Download presentation
Presentation is loading. Please wait.

1
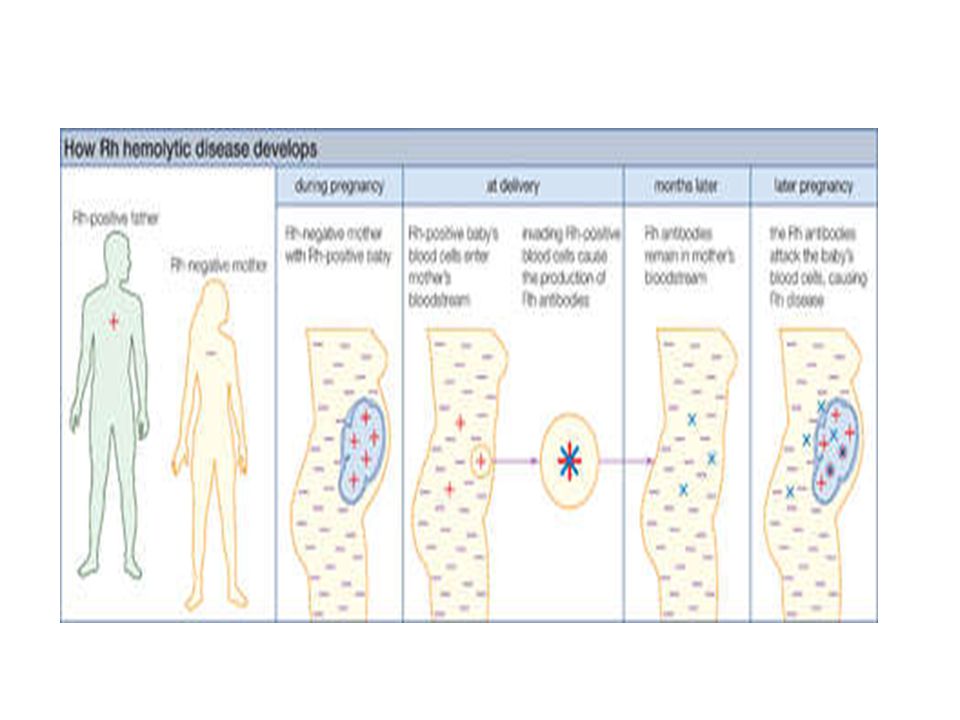
Fetal Haemolytic Disease

2
Maternal antibodies develop against fetal red blood cells IgG antibodies cross the placenta Haemolysis, anaemia, high-output cardiac failure & death

3
Usually a problem with subsequent pregnancies but may occur in the index pregnancy

4
Causes ABO – does not usually cause significant haemolytic disease. Anti-Kell – causes fetal bone marrow aplasia. Rhesus – D antigenanti-D c antigenanti-c E antigenanti-E

5
Incidence Approx 17% of the population is Rh-ve 10% of women at risk of developing anti-D. Incidence 1/1000 pregnancies

6
Predisposing Factors Miscarriage and ectopic pregnancy Invasive procedures ECV Abdominal trauma Antepartum haemorrhage Labour and birth

7
Initial exposure Small IgM response Subsequent exposure Large IgG response

8
IgG crosses placenta Forms antigen-antibody complex on red cell Red cells phagocytosed Anaemia and haemolysis

9
Anaemia Fetal hypoxia Hepatic and cardiac dysfunction Oedema, ascites, pericardial & pleural effusions - HYDROPS

10
Haemolysis Increased bilirubin Jaundice postnatally Kernicterus

11
Prevention Anti-D after any sensitizing episode after 12 weeks Consider routine prophylaxis

12
Management Check antibodies at booking and 3 rd trimester If antibodies present – check antibody levels every 4 weeks to 28 weeks and then 2-weekly to term <4IU/ml – severe disease rare 4-15IU/ml – moderate risk >15IU/ml – 50% risk of severe anaemia

13
Check paternal genotype D antigen autosomal dominant Father DD – fetus Rh positive Father d/D – 50% chance that fetus will be Rh+ve

14
Measurement of blood velocity in middle cerebral artery. Hyperkinetic circulation correlates with fetal anaemia and need for further treatment.

15
Anti-D for sensitising events after 12 weeks. If anti-D antibodies present do not give more anti-D. Serial measurements of Anti-D levels. Observe for signs of fetal anemia – if anemic transfuse or deliver.

Similar presentations
 ISOIMMUNIZATION>")














>")



