Download presentation
Presentation is loading. Please wait.

1
Pituitary Insufficiency William Harper, MD, FRCPC Endocrinology & Metabolism Assistant Professor of Medicine McMaster University

2
Pituitary Disorders Mass effect Headaches CN II, III, IV, V 1, V 2, VI Pituitary hypersecretory Syndrome PRL, GH, ACTH, > > TSH Anterior Pituitary Dysfunction ACTH, TSH, LH/FSH > > GH Posterior Pituitary Dysfunction ADH

3
Mass Effect: H/A, CN II, EOM, V 1, V 2 (LR 6 SO 4 ) 3 V1V1 V2V2
 3 V1V1 V2V2")
7
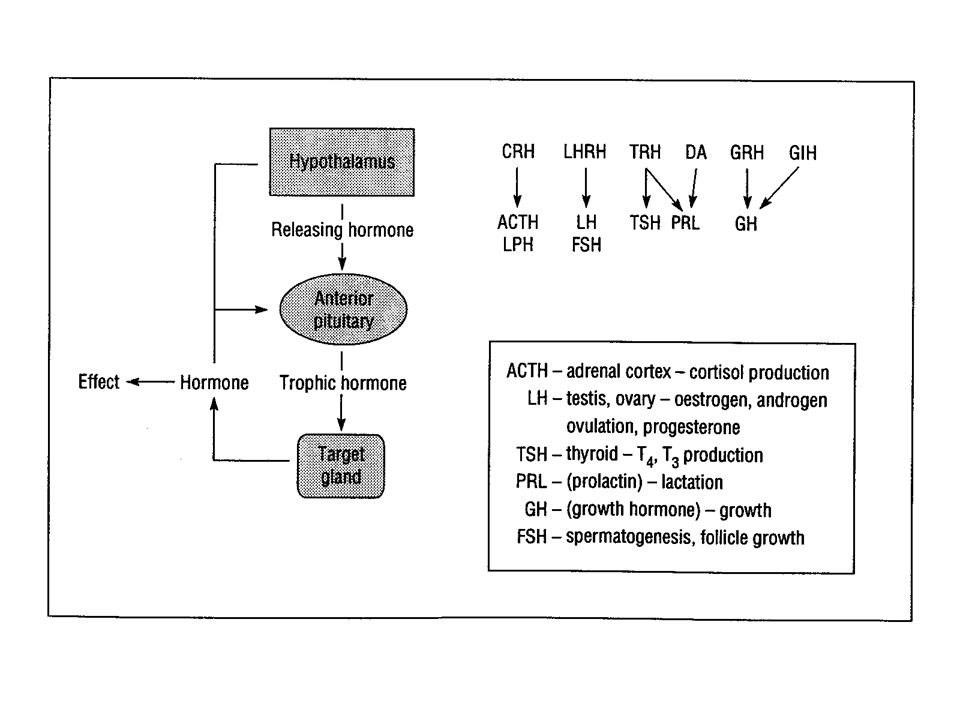
H-P-A Axis

8
Cushing’s Disease Ectopic ACTH High ACTH Cushing’s

9
Establish hypercortisolism (Cushing’s syndrome) “Screening” tests 1 mg O/N DMST DXM 1 mg po 11PM 8AM plasma cortisol < 140 nM R/O Cushing’s Syndrome »SEN 98% SPEC 71-80% »< 50 nM SEN ~100% SPEC ? (Poor), still some cases missed! 24 UFC < 248 nM/d R/O Cushing’s Syndrome (SEN 95-100%) 248-840 nM/d Equivocal > 840 nM/d consistent with Cushing’s Syndrome (SPEC 98%)
, still some cases missed. 24 UFC < 248 nM/d R/O Cushing’s Syndrome (SEN %) nM/d Equivocal > 840 nM/d consistent with Cushing’s Syndrome (SPEC 98%).")
10
Establish hypercortisolism (Cushing’s syndrome) “Confirmatory Tests” 24 UFC > 840 nM/d Establishes Cushing’s Syndrome on 2 or more collections AND clear clinical findings of Cushing’s makes diagnosis of Cushing’s with SPEC 98% Otherwise, need an additional confirmatory test. LDDST (Liddle Test) 2 baseline 24h urine for cortisol and 17-OH steroids DXM 0.5 mg q6h x 48h (8 doses) During 2 nd day on DXM repeat 24h urine collection –UFC > 100 nM/d or 17OHS > 11 uM/d indicates Cushing’s –Historical gold standard but SEN 56-69%, SPEC 74-100% Plasma cortisol < 50 nM measured 2 or 6 hours after last dose has SEN 90-100% and SPEC 97-100%
 2 baseline 24h urine for cortisol and 17-OH steroids DXM 0.5 mg q6h x 48h (8 doses) During 2 nd day on DXM repeat 24h urine collection –UFC > 100 nM/d or 17OHS > 11 uM/d indicates Cushing’s –Historical gold standard but SEN 56-69%, SPEC % Plasma cortisol < 50 nM measured 2 or 6 hours after last dose has SEN % and SPEC %.")
11
Clinical Suspicion Screen Test: 24 UFC or 1mg O/N DST (+/- evening plasma/salivary cortisol) Confirmatory Testing: Repeat 24 UFC +/- CRH/DXM Test (+/- evening plasma/salivary cortisol) ACTH Independent CT abdo Adrenal Surgery ACTH dependent 1 st 8mg O/N DST or HDDST 2 nd CRH Test if above test negative CRH Test Pituitary MRI Pituitary Surgery IPSS Ectopic ACTH CT thorax, abdo Thyroid U/S Octreotide Scan Continue search for ectopic source Remove ectopic source < 1.1pM>2.2pM 1.1-2.2pM No Stim Positive Stim Conclusive (>0.8-1.0cm) Inconclusive >2 basal >3 CRH <1.5 basal <2 CRH Conclusive No CRH stim No DXM suppression Stim by CRH or DXM suppresses
 Confirmatory Testing: Repeat 24 UFC +/- CRH/DXM Test (+/- evening plasma/salivary cortisol) ACTH Independent CT abdo Adrenal Surgery ACTH dependent 1 st 8mg O/N DST or HDDST 2 nd CRH Test if above test negative CRH Test Pituitary MRI Pituitary Surgery IPSS Ectopic ACTH CT thorax, abdo Thyroid U/S Octreotide Scan Continue search for ectopic source Remove ectopic source < 1.1pM>2.2pM pM No Stim Positive Stim Conclusive (> cm) Inconclusive >2 basal >3 CRH <1.5 basal <2 CRH Conclusive No CRH stim No DXM suppression Stim by CRH or DXM suppresses")
12
Case 49 year old female Adie’s pupil x 2 years L frontoparietal H/A Neurologist ordered MRI Enlarged Pituitary! Subsequent Endo referral TSH 31.7 mU/L, FT4 6 pM Hypothyroid! FSH 63 (menopausal)
.")
14
Pituitary Hyperplasia Another cause of sellar mass! Physiological enlargement of pituitary Lactotroph Hyperplasia (pregnancy) »Pregnancy, most common Thyrotroph, Gonadotroph Hyperplasia »Primary gland failure Somatotroph, Corticotroph Hyperplasia »GHRH or CRH secreting neuroendocrine tumors
 »Pregnancy, most common Thyrotroph, Gonadotroph Hyperplasia »Primary gland failure Somatotroph, Corticotroph Hyperplasia »GHRH or CRH secreting neuroendocrine tumors.")
16
Prolactinoma Most common pituitary tumor Dx: elevated PRL with size/level correlation (stalk-effect!) Treatment: Dopamine Agonist »Bromocriptine, Cabergoline, Pergolide, Quinagolide TSSx XRT Treatment goals: Macroadenoma: shrink tumor (mass effect, H/A) Stop galactorrhea Reestablish menses/fertility »OCP if fertility not wanted
 Treatment: Dopamine Agonist »Bromocriptine, Cabergoline, Pergolide, Quinagolide TSSx XRT Treatment goals: Macroadenoma: shrink tumor (mass effect, H/A) Stop galactorrhea Reestablish menses/fertility »OCP if fertility not wanted")
17
Prolactinoma: pregnancy Microadenoma: 1.6% symptomatic growth Stop bromocriptine once conception achieved Macroadenoma 13-36% symptomatic growth during pregnancy Continue bromocriptine througout pregnancy Monitoring PRL useless Formal VF tests q3mos MRI if any change in vision

19
Anterior Pituitary Dysfunction Gold standard diagnosis = 3x bolus test Insulin ACTH, GH (Insulin Tolerance Test) LHRH LH, FSH TRH TSH, PRL Done > 6 weeks post pituitary surgery ITT contraindicated: elderly, cardiac disease 8AM plasma cortisol 1 mcg ACTH stimulation testing
 LHRH LH, FSH TRH TSH, PRL Done > 6 weeks post pituitary surgery ITT contraindicated: elderly, cardiac disease 8AM plasma cortisol 1 mcg ACTH stimulation testing")
20
Diagnosis of AI 8AM Plasma Cortisol (Pcortisol at 8AM or during “Stress”): < 83 nM AI confirmed < 138 nM suggests AI present (SEN 36%, SPEC~100%) > 552 nM excludes AI (>552 nM @ anytime of day, SEN~100%) [with possible exception of critically-ill patients]
![Diagnosis of AI 8AM Plasma Cortisol (Pcortisol at 8AM or during Stress ): < 83 nM AI confirmed < 138 nM suggests AI present (SEN 36%, SPEC~100%) > 552 nM excludes AI (>552 anytime of day, SEN~100%) [with possible exception of critically-ill patients]](http://images.slideplayer.com/16/4979830/slides/slide_20.jpg "Diagnosis of AI 8AM Plasma Cortisol (Pcortisol at 8AM or during Stress ): < 83 nM AI confirmed < 138 nM suggests AI present (SEN 36%, SPEC~100%) > 552 nM excludes AI (>552 anytime of day, SEN~100%) [with possible exception of critically-ill patients]")
21
Diagnosis of AI Short Cortrosyn/ACTH test Must be performed within a few days of starting exogenous glucocorticoid Rx or else H-P-A axis will be suppressed by steroid Rx Exogenous glucocorticoid must be dexamethasone (isn’t picked up by the cortisol RIA)
")
22
Short Cortrosyn Test High (Standard) Dose: 250 ug IV or IM, measure cortisol t = 0, 30, 60 min Normal: any cortisol > 550 nM (even pre-injection t = 0) Rules out 1˚ AI (SEN 100%) but only 90% SEN for 2˚ AI Low Dose: 1 ug IV (can’t be IM), measure cortisol t = 0, 30 min t = 30 min cortisol > 500 nM rules out 1˚ or 2˚ AI (exception is 2˚ AI of recent onset < 2wk) SEN 95% SPEC 96% ( > 600 nM SEN 100%, SPEC 83%) 1 ug dose stimulates maximal adrenal cortex secretion 30 min after injection and in normal subjects results in a peak plasma ACTH concentration 2X that seen in an ITT
 Dose: 250 ug IV or IM, measure cortisol t = 0, 30, 60 min Normal: any cortisol > 550 nM (even pre-injection t = 0) Rules out 1˚ AI (SEN 100%) but only 90% SEN for 2˚ AI Low Dose: 1 ug IV (can’t be IM), measure cortisol t = 0, 30 min t = 30 min cortisol > 500 nM rules out 1˚ or 2˚ AI (exception is 2˚ AI of recent onset < 2wk) SEN 95% SPEC 96% ( > 600 nM SEN 100%, SPEC 83%) 1 ug dose stimulates maximal adrenal cortex secretion 30 min after injection and in normal subjects results in a peak plasma ACTH concentration 2X that seen in an ITT")
23
Short Cortrosyn Test (cont’d) Criteria requiring a minimum cortisol increment (i.e. 2x baseline or absolute rise of 250 nM) now considered invalid High basal cortisol due to stress or normal diurnal variation may represent near maximal stimulation with an inability to increase secretion further in upwards of 20% of normal patients Possible exception of critically-ill patients
 now considered invalid High basal cortisol due to stress or normal diurnal variation may represent near maximal stimulation with an inability to increase secretion further in upwards of 20% of normal patients Possible exception of critically-ill patients.")
24
Distinguish 1˚ from Central AI Plasma ACTH Measure with basal cortisol during short ACTH test Primary AI: ACTH > 11 pM Central AI: ACTH < 2.2 pM Must measure BEFORE exogenous glucocorticoid administration as will be suppressed almost immediately 2 phases of steroid feedback suppression on ACTH: Fast Phase (sec-min): membrane stabilizing effect Delayed phase (hrs-days): mediated by glucocorticoid receptor
: membrane stabilizing effect Delayed phase (hrs-days): mediated by glucocorticoid receptor")
25
Distinguish 1˚ from Central AI Long Cortrosyn Test Rarely needed Done if plasma ACTH equivocal (2.2-11 pM) or result not available (i.e. not sent before the initiation of exogenous glucocorticoids) 250 ug IV infusion over 8h x 3d Plasma cortisols during infusion (0, 4, and 8h) 24h UFC day prior to and on 3 days with infusion 1˚AI: no response Central AI: some response
 250 ug IV infusion over 8h x 3d Plasma cortisols during infusion (0, 4, and 8h) 24h UFC day prior to and on 3 days with infusion 1˚AI: no response Central AI: some response.")
26
Anterior Pituitary Dysfn Rx Corticosteroids Prednisone 5 mg qhs or qam to 5/2.5 mg daily Cortef 20 mg qhs or qam to 20/10 mg daily Medic-alert, 2-3x dose during acute-illness Surgery: 50mg IV preop & q8h postop Levothyroxine Titrate dose to mid-normal FT4 not TSH Sex steroids Male: testosterone 100 mg/wk IM, androgel 5g/d Female: premenopausal OCP, postmenopausal HRT? Growth hormone?

27
Pituitary Apoplexy Acute pituitary hemorrhage Sudden severe H/A, diploplia, visual loss Shock due to adrenal crisis Diagnosis: pituitary MRI or CT Rx: urgent surgical decompression Solucortef 50 mg IV q8h Dopamine agonist if high PRL/known prolactinoma

29
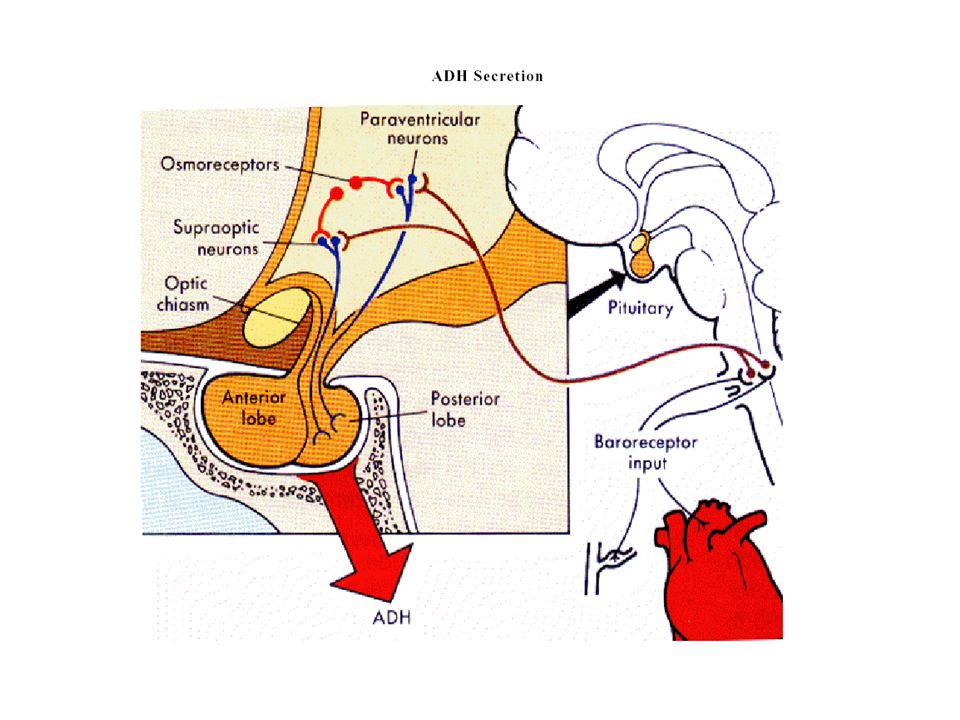
P Na (mEq/L) 130135140145 0 5 ADH (pM) Thirst↓ ECFv Normal Serum [Na] (135-145 mEq/L) Closely Guarded
![P Na (mEq/L) ADH (pM) Thirst↓ ECFv Normal Serum [Na] ( mEq/L) Closely Guarded](http://images.slideplayer.com/16/4979830/slides/slide_29.jpg "P Na (mEq/L) ADH (pM) Thirst↓ ECFv Normal Serum [Na] ( mEq/L) Closely Guarded")
30
Diabetes Insipidus Ddx Diabetes Mellitus Hypercalcemia Solute diuresis: »Volume expansion 2° saline loading »High-protein feeds (urea as osmotic agent) »Post-obstructive diuresis Diabetes Insipidus: »Central (CDI) »Nephrogenic (NDI) Primary (Psychogenic) Polydipsia Polyuria: > 3 L/d +Polydipsia: > 3.5 L/d
 »Post-obstructive diuresis Diabetes Insipidus: »Central (CDI) »Nephrogenic (NDI) Primary (Psychogenic) Polydipsia Polyuria: > 3 L/d +Polydipsia: > 3.5 L/d")
31
Diabetes Insipidus Ddx Central (CDI) Idiopathic –autoimmune Neurosurgery, head trauma Cerebral hypoperfusion Tumor –Craniopharyngioma, pituitary adenoma, suprasellar meningioma, pineal gland, metastasis Infiltration –Fe, Sarcoid, Histiocytosis X Nephrogenic (NDI) X-linked recessive Hypokalemia Hypercalcemia (2° to HPT in particular) Renal disease: after ATN, postobstructive uropathy, RAS, renal transplant, amyloid, Sickle cell anemia Sjogren’s Drugs: –Lithium, 20% of chronic users –Demeclocycline, amphotericin, colchicine
 Idiopathic –autoimmune Neurosurgery, head trauma Cerebral hypoperfusion Tumor –Craniopharyngioma, pituitary adenoma, suprasellar meningioma, pineal gland, metastasis Infiltration –Fe, Sarcoid, Histiocytosis X Nephrogenic (NDI) X-linked recessive Hypokalemia Hypercalcemia (2° to HPT in particular) Renal disease: after ATN, postobstructive uropathy, RAS, renal transplant, amyloid, Sickle cell anemia Sjogren’s Drugs: –Lithium, 20% of chronic users –Demeclocycline, amphotericin, colchicine")
32
Diabetes Insipidus Intact thirst & access to water Hi-normal serum sodium (142-145 mEq/L) Polydipsia (crave cold fluids) Polyuria, Nocturia sleep disturbance 1° treatment is pharmacological Impaired thirst or access to water: Hypernatremia Insufficiently concentrated urine 1° treatment is free water (enteral or IV D5W)
 Polydipsia (crave cold fluids) Polyuria, Nocturia sleep disturbance 1° treatment is pharmacological Impaired thirst or access to water: Hypernatremia Insufficiently concentrated urine 1° treatment is free water (enteral or IV D5W)")
33
Diabetes Insipidus Healthy out-patients DI with Intact thirst or access to water Hi-normal serum sodium (142-145 mEq/L) Polydipsia (crave cold fluids) Polyuria, Nocturia sleep disturbance 1˚ Psychogenic Polydipsia Low-normal serum sodium (135-137 mEq/L) Anxious middle-aged women Psychiatric illness, phenothiazine (dry mouth)
 Polydipsia (crave cold fluids) Polyuria, Nocturia sleep disturbance 1˚ Psychogenic Polydipsia Low-normal serum sodium ( mEq/L) Anxious middle-aged women Psychiatric illness, phenothiazine (dry mouth)")
34
1˚ Polydipsia: “What came first?” The Chicken or the Egg? (Egg) The Polyuria or the Polydipsia?
 The Polyuria or the Polydipsia")
35
Water Deprivation Test Hold water intake for 2-3h prior to coming in. Continue to hold water & Monitor: Urine volume, U OSM q1h Serum Na, OSM q2h If serum OSM/sodium do not rise above normal ranges & UOSM reaches 600 1˚ Polydipsia If serum OSM reaches 295-300 mM & U OSM doesn’t ↑ Diabetes Insipidus established Endogenous ADH should be maximal, check serum ADH –2 green rubber stopper tubes, pre-chilled, on ice, need biochemist Give DDAVP 10 ug IN –CDI: U OSM ↑ by 100-800% (complete CDI), ↑ by 15-50% (partial CDI) with absolute U OSM > 345mM –NDI: U OSM ↑ by up to < 9%, sometimes ↑ as high as 45% but absolute U OSM always < isotonic (290 mM)
, ↑ by 15-50% (partial CDI) with absolute U OSM > 345mM –NDI: U OSM ↑ by up to < 9%, sometimes ↑ as high as 45% but absolute U OSM always < isotonic (290 mM).")
36
Diabetes Insipidus Impaired thirst or access to water Elevated serum sodium/OSM U OSM < 500 mM, U SG < 1.017 If serum sodium/OSM not elevated Not DI! U OSM and U SG are irrelevant

37
Pituitary Surgery/Trauma Triphasic response to surgery Phase 1: DI Axonal injury 2° surgery/swelling Begins after POD #1 (pre-existing DI can occur earlier) Lasts 1-5d Phase 2: SIADH Axonal necrosis of AVP secreting neurons with uncontrolled AVP release Lasts 1-5 days Phase 3: DI Axonal death with cessation of AVP production Usually permanent
 Lasts 1-5d Phase 2: SIADH Axonal necrosis of AVP secreting neurons with uncontrolled AVP release Lasts 1-5 days Phase 3: DI Axonal death with cessation of AVP production Usually permanent")
38
1611 POD # 50 100 150 P Na (mEq/L) 50 100 400 U/O (cc/h) U/O #1 U/O #2
 U/O (cc/h) U/O #1 U/O #2")
39
1611 POD # 50 100 150 P Na (mEq/L) 50 100 400 U/O (cc/h) Na #1 U/O #1
 U/O (cc/h) Na #1 U/O #1")
40
1611 POD # 50 100 150 P Na (mEq/L) 50 100 400 U/O (cc/h) Na #2 U/O #2
 U/O (cc/h) Na #2 U/O #2")
41
1611 POD # 50 100 150 P Na (mEq/L) 50 100 400 U/O (cc/h) Na #1 Na #2 U/O #1 U/O #2 #1 DI #2 Normal
 U/O (cc/h) Na #1 Na #2 U/O #1 U/O #2 #1 DI #2 Normal")
42
PITUITARY SURGERY PROTOCOL Immediately Postop (in recovery room): Send serum for electrolytes, creatinine, blood sugar Send urine for U SG (specific gravity) Then monitor: Accurate I&O: fluid intake & urine output hourly (q1h) with complete tally q12 hours (q12h) Serum electrolytes and U SG : q12h If on steroids (decadron, solucortef, etc.) do capillary blood glucose bid If urine output > 400cc/hour: Serum OSM & urine OSM now and then q12h Serum lytes, creatinine now and then q6h U SG now and then q4h Call Endocrinology Service once serum electrolytes and U SG results are back for possible DDAVP and IV fluid orders Call Endocrinology Service whenever: Serum sodium > 148 Serum sodium < 130 Urine output > 400 cc/h (see above 3.)
: Send serum for electrolytes, creatinine, blood sugar Send urine for U SG (specific gravity) Then monitor: Accurate I&O: fluid intake & urine output hourly (q1h) with complete tally q12 hours (q12h) Serum electrolytes and U SG : q12h If on steroids (decadron, solucortef, etc.) do capillary blood glucose bid If urine output > 400cc/hour: Serum OSM & urine OSM now and then q12h Serum lytes, creatinine now and then q6h U SG now and then q4h Call Endocrinology Service once serum electrolytes and U SG results are back for possible DDAVP and IV fluid orders Call Endocrinology Service whenever: Serum sodium > 148 Serum sodium < 130 Urine output > 400 cc/h (see above 3.)")
43
Treatment of DI Rx Dehydration NS initially if ECFv contraction Then IV D5W or enteral free water to lower serum [Na] »1-2 mEq/h if Na > 160, symptomatic (coma, SZ), acute »Otherwise 0.5-1.0 mEq/h Insensible losses? (0.5 L/d) Do NOT replace U/O if giving DDAVP DDAVP (Desmopressin) Reduces U/O and therefore simplifies fluid therapy Long t½: duration 8-12h, up to 24h Therefore use judiciously »DDAVP 1ug IV/SC x 1 »Only repeat if breaks-thru again (i.e. becomes hypernatremic with dilute polyuria) »Once nasal mucosa stable can switch to intranasal »Also oral form DDAVP now available DDAVP: 1ug IV/SC = 10 ug IN = 0.1 mg PO
![Treatment of DI Rx Dehydration NS initially if ECFv contraction Then IV D5W or enteral free water to lower serum [Na] »1-2 mEq/h if Na > 160, symptomatic (coma, SZ), acute »Otherwise mEq/h Insensible losses.](http://images.slideplayer.com/16/4979830/slides/slide_43.jpg "(0.5 L/d) Do NOT replace U/O if giving DDAVP DDAVP (Desmopressin) Reduces U/O and therefore simplifies fluid therapy Long t½: duration 8-12h, up to 24h Therefore use judiciously »DDAVP 1ug IV/SC x 1 »Only repeat if breaks-thru again (i.e. becomes hypernatremic with dilute polyuria) »Once nasal mucosa stable can switch to intranasal »Also oral form DDAVP now available DDAVP: 1ug IV/SC = 10 ug IN = 0.1 mg PO.")
44
Treatment of DI AVP, Aqueous vasopressin (Pitressin) Only parenteral form, 5-10 U SC q2-4h Lasts 2-6h Can cause HTN, coronary vasospasm Chlorpropamide (OHA which stimulates AVP secretion) 100-500 mg po OD-bid Only useful for partial DI, can cause hypoglycemia HTCZ (induces volume contraction which diminishes free water excretion) 50-100 mg OD-bid Mainstay of Rx for chronic NDI Amiloride (blunts Lithium uptake in distal tubules & collecting ducts) 5-20 mg po OD-bid Drug of choice for Lithium induced DI Indomethacin 100-150 mg po bid-tid (PGs antagonize AVP action) Clofibrate 500 mg po qid (augments AVP release in partial CDI) Tegretol 200-600 mg po od (augments AVP release in partial CDI)
 Only parenteral form, 5-10 U SC q2-4h Lasts 2-6h Can cause HTN, coronary vasospasm Chlorpropamide (OHA which stimulates AVP secretion) mg po OD-bid Only useful for partial DI, can cause hypoglycemia HTCZ (induces volume contraction which diminishes free water excretion) mg OD-bid Mainstay of Rx for chronic NDI Amiloride (blunts Lithium uptake in distal tubules & collecting ducts) 5-20 mg po OD-bid Drug of choice for Lithium induced DI Indomethacin mg po bid-tid (PGs antagonize AVP action) Clofibrate 500 mg po qid (augments AVP release in partial CDI) Tegretol mg po od (augments AVP release in partial CDI)")
Similar presentations











, FRCP Consultant Endocrinologist>")






 is an uncommon condition that occurs when the kidneys are unable to conserve.>")



