Download presentation
Presentation is loading. Please wait.

1
Role of Prostaglandin Analogs in The Treatment of Glaucoma Mahmood J Showail MD

2
Glaucoma One of the most common cause of blindness in the world.

3
Glaucoma Glaucoma is characterized by three factors: Elevated Intra Ocular Pressure (IOP) Optic nerve damage (cupping of the disc) Progressive loss of visual field
 Optic nerve damage (cupping of the disc) Progressive loss of visual field")
4
Visual Field Loss Intraocular Pressure Optic Nerve Damage Glaucoma

5
Glaucoma Mechanisms of aqueous humor Aqueous is produced by the ciliary processes It flows into the posterior chamber Bathes the lens Fills the anterior chamber

6
Glaucoma Aqueous Flow Dynamics Inflow should be equal to the outflow Normal IOP is between 10 – 20 mmHg Normally the IOP is highest in the morning and lowest in the evening Diurnal curve

7
There are two major component of aqueous outflow : Trabecular outflow “pressure dependant” Uveoscleral outflow “pressure independant” Aqueous Humor Outflow

8
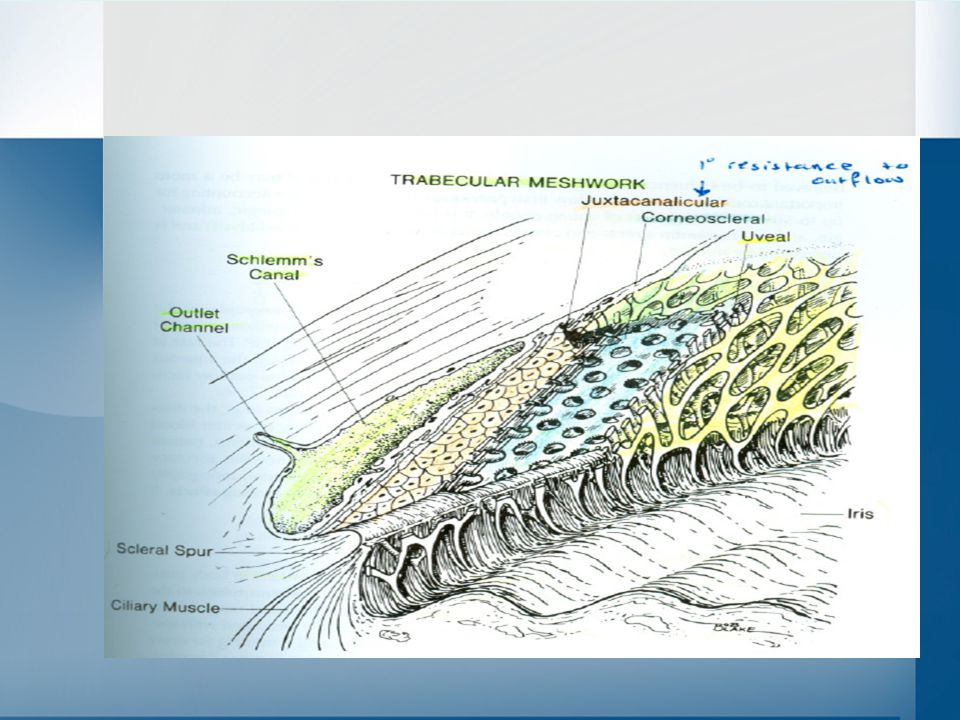
Trabecular Outflow Most of the aqueous exits the eye through trabecular meshwork- schlemm’s canal- venous system The TM can be devided into three zones Uveal Corneoscleral Juxtacanalicular The primary resistance occurs at the juxtacanalicular tissue.

10
Anatomy Review

12
The TM functions as a one way valve that permits aqueous to leave the eye by bulk flow. Once in schlemm’s canal, aqueous enter the episcleral veinous plexus by way of scleral collector channels.

13
Uveoscleral Outflow The aqueous passages from the anterior chamber into the cilliary muscle and then into the supracilliary and suprachoroidal spaces. The fluid then exits the eye through the intact sclera or along the nerves and the vessels that penetrate it.

15
Uveoscleral Outflow Uveoscleral outflow is pressure independent and is believed to be influnced by age. Recent researches suggest that it may be a more important route of aqueous outflow than previously thought. Possibly accounting for up to 50% in normal eyes of young people.

16
Aqueous Humor Outflow The facililty of outflow “C in goldman equation”varies widely in normal eyes The mean value reported from 0.22 to 0.28 µl/min/mmHg Outflow facililty decrease with age & is affected by surgery, trauma, medications and endocrine factors Patients with glaucoma and elevated IOP have decreased outflow facililty

17
Goldman equation Pº = (F/C) + Pv Pº IOP in “mmHg” F rate of aqueous formation “µl/min” C facililty of outflow “µl/min/mmHg” Pv episcleral venous pressure “mmHg”
 + Pv Pº IOP in mmHg F rate of aqueous formation µl/min C facililty of outflow µl/min/mmHg Pv episcleral venous pressure mmHg")
18
How would we decrease the pressure?

19
Glaucoma Decrease the IOP in Glaucoma Decrease the inflow Blocking the mechanism of production Increase the outflow Through the trabecular meshwork Through the uveoscleral channels

20
Prostaglandin Analogs

21
Prostaglandins Analogs Latanaprost (Xalathan) Bimatoprost (Lumigan) Travoprost (Travatan) Side effects: Iris pigmentation and irritation/redness
 Bimatoprost (Lumigan) Travoprost (Travatan) Side effects: Iris pigmentation and irritation/redness")
22
Prostaglandin + Betablockers –Decrease production of aqueous humor (double effectiveness) Generics –Latanoprost + Timolol (0.005% with 0.5% solution) Usage: –Once daily in the morning Glaucoma Drugs Combination Drugs Brands –Xalacom
 Generics –Latanoprost + Timolol (0.005% with 0.5% solution) Usage: –Once daily in the morning Glaucoma Drugs Combination Drugs Brands –Xalacom")
23
Xalacom Careful medical history is important Notify the doctor if the patient suffers from: Asthma Heart disease Diabetes Hypoglycemia Overactive thyroid gland Hypotension Vascular disorders

24
So, How would Prostaglandin analogs works ??

25
Prostaglandin analogues lower intraocular pressure by increasing uveoscleral outflow. Although the precise mechanism is not clearly understood, there appears to be activation of a molecular transduction cascade and increase in the biosynthesis of metalloproteneases ( MMP-1, MMP-2& MMP9). This lead to reduction of extracellular matrix components within the cilliary muscle, iris root and sclera
. This lead to reduction of extracellular matrix components within the cilliary muscle, iris root and sclera.")
26
Uveoscleral out flow is known to flow from the anterior chamber into the extracellular spaces of the ciliary muscle and then in large part pass through sclera. Hence, It is possible that reduction of ECM and widening and decompressing the connective tissue that is present within portions of the uveoscleral pathway may contribute to the mechanism of ↑↑ outflow.

28
Additional mechanisms that may contribute to PG mediated increase of uveoscleral outflow include Relaxation of ciliary muscle and widening of intermuscular spaces. Cell shape changes Cytoskeletal alteration Compaction of the ECM within the tissue of the uveoscleral outflow pathway.

29
Many study have reported that PGF2α and its analouges and prodrugs can increrase total outflow facility in monkeys and human ( a comination of trabecular, uveoscleral and pseudo- facililty ) less consistent finding is an increase in trabecular outflow facility “ with a lot of controversies”.
 less consistent finding is an increase in trabecular outflow facility with a lot of controversies .")
30
Trabecular outflow facility is not always increased following topical treatment with PG analogs but evidence is building that the effect is real and not unique to any one drug of this class. Latanoprost, travoprost, bimatoprost, and unoprostone all have been found to significantly increase trabecular outflow facility in at least one clinical study* * Update on the Mechanism of Action of Topical Prostaglandins for Intraocular Pressure Reduction doi:10.1016/j.survophthal.2008.08.010

31
Latanoprost (Xalatan) Latanoprost is a prostaglandin F2α analogue. Its chemical name is isopropyl - (Z) -7 [(1R,2R,3R,5S) 3,5-dihydroxy-2-[(3R)-3-hydroxy-5-phenylpentyl] cyclopentyl] -5-heptenoate. Its molecular formula is C26 H40 O5 and its chemical structure is:
 -7 [(1R,2R,3R,5S) 3,5-dihydroxy-2-[(3R)-3-hydroxy-5-phenylpentyl] cyclopentyl] -5-heptenoate. Its molecular formula is C26 H40 O5 and its chemical structure is:.")
32
Latanoprost is a colorless to slightly yellow oil & Benzalkonium chloride, 0.02% is added as a preservative.

33
Action: Reduce IOP by increasing the outflow through uveoscleral channels Lowers IOP in 3- 4 hrs after instillation Generics Latanaprost (0.005% Sol.) Usage: Once daily at bedtime Brands Xalatan Glaucoma Drugs Prostaglandin Analogs
 Usage: Once daily at bedtime Brands Xalatan Glaucoma Drugs Prostaglandin Analogs")
35
Bimatoprost (LUMIGAN) Bimatoprost, an amide that is classified as a prostamide, ( so it is not a prostaglandin but it acts on FP prostanoid receptor) The free acid of bimatoprost is identical to that of latanoprost with exception of a double instead of a single bond at the carbon13-14 position
 Bimatoprost, an amide that is classified as a prostamide, ( so it is not a prostaglandin but it acts on FP prostanoid receptor) The free acid of bimatoprost is identical to that of latanoprost with exception of a double instead of a single bond at the carbon13-14 position")
37
The free acid of bimatoprost is known to be a very potent FP receptor agonist The hydrolysis of bimatoprost have been demonstrated in human corneal tissue in vitro. Enzymes including amidases,peptidases and fatty acid amide hydrolases capable of hydrolysing bimatoprost to its free acid and activate FP prostanoid receptor

38
Bimatoprost appears to reduce the IOP of patients who are unresponsive to latanoprost. suggesting that the prostamide bimatoprost and the FP receptor agonist latanoprost stimulate different receptor populations. This is consistent with studies on isolated iridial cells where bimatoprost stimulated an entirely different cell population to those sensitive to PGF 2α and bimatoprost acid. An equally plausible explanation is that some eyes may be deficient in corneal esterase and thus are not able to adequately convert the prodrug latanoprost into its free acid active form.

39
Action: –Reduce IOP by increasing the outflow through uveoscleral channels Generics –Bimatoprost (0.03% Sol.) Usage: –Once daily at bedtime –Should NOT be used under 18 yrs of age. Brands –Lumigan Glaucoma Drugs Prostaglandin Analogs

40
Travoprost (TRAVATAN) Travoprost is a PGF2α analog, is an isopropyl ester of the enantiomer of fluprostenol. It is structurally similar to other f2α anlogs. It is a selective FP prostanoid receptor agonist.

42
Action: –Reduce IOP by increasing the outflow through uveoscleral channels –Lowers IOP in 2 - 3 hrs after instillation Generics –Travoprost (0.004% Sol.) Usage: –Once daily at bedtime Brands –Travatan Glaucoma Drugs Prostaglandin Analogs
 Usage: –Once daily at bedtime Brands –Travatan Glaucoma Drugs Prostaglandin Analogs")
44
Pharmacokinetics Reduction of the intraocular pressure starts approximately 3 to 4 hours after administration and the maximum effect is reached after 8 to 12 hours. XALATAN may be used concomitantly with other topical ophthalmic drug products to lower intraocular pressure. If more than one topical ophthalmic drug is being used, the drugs should be administered at least five (5) minutes apart
 minutes apart.")
45
Absorption: Latanoprost is absorbed through the cornea where the isopropyl ester prodrug is hydrolyzed to the acid form to become biologically active. Studies in man indicate that the peak concentration in the aqueous humor is reached about 2 hours after topical administration.

46
Pediatric Use: Safety and effectiveness in pediatric patients have not been established.

47
CONTRAINDICATIONS XALATAN has been reported to cause changes to pigmented tissues. The most frequently reported changes have been increased pigmentation of the iris and periorbital tissue (eyelid) and increased pigmentation and growth of eyelashes. These changes may be permanent.
 and increased pigmentation and growth of eyelashes. These changes may be permanent..")
48
WARNINGS / PRECAUTIONS Concerns related to adverse effects: Bacterial keratitis: Inadvertent contamination of multiple-dose ophthalmic solutions, has caused bacterial keratitis. Ocular effects: May permanently change/increase brown pigmentation of the iris, the eyelid skin, and eyelashes. In addition, may increase the length and/or number of eyelashes (may vary between eyes); changes occur slowly and may not be noticeable for months or years. Long-term consequences and potential injury to eye are not known.
; changes occur slowly and may not be noticeable for months or years. Long-term consequences and potential injury to eye are not known..")
49
ADVERSE REACTIONS SIGNIFICANT >10%: Ocular: Blurred vision, burning and stinging, conjunctival hyperemia, foreign body sensation, itching, increased pigmentation of the iris, and punctate epithelial keratopathy

50
1% to 10%: Cardiovascular: Chest pain, angina pectoris Dermatologic: Rash, allergic skin reaction Neuromuscular & skeletal: Myalgia, arthralgia, back pain Ocular: Dry eye, excessive tearing, eye pain, lid crusting, lid edema, lid erythema, lid discomfort/pain, photophobia Respiratory: Upper respiratory tract infection, cold, flu

51
Ocular: Change in iris color Burning Stinging Decreased VA Sensitivity to light Pain Hyperemia Systemic: Headaches Summary – Common Side Effects Prostaglandin Analogs

52
DRUG INTERACTIONS Bimatoprost: The concomitant use of Latanoprost and Bimatoprost may result in increased intraocular pressure. Risk D: Consider therapy modification

53
Thank You..

Similar presentations



















. 2. *The sclera is the.>")






