject has a particular outcome Censoring: Subjects are said to be censored if they are lost to follow up or drop out of the study, or if the study ends before they die or have an outcome of interest. They are counted as alive or disease-free for the time they were enrolled in the study. PhD candidates who are most likely to take longest may be most likely to drop out, thereby biasing results.

15
Review Question 1 Which of the following data sets is likely to lend itself to survival analysis? A case-control study of caffeine intake and breast cancer. A randomized controlled trial where the outcome was whether or not women developed breast cancer in the study period. A cohort study where the outcome was the time it took women to develop breast cancer. A cross-sectional study which identified both whether or not women have ever had breast cancer and their date of diagnosis.

16
Review Question 1 Which of the following data sets is likely to lend itself to survival analysis? A case-control study of caffeine intake and breast cancer. A randomized controlled trial where the outcome was whether or not women developed breast cancer in the study period. A cohort study where the outcome was the time it took women to develop breast cancer. A cross-sectional study which identified both whether or not women have ever had breast cancer and their date of diagnosis.

17
Introduction to Kaplan-Meier
Non-parametric estimate of the survival function: Simply, the empirical probability of surviving past certain times in the sample (taking into account censoring).
.")
18
Introduction to Kaplan-Meier
Non-parametric estimate of the survival function. Commonly used to describe survivorship of study population/s. Commonly used to compare two study populations. Intuitive graphical presentation.

19
Survival Data (right-censored)
Beginning of study End of study Time in months Subject B Subject A Subject C Subject D Subject E 1. subject E dies at 4 months X

20
Corresponding Kaplan-Meier Curve
100% Time in months Probability of surviving to 4 months is 100% = 5/5 Fraction surviving this death = 4/5 Subject E dies at 4 months

21
Survival Data Beginning of study End of study Time in months
Subject B Subject A Subject C Subject D Subject E 2. subject A drops out after 6 months 3. subject C dies at 7 months X 1. subject E dies at 4 months X

22
Corresponding Kaplan-Meier Curve
100% Time in months Fraction surviving this death = 2/3 subject C dies at 7 months

23
Survival Data Beginning of study End of study Time in months
Subject B Subject A Subject C Subject D Subject E 2. subject A drops out after 6 months 4. Subjects B and D survive for the whole year-long study period 3. subject C dies at 7 months X 1. subject E dies at 4 months X

24
Corresponding Kaplan-Meier Curve
100% Time in months Rule from probability theory: P(A&B)=P(A)*P(B) if A and B independent In survival analysis: intervals are defined by failures (2 intervals leading to failures here). P(surviving intervals 1 and 2)=P(surviving interval 1)*P(surviving interval 2) Product limit estimate of survival = P(surviving interval 1/at-risk up to failure 1) * P(surviving interval 2/at-risk up to failure 2) = 4/5 * 2/3= .5333
=P(A)*P(B) if A and B independent. In survival analysis: intervals are defined by failures (2 intervals leading to failures here). P(surviving intervals 1 and 2)=P(surviving interval 1)*P(surviving interval 2) Product limit estimate of survival = P(surviving interval 1/at-risk up to failure 1) * P(surviving interval 2/at-risk up to failure 2) = 4/5 * 2/3=")
25
The product limit estimate
The probability of surviving in the entire year, taking into account censoring = (4/5) (2/3) = 53% NOTE: 40% (2/5) because the one drop-out survived at least a portion of the year. AND <60% (3/5) because we don’t know if the one drop-out would have survived until the end of the year.
 (2/3) = 53% NOTE: 40% (2/5) because the one drop-out survived at least a portion of the year. AND <60% (3/5) because we don’t know if the one drop-out would have survived until the end of the year.")
26
Example 1: time-to-conception for subfertile women
“Failure” here is a good thing. 38 women (in 1982) were treated for infertility with laparoscopy and hydrotubation. All women were followed for up to 2-years to describe time-to-conception. The event is conception, and women "survived" until they conceived. Example from: BMJ, Dec 1998; 317:
 were treated for infertility with laparoscopy and hydrotubation. All women were followed for up to 2-years to describe time-to-conception. The event is conception, and women survived until they conceived. Example from: BMJ, Dec 1998; 317:")
27
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2 3 4 7 8 9 11 24 6 10 13 16 Conceived (event) Did not conceive (censored) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 Did not conceive (censored) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
28
Corresponding Kaplan-Meier Curve
S(t) is estimated at 9 event times. (step-wise function)
 is estimated at 9 event times. (step-wise function)")
29
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2 3 4 7 8 9 11 24 6 10 13 16 Conceived (event) Did not conceive (censored) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 Did not conceive (censored) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
30
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2 3 4 7 8 9 11 24 6 10 13 16 Conceived (event) Did not conceive (censored) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 Did not conceive (censored) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
31
Corresponding Kaplan-Meier Curve
6 women conceived in 1st month (1st menstrual cycle). Therefore, 32/38 “survived” pregnancy-free past 1 month.
. Therefore, 32/38 survived pregnancy-free past 1 month.")
32
Corresponding Kaplan-Meier Curve
S(t=1) = 32/38 = 84.2% S(t) represents estimated survival probability: P(T>t) Here P(T>1).
 = 32/38 = 84.2% S(t) represents estimated survival probability: P(T>t) Here P(T>1).")
33
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2.1 3 4 7 8 2 9 11 24 6 10 13 16 Conceived (event) Did not conceive (censored) Important detail of how the data were coded: Censoring at t=2 indicates survival PAST the 2nd cycle (i.e., we know the woman “survived” her 2nd cycle pregnancy-free). Thus, for calculating KM estimator at 2 months, this person should still be included in the risk set. Think of it as 2+ months, e.g., 2.1 months. Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 Did not conceive (censored) Important detail of how the data were coded: Censoring at t=2 indicates survival PAST the 2nd cycle (i.e., we know the woman survived her 2nd cycle pregnancy-free). Thus, for calculating KM estimator at 2 months, this person should still be included in the risk set. Think of it as 2+ months, e.g., 2.1 months. Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
34
Corresponding Kaplan-Meier Curve

35
Corresponding Kaplan-Meier Curve
5 women conceive in 2nd month. The risk set at event time 2 included 32 women. Therefore, 27/32=84.4% “survived” event time 2 pregnancy-free. S(t=2) = ( 84.2%)*(84.4%)=71.1%
 = ( 84.2%)*(84.4%)=71.1%")
36
Risk set at 3 months includes 26 women
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2.1 3.1 4 7 8 2 9 11 3 24 6 10 13 16 Conceived (event) Did not conceive (censored) Risk set at 3 months includes 26 women Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) Conceived (event) Did not conceive (censored) Risk set at 3 months includes 26 women. Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
37
Corresponding Kaplan-Meier Curve

38
Corresponding Kaplan-Meier Curve
3 women conceive in the 3rd month. The risk set at event time 3 included 26 women. 23/26=88.5% “survived” event time 3 pregnancy-free. S(t=3) = ( 84.2%)*(84.4%)*(88.5%)=62.8%
 = ( 84.2%)*(84.4%)*(88.5%)=62.8%")
39
Risk set at 4 months includes 22 women
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2 3.1 4 7 8 9 11 3 24 6 10 13 16 Conceived (event) Did not conceive (censored) Risk set at 4 months includes 22 women Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) Conceived (event) Did not conceive (censored) Risk set at 4 months includes 22 women. Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
40
Corresponding Kaplan-Meier Curve

41
Corresponding Kaplan-Meier Curve
3 women conceive in the 4th month, and 1 was censored between months 3 and 4. The risk set at event time 4 included 22 women. 19/22=86.4% “survived” event time 4 pregnancy-free. S(t=4) = ( 84.2%)*(84.4%)*(88.5%)*(86.4%)=54.2%
 = ( 84.2%)*(84.4%)*(88.5%)*(86.4%)=54.2%")
42
Risk set at 6 months includes 18 women
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2 3 4.1 7 8 9 11 24 4 6 10 13 16 Conceived (event) Did not conceive (censored) Risk set at 6 months includes 18 women Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) Conceived (event) Did not conceive (censored) Risk set at 6 months includes 18 women. Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
43
Corresponding Kaplan-Meier Curve

44
Corresponding Kaplan-Meier Curve
2 women conceive in the 6th month of the study, and one was censored between months 4 and 6. The risk set at event time 5 included 18 women. 16/18=88.8% “survived” event time 5 pregnancy-free. S(t=6) = (54.2%)*(88.8%)=42.9%
 = (54.2%)*(88.8%)=42.9%")
45
Skipping ahead to the 9th and final event time (months=16)…
S(t=13) 22% (“eyeball” approximation)
 22% ( eyeball approximation)")
46
Raw data: Time (months) to conception or censoring in 38 sub-fertile women after laparoscopy and hydrotubation (1982 study) 1 2 3 4 7 8 9 11 24 6 10 13 16 Conceived (event) Did not conceive (censored) 2 remaining at 16 months (9th event time) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:
 Did not conceive (censored) 2 remaining at 16 months (9th event time) Data from: Luthra P, Bland JM, Stanton SL. Incidence of pregnancy after laparoscopy and hydrotubation. BMJ 1982; 284:")
47
Skipping ahead to the 9th and final event time (months=16)…
S(t=16) =( 22%)*(2/3)=15% Tail here just represents that the final 2 women did not conceive (cannot make many inferences from the end of a KM curve)!
 =( 22%)*(2/3)=15% Tail here just represents that the final 2 women did not conceive (cannot make many inferences from the end of a KM curve)!")
48
Comparing 2 groups Use log-rank test to test the null hypothesis of no difference between survival functions of the two groups

49
Kaplan-Meier: example 2
Researchers randomized 44 patients with chronic active hepatitis were to receive prednisolone or no treatment (control), then compared survival curves. Example from: BMJ 1998;317: ( 15 August )
, then compared survival curves. Example from: BMJ 1998;317: ( 15 August )")
50
Data from: BMJ 1998;317:468-469 ( 15 August ) *=censored
Survival times (months) of 44 patients with chronic active hepatitis randomised to receive prednisolone or no treatment. Prednisolone (n=22) Control (n=22) 2 6 3 12 4 54 7 56 * 10 68 22 89 28 96 29 32 125* 37 128* 40 131* 41 140* 141* 61 143 63 145* 71 146 127* 148* 162* 146* 168 158* 173* 167* 181* 182* Data from: BMJ 1998;317: ( 15 August ) *=censored
 of 44 patients with chronic active hepatitis randomised to receive prednisolone or no treatment. Prednisolone (n=22) Control (n=22) * * * * * 141* * * 148* 162* 146* * 173* 167* 181* 182* Data from: BMJ 1998;317: ( 15 August ) *=censored.")
51
Kaplan-Meier: example 2
Are these two curves different? Big drops at the end of the curve indicate few patients left. E.g., only 2/3 (66%) survived this drop. Misleading to the eye—apparent convergence by end of study. But this is due to 6 controls who survived fairly long, and 3 events in the treatment group when the sample size was small.
 survived this drop. Misleading to the eye—apparent convergence by end of study. But this is due to 6 controls who survived fairly long, and 3 events in the treatment group when the sample size was small.")
52
Log-rank test Test of Equality over Strata Pr > Test Chi-Square DF Chi-Square Log-Rank Chi-square test (with 1 df) of the (overall) difference between the two groups. Groups appear significantly different.
 of the (overall) difference between the two groups. Groups appear significantly different.")
53
Caveats Survival estimates can be unreliable toward the end of a study when there are small numbers of subjects at risk of having an event.

54
WHI and breast cancer Small numbers left

55
Limitations of Kaplan-Meier
Mainly descriptive Doesn’t control for covariates Requires categorical predictors Can’t accommodate predictor variables that change over time

56
Review question 2 A two-sample t-test. ANOVA Repeated-measures ANOVA
Investigators studied a cohort of individuals who joined a weight-loss program by tracking their weight loss over 1 year. Which of the following statistical test is likely the most appropriate test for evaluating the effectiveness of the weight loss program? A two-sample t-test. ANOVA Repeated-measures ANOVA Chi-square Kaplan-Meier methods

57
Review question 2 A two-sample t-test. ANOVA Repeated-measures ANOVA
Investigators studied a cohort of individuals who joined a weight-loss program by tracking their weight loss over 1 year. Which of the following statistical test is likely the most appropriate test for evaluating the effectiveness of the weight loss program? A two-sample t-test. ANOVA Repeated-measures ANOVA Chi-square Kaplan-Meier methods

58
Review question 3 A two-sample t-test. ANOVA. Repeated-measures ANOVA
Investigators compared mean cholesterol level between cases with heart disease and controls without heart disease. Which of the following is likely the most appropriate statistical test for this comparison? A two-sample t-test. ANOVA. Repeated-measures ANOVA Chi-square Kaplan-Meier methods

59
Review question 3 A two-sample t-test. ANOVA. Repeated-measures ANOVA
Investigators compared mean cholesterol level between cases with heart disease and controls without heart disease. Which of the following is likely the most appropriate statistical test for this comparison? A two-sample t-test. ANOVA. Repeated-measures ANOVA Chi-square Kaplan-Meier methods

60
Review question 4 Logistic regression Cox regression Linear regression
What is another way to analyze the data from review question 3? Logistic regression Cox regression Linear regression Kaplan-Meier methods There is no other way.

61
Review question 4 Logistic regression Cox regression Linear regression
What is another way to analyze the data from review question 3? Logistic regression Cox regression Linear regression Kaplan-Meier methods There is no other way.

62
Review question 5 Which statement about this K-M curve is correct?
The mortality rate was higher in the control group than the treated group. The probability of surviving past 100 days was about 50% in the treated group. The probability of surviving past 100 days was about 70% in the control group. Treatment should be recommended.

63
Review question 5 Which statement about this K-M curve is correct?
The mortality rate was higher in the control group than the treated group. The probability of surviving past 100 days was about 50% in the treated group. The probability of surviving past 100 days was about 70% in the control group. Treatment should be recommended.

64
Introduction to Cox Regression
Also called proportional hazards regression Multivariate regression technique where time-to-event (taking into account censoring) is the dependent variable. Estimates adjusted hazard ratios. A hazard ratio is a ratio of rates (hazard rates)
 is the dependent variable. Estimates adjusted hazard ratios. A hazard ratio is a ratio of rates (hazard rates)")
65
History “Regression Models and Life-Tables” by D.R. Cox, published in 1972, is one of the most frequently cited journal articles in statistics and medicine Introduced “maximum partial likelihood”

66
Introduction to Cox Regression
Distinction between hazard/rate ratio and odds ratio/risk ratio: Hazard ratio: ratio of rates Odds/risk ratio: ratio of proportions All are measures of relative risk! By taking into account time, you are taking into account more information than just binary yes/no. Gain power/precision. Logistic regression aims to estimate the odds ratio; Cox regression aims to estimate the hazard ratio

67
Example 1: Study of publication bias
By Kaplan-Meier methods From: Publication bias: evidence of delayed publication in a cohort study of clinical research projects BMJ 1997;315: (13 September)
")
68
Univariate Cox regression
Table 4 Risk factors for time to publication using univariate Cox regression analysis Characteristic # not published # published Hazard ratio (95% CI) Null 29 23 1.00 Non-significant trend 16 4 0.39 (0.13 to 1.12) Significant 47 99 2.32 (1.47 to 3.66) Interpretation: Significant results have a 2-fold higher incidence of publication compared to null results. From: Publication bias: evidence of delayed publication in a cohort study of clinical research projects BMJ 1997;315: (13 September)
 Null Non-significant trend (0.13 to 1.12) Significant (1.47 to 3.66) Interpretation: Significant results have a 2-fold higher incidence of publication compared to null results. From: Publication bias: evidence of delayed publication in a cohort study of clinical research projects BMJ 1997;315: (13 September)")
69
Example 2: Study of mortality in academy award winners for screenwriting
Kaplan-Meier methods From: Longevity of screenwriters who win an academy award: longitudinal study BMJ 2001;323: ( 22-29 December )
")
70
Relative increase in death rate for winners
Table 2. Death rates for screenwriters who have won an academy award.* Values are percentages (95% confidence intervals) and are adjusted for the factor indicated Relative increase in death rate for winners Basic analysis 37 (10 to 70) Adjusted analysis Demographic: Year of birth 32 (6 to 64) Sex 36 (10 to 69) Documented education 39 (12 to 73) All three factors 33 (7 to 65) Professional: Film genre Total films Total four star films 40 (13 to 75) Total nominations 43 (14 to 79) Age at first film 36 (9 to 68) Age at first nomination All six factors 40 (11 to 76) All nine factors 35 (7 to 70) HR=1.37; interpretation: 37% higher incidence of death for winners compared with nominees HR=1.35; interpretation: 35% higher incidence of death for winners compared with nominees even after adjusting for potential confounders
 and are adjusted for the factor indicated. Relative increase in death rate for winners. Basic analysis. 37 (10 to 70) Adjusted analysis. Demographic: Year of birth. 32 (6 to 64) Sex. 36 (10 to 69) Documented education. 39 (12 to 73) All three factors. 33 (7 to 65) Professional: Film genre. Total films. Total four star films. 40 (13 to 75) Total nominations. 43 (14 to 79) Age at first film. 36 (9 to 68) Age at first nomination. All six factors. 40 (11 to 76) All nine factors. 35 (7 to 70) HR=1.37; interpretation: 37% higher incidence of death for winners compared with nominees. HR=1.35; interpretation: 35% higher incidence of death for winners compared with nominees even after adjusting for potential confounders.")
71
Characteristics of Cox Regression
Can accommodate both discrete and continuous measures of event times Easy to incorporate time-dependent covariates—covariates that may change in value over the course of the observation period

72
Characteristics of Cox Regression, continued
Cox models the effect of covariates on the hazard rate but leaves the baseline hazard rate unspecified. Does NOT assume knowledge of absolute risk. Estimates relative rather than absolute risk.

73
Assumptions of Cox Regression
Proportional hazards assumption: the hazard for any individual is a fixed proportion of the hazard for any other individual Multiplicative risk

74
The Hazard function In words: the probability that if you survive to t, you will succumb to the event in the next instant.

75
The model Can take on any form! Components:
A baseline hazard function that is left unspecified but must be positive (=the hazard when all covariates are 0) A linear function of a set of k fixed covariates that is exponentiated. (=the relative risk) Can take on any form!
 A linear function of a set of k fixed covariates that is exponentiated. (=the relative risk) Can take on any form!")
76
The model Proportional hazards:
Hazard for person i (eg a smoker) Hazard ratio Hazard for person j (eg a non-smoker) Hazard functions should be strictly parallel! Produces covariate-adjusted hazard ratios!
 Hazard ratio. Hazard for person j (eg a non-smoker) Hazard functions should be strictly parallel! Produces covariate-adjusted hazard ratios!")
77
The model: binary predictor
This is the hazard ratio for smoking adjusted for age.

78
The model:continuous predictor
This is the hazard ratio for a 10-year increase in age, adjusted for smoking. Exponentiating a continuous predictor gives you the hazard ratio for a 1-unit increase in the predictor.

79
Review Question 6 Exponentiating a beta-coefficient from linear regression gives you what? Odds ratios Risk ratios Hazard ratios None of the above

80
Review Question 6 Exponentiating a beta-coefficient from linear regression gives you what? Odds ratios Risk ratios Hazard ratios None of the above

81
Review Question 7 Exponentiating a beta-coefficient from logistic regression gives you what? Odds ratios Risk ratios Hazard ratios None of the above

82
Review Question 7 Exponentiating a beta-coefficient from logistic regression gives you what? Odds ratios Risk ratios Hazard ratios None of the above

83
Review Question 8 Exponentiating a beta-coefficient from Cox regression gives you what? Odds ratios Risk ratios Hazard ratios None of the above

84
Review Question 8 Exponentiating a beta-coefficient from Cox regression gives you what? Odds ratios Risk ratios Hazard ratios None of the above

85
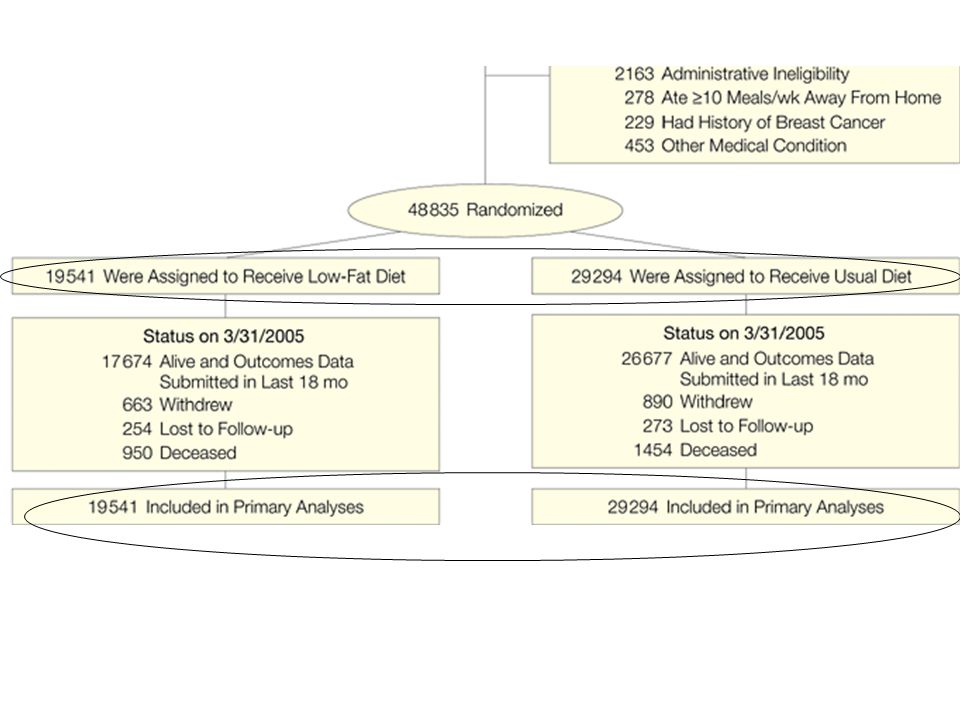
Intention-to-Treat Analysis in Randomized Trials
Intention-to-treat analysis: compare outcomes according to the groups to which subjects were initially randomized, regardless of which intervention (if any) they actually followed.
 they actually followed.")
86
Intention to treat Participants will be counted in the intervention group to which they were originally assigned, even if they: Refused the intervention after randomization Discontinued the intervention during the study Followed the intervention incorrectly Violated study protocol Missed follow-up measurements

87
Dietary Modification Trial
<20% of diet from fat >=5 servings of fruit and vegetables >=6 servings of whole grains Primary outcomes: breast and colorectal cancer

88
Participant Flow in the Dietary Modification Component of the Women's Health Initiative
Prentice, R. L. et al. JAMA 2006;295: Copyright restrictions may apply.

90
Why intention to treat? Preserves the benefits of randomization.
Randomization balances potential confounding factors in the study arms. This balance will be lost if the data are analyzed according to how participants self-selected rather than how they were randomized. Simulates real life, where patients often don’t adhere perfectly to treatment or may discontinue treatment altogether Evaluates effectiveness, rather than efficacy

91
Baseline Demographics of Participants in Women's Health Initiative Dietary Modification Trial*
Copyright restrictions may apply. Prentice, R. L. et al. JAMA 2006;295:

92
Benefits of randomization…

93
Nutrient Consumption Estimates and Body Weight at Baseline and Year 1
Prentice, R. L. et al. JAMA 2006;295: Copyright restrictions may apply.

94
Real-world effectiveness…
Only 31 percent of treatment participants got their dietary fat below 20% in the first year.

95
Effect of intention to treat on the statistical analysis
Intention-to-treat analyses tend to underestimate treatment effects; increased variability due to switching “waters down” results.

96
Example Take the following hypothetical RCT:
Treated subjects have a 25% chance of dying during the 2-year study vs. placebo subjects have a 50% chance of dying. TRUE RR= 25%/50% = .50 (treated have 50% less chance of dying) You do a 2-yr RCT of 100 treated and 100 placebo subjects. If nobody switched, you would see about 25 deaths in the treated group and about 50 deaths in the placebo group (give or take a few due to random chance). Observed RR .50
 You do a 2-yr RCT of 100 treated and 100 placebo subjects. If nobody switched, you would see about 25 deaths in the treated group and about 50 deaths in the placebo group (give or take a few due to random chance). Observed RR .50.")
97
Example, continued BUT, if early in the study, 25 treated subjects switch to placebo and 25 placebo subjects switch to control. You would see about 25* *.50 = deaths in the placebo group And about 25* *.25 = 31 deaths in the treated group Observed RR = 31/44 .70 Diluted effect! (but not biased)
")
98
The researchers factored this into their power calculation…
The study was powered to find a 14% difference in breast cancer risk between treatment and control. They assumed a 50% reduction in risk with perfect adherence, but calculated that this would translate to only a 14% reduction in risk with imperfect adherence.

99
Alternatives to ITT Per-protocol analysis Treatment-received analysis
Restricts analysis to only those who followed the assigned intervention until the end. Treatment-received analysis Censored analysis: Subjects are dropped from the analysis at the time of stopping the assigned treatment Transition analysis: e.g., controls who cross over to treatment contribute to the denominator for the control group until they cross over; then they contribute to the denominator for the treatment group. But becomes an observational study…

100
Review question 9 I randomized 600 people to receive treatment (n=300) or placebo (n=300). Of these, 10 treatment and 8 placebo subjects never started their study drug. An additional 30 dropped out of each group before the end of the trial (or were lost to followup). 18 treated subjects and 3 placebo subjects discontinued their treatment because of side effects. How many subjects do I include in my primary statistical analysis? 290 treatment, 292 placebo 272 treatment, 289 placebo 272 treatment, 292 placebo 242 treatment, 259 placebo 300 treatment, 300 placebo
. 18 treated subjects and 3 placebo subjects discontinued their treatment because of side effects. How many subjects do I include in my primary statistical analysis 290 treatment, 292 placebo. 272 treatment, 289 placebo. 272 treatment, 292 placebo. 242 treatment, 259 placebo. 300 treatment, 300 placebo.")
101
Review question 9 I randomized 600 people to receive treatment (n=300) or placebo (n=300). Of these, 10 treatment and 8 placebo subjects never started their study drug. An additional 30 dropped out of each group before the end of the trial (or were lost to followup). 18 treated subjects and 3 placebo subjects discontinued their treatment because of side effects. How many subjects do I include in my primary statistical analysis? 290 treatment, 292 placebo 272 treatment, 289 placebo 272 treatment, 292 placebo 242 treatment, 259 placebo 300 treatment, 300 placebo
. 18 treated subjects and 3 placebo subjects discontinued their treatment because of side effects. How many subjects do I include in my primary statistical analysis 290 treatment, 292 placebo. 272 treatment, 289 placebo. 272 treatment, 292 placebo. 242 treatment, 259 placebo. 300 treatment, 300 placebo.")
102
Homework Finish reading textbook Study for the final exam!

Similar presentations
![If we use a logistic model, we do not have the problem of suggesting risks greater than 1 or less than 0 for some values of X: E[1{outcome = 1} ] = exp(a+bX)/](/11/3248837/big_thumb.jpg "If we use a logistic model, we do not have the problem of suggesting risks greater than 1 or less than 0 for some values of X: E[1{outcome = 1} ] = exp(a+bX)/>")

>")





>")
 Cox-Regression>")









. MEASURES OF DISEASE FREQUENCY Absolute measures of disease frequency: –Incidence –Prevalence –Odds Measures of association:>")