Download presentation
Presentation is loading. Please wait.

1
Metabolic Disorders Inborn Errors Of Metabolism
DR. ABDULLAH ALOMAIR MB ChB, MRCP (Edin), FRCP (Edin.), DCH (Glas.) Associate Professor of Pediatrics Consultant Pediatrician Department of Pediatrics PRESIDENT SAUDI PEDIATRIC ASSOCIATION
, FRCP (Edin.), DCH (Glas.) Associate Professor of Pediatrics. Consultant Pediatrician. Department of Pediatrics. PRESIDENT. SAUDI PEDIATRIC ASSOCIATION.")
2
Inborn Errors Of Metabolism
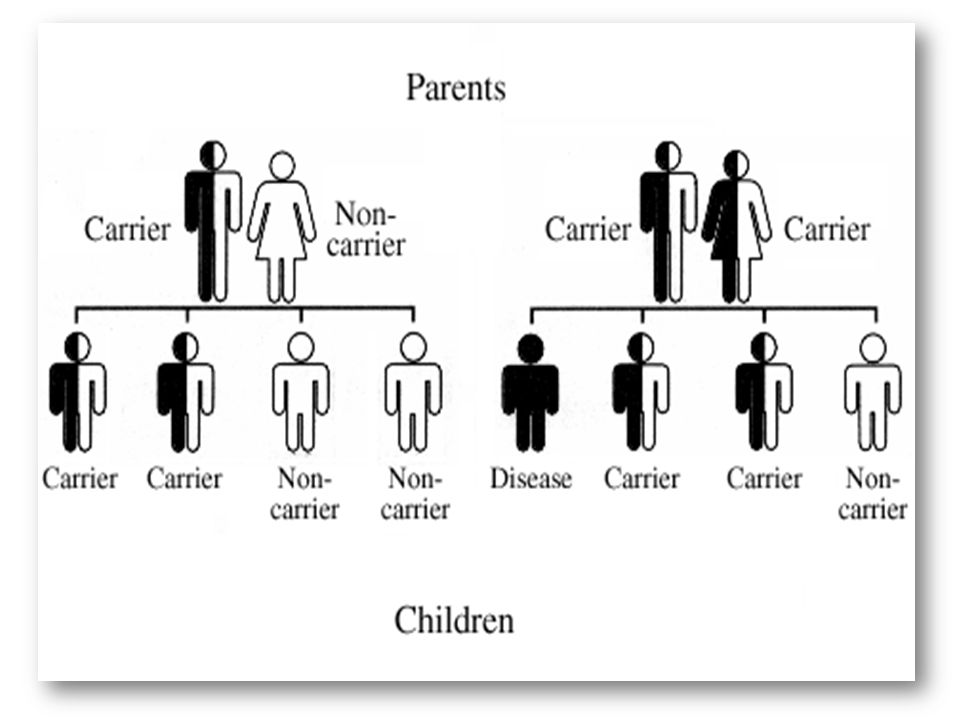
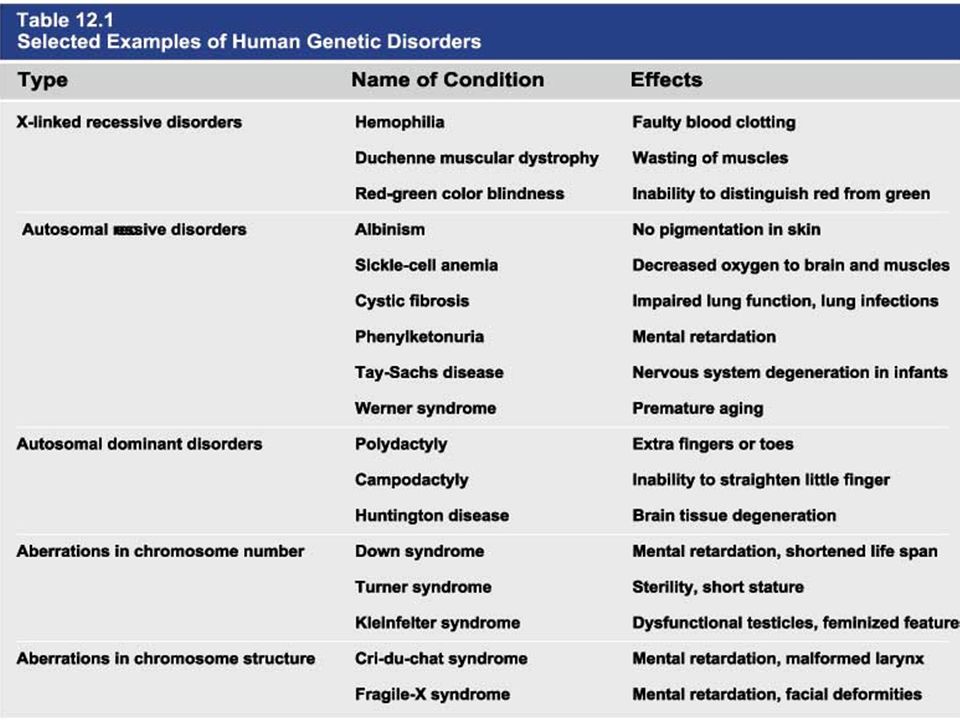
Metabolic Disorders Inborn Errors Of Metabolism Inborn Errors Of Metabolism (IEM) -A large group of hereditary biochemical diseases. -In autosomal dominant disorders, the structural abnormality dominates over the chemical abnormality. -Specific gene mutation cause abnormal or missing proteins that lead to altered function.
 -A large group of hereditary biochemical diseases. -In autosomal dominant disorders, the structural abnormality dominates over the chemical abnormality. -Specific gene mutation cause abnormal or missing proteins that lead to altered function.")
3
Pathophysiology SINGLE GENE DEFECTS in synthesis or catabolism of proteins, carbohydrates, or fats. Defect in an ENZYME or TRANSPORT PROTEIN , which results in a block in a metabolic pathway. EFFECTS : - toxic ACCUMULATION of substrates before the block, - intermediates from ALTERNATIVE pathways - defects in ENERGY production and utilization caused by a deficiency of products beyond the BLOCK. Every metabolic disease has several forms that vary in AGE OF ONSET , clinical severity and, often, MODE OF INHERITANCE.

6
Classification Transient Hyperammonemia of Newborn
Inborn Errors of Metab: Organic Acidemias Fatty Acid Oxidation def Urea Cycle Defects Amino Acidurias Non-ketotic Hyperglycinemia Molybdenum Cofactor Deficiency Sulfite Oxidase Deficiency Metal Storage Disorders: Cholesterol Disorders: Leukodystrophies, other… Krabbe disease Mitochondrial Disorders Glycogen Storage Disorders Hyperinsulinism Carbohydrate Disorders Lysosomal Disorders Mucopolysaccharidoses (X-linked Hunter’s, Hurler’s) Gaucher disease Tay-Sachs Disease Peroxisomal Disorders Zellwegger’s (Cerebro-Hepato-renal) X-linked Adrenoleukodystrophy
 Gaucher disease. Tay-Sachs Disease. Peroxisomal Disorders. Zellwegger’s (Cerebro-Hepato-renal) X-linked Adrenoleukodystrophy.")
7
Metabolic Disorders Due to inherited reduced activities of proteins involved in the synthesis, breakdown or transport of amino acids, organic acids, fats, carbohydrates and complex macromolecules. Most are autosomal recessive due to mutations that result in reduced enzyme activity or reduced amount of enzyme. Pathogenesis may include: accumulation of a toxic intermediate, reduced amount of a necessary end product or activation of an alternate pathway.

8
Metabolic Disorders Features suggestive of metabolic disorder :
From history: Parental history : Consanguineous parents Previous unexplained neonatal deaths Particular ethnic group (in certain diseases)
")
9
Metabolic Disorders Features suggestive of metabolic disorder :
Examination findings: Organomegaly (e.g. hepatomegaly) in the absence of viral infection. Cardiac disease Ocular involvement (e.g. cherry red spot) Skin manifestations e.g. pigmentations. Unusual odour. Due to change in the chemicals of the urine. Non-specific neurological findings. In a non-meningitis child you have to think of metabolic disorders.
 in the absence of viral infection. Cardiac disease. Ocular involvement (e.g. cherry red spot) Skin manifestations e.g. pigmentations. Unusual odour. Due to change in the chemicals of the urine. Non-specific neurological findings. In a non-meningitis child you have to think of metabolic disorders.")
10
Neonatal and Post Neonatal Presentation
Normal-appearing child at birth (some conditions are associated with dysmorphic features) poor feeding lethargy vomiting seizures coma unusual odour Hypoglycaemia is very dangerous, acidosis (in some defects)
 poor feeding. lethargy. vomiting. seizures. coma. unusual odour. Hypoglycaemia is very dangerous, acidosis (in some defects)")
11
Neonatal and Post Neonatal Presentation
Encephalopathy without the presence of infection. Developmental regression Reye syndrome ( damage of the brain and liver eventually leading to encephalopathy). Motor deficits Seizures Intermittent episodes of vomiting, acidosis, hypoglycaemia and/or coma triggered by stress e.g. infections, surgery.
. Motor deficits. Seizures. Intermittent episodes of vomiting, acidosis, hypoglycaemia and/or coma triggered by stress e.g. infections, surgery.")
12
Newborn Screening the earlier its detected the fewer the complications
PKU - in NICU even if not advanced to full feeds Galactosemia Hypothyroidism Hemoglobinopathies Biotinidase defic, CAH (21-OH’ase def), Maple syrup urine disease ( MSUD ) - GUTHRIE TEST: it’s a cheap test that requires only one drop of blood to check for multiple metabolic disorders.
, Maple syrup urine disease ( MSUD ) - GUTHRIE TEST: it’s a cheap test that requires only one drop of blood to check for multiple metabolic disorders.")
13
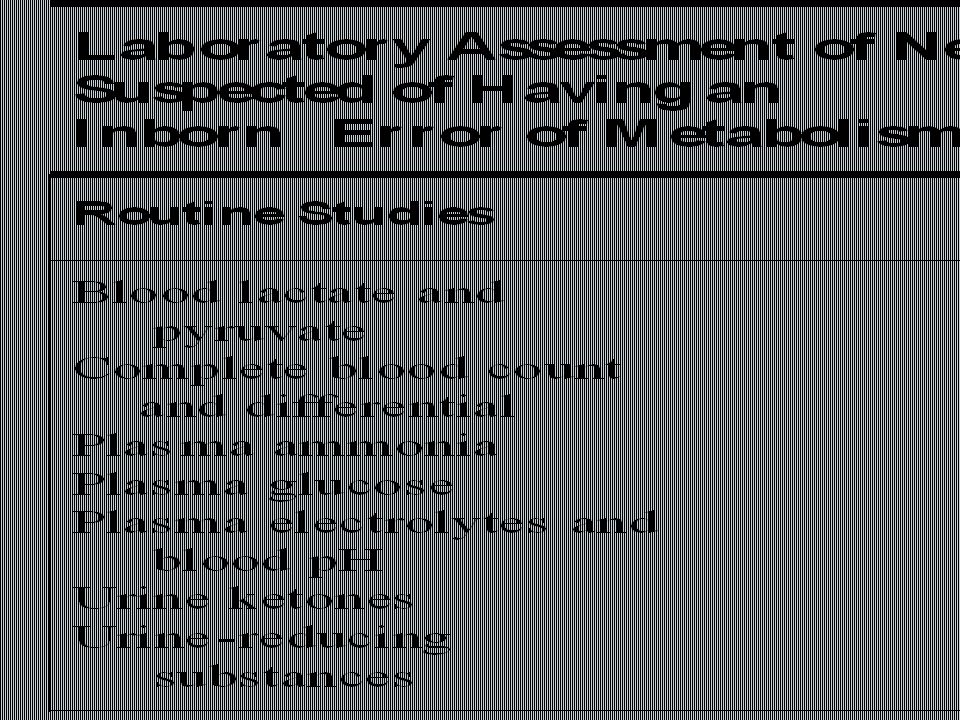
PROCEDURES FOR DIAGNOSIC CONFIRMATION
Non – Specific Tests: Blood glucose, ammonia, bicarbonate and pH Peripheral Blood smear – WBC or bone marrow vacuolization , foam cells or granules. C.S.F. glycine , other amino acids , lactate. Amino acids shouldn’t be present in the CSF if its there it indicates a metabolic disorder. Specific Tests: Direct biochemical assays of metabolites or their metabolic by-products, or of an enzyme’s function. DNA studies Neuro-radiology Bone marrow transplantation is a treatment of both inborn errors of metabolism

14
Urine Odor Inborn Error of Metabolism
INBORN ERRORS OF AMINO ACID METABOLISM ASSOSIATED WITH ABNORMAL ODOR Urine Odor Inborn Error of Metabolism Sweaty feet Gultaric Acidemia Maple syrup Maple Syrup urine disease Boiled cabbage Hypermethioninemia Mousy or musty Phenylketonuria Rotten fish Trimethylaminuria

16
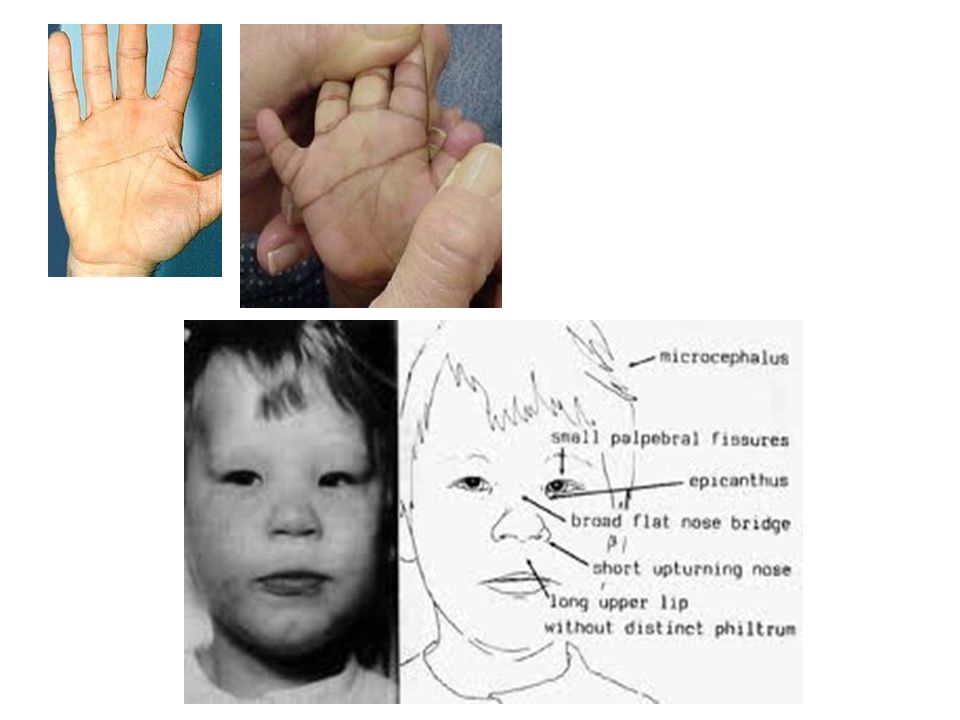
They may come with flattened mid-face, indistinct philtrum, low nasal bridge and single palmar crease. Small chin is called micrognathia

18
Low-set ears: >1/3rd of the ears lower than the line connecting the 2 pupils.
Low nasal bridge: common sign, which is also seen in Down.

19
MANAGEMENT OF IEM Genetic: Establish diagnosis. Carrier testing.
Pedigree analysis, risk counseling. Consideration of Prenatal diagnosis for pregnancies at risk.

20
PSYCHOSOCIAL , EDUCATIONAL , FAMILIAL
MANAGEMENT OF IEM PSYCHOSOCIAL , EDUCATIONAL , FAMILIAL Family counseling and support. Education to promote increased compliance with special form of therapy such as Protein – restricted diet. Assessment of community resources and support groups.

21
TREATMENT OF GENETIC DISEASES
Modify environment, e.g., diet, drugs Avoid known environmental triggers BMT Surgical, correct or repair defect or organ transplantation Modify or replace defective gene product, megadose vitamin therapy or enzyme replacement Replace defective gene Correct altered DNA in defective gene

22
Galactosemia

23
: Carbohydrates Galactosemia Enzyme deficiency:
Galactose-1-phosphate uridyl transferase deficiency. It is a rare autosomal recessive. Follows feeding with lactose containing (breast milk / formula) Patient feeds poorly , have vomiting, jaundice, hepatomegaly and hepatic failure Chronic liver disease Cataracts Developmental delay develop if condition is untreated., if they were given galactose free diet you will avoid the social and mental damage but they might complain of dyslexia.
 Patient feeds poorly , have vomiting, jaundice, hepatomegaly and hepatic failure. Chronic liver disease. Cataracts. Developmental delay develop if condition is untreated., if they were given galactose free diet you will avoid the social and mental damage but they might complain of dyslexia.")
24
CYSTIC FIBROSIS Cause : Loss of 3 DNA bases in a gene for the protein that transports Cl ions so salt balance is upset. Causes .a build up of thick mucus in lungs and digestive organs. It is diagnosed by sweat test: measuring the chloride concentration in the sweat

25
Phenyl Ketonuria (PKU)
AMINO ACID DISORDERS Phenyl Ketonuria (PKU) Phenylalanine Phenylalanine Tyrosine Hydroxylase Phenyl ethylamine Phenyl pyruvic acid Phenyl pyruvic acid is what gives the urine its smell because its ketonic and acidic.
 Phenylalanine. Phenylalanine. Tyrosine. Hydroxylase. Phenyl ethylamine Phenyl pyruvic acid. Phenyl pyruvic acid is what gives the urine its smell because its ketonic and acidic.")
26
Phenylketonuria PKU

27
PKU Hyperactivity, athetosis, vomiting. Blond.
DIAGNOSIS CLINICAL FEATURES Screening : Guthrie Test. High Phenylalanine > 20 mg/dl. High Phenyl pyruvic acid. Hyperactivity, athetosis, vomiting. Blond. Seborric dermatitis or eczema skin. Hypertonia. Seizures. Severe mental retardation. Unpleasant odor of phenyl acetic acid. TREATMENT DIET. BH4 (Tetrahydrobiopterin). L – dopa and 5- hydroxytryptophan.
. L – dopa and 5- hydroxytryptophan.")
28
PKU

29
Albinism

30
Iris had fibrous tissue, and it’s colourless and is red due to vessels.

31
Homocystinuria Elevated homocystine levels affect collagen , result in a Marfanoid habitus, ectopia lentis but lens dislocation in homocystinemia is downward unlike in marfan its upward, mental retardation and strokes, its harmful to the bones and body. Araachnodyctly.

32
Homocystinuria METHIONINE CYSTATHIONINE Cysathionine Synthatase
DIAGNOSIS: High methionine and homocystine. TREATMENT: High dose of B6 and Folic Acid. Low methionine and high cystine diet, Betain (trimethylglycine)
")
33
Homocystinuria

34
Amino acid disorders : Urea cycle defects and hyperammonemia
All present with lethargy, seizures, ketoacidosis, neutropenia, and hyperammonemia Ornithine carbamyl transferase (OTC) deficiency Carbamyl phosphate synthetase deficiency Citrullinemia Arginosuccinic Aciduria Argininemia Transient tyrosinemia of prematurity
 deficiency. Carbamyl phosphate synthetase deficiency. Citrullinemia. Arginosuccinic Aciduria. Argininemia. Transient tyrosinemia of prematurity.")
35
First Steps in Metabolic Therapy for IEM
Reduce precursor substrate load Provide caloric support Provide fluid support Remove metabolites via dialysis Divert metabolites Supplement with cofactor(s)
")
36
Therapeutic Measures for IEM
D/C oral intake temporarily Usually IVF’s with glucose to give mg/kg/min glu and at least 60 kcal/kg to prevent catabolism (may worsen pyruvate dehydrogenase deficiency) Bicarb/citrate Carnitine/glycine Na Benzoate/arginine/citrulline Dialysis--not exchange transfusion Vitamins--often given in cocktails after labs drawn before dx is known Biotin, B6, B12, riboflavin, thiamine, folate
 Bicarb/citrate Carnitine/glycine. Na Benzoate/arginine/citrulline. Dialysis--not exchange transfusion. Vitamins--often given in cocktails after labs drawn before dx is known. Biotin, B6, B12, riboflavin, thiamine, folate.")
37
Important IEM Treatment supplements:
Carnitine for elimination of Organic Acid through creation of carnitine esters. Sodium Benzoate, phenylacetate and phenylbutyrate for Hyperammonemia elimination.

38
CARNITINE METABOLISM An essential nutrient found in highest concentration in red meat. Primary function : Transport long-chain fatty acids into mitochondria for oxidation. Carnitine supplementation in fatty acid oxidation disorders and organic acidosis may augment excretion of accumulated metabolites , but may not prevent metabolic crises in such patients . Carnitine is an endogenous metabolite but can be given as supplementations.

39
CARNITINE METABOLISM Primary defects of carnitine transport manifest as Reye syndrome , cardiomyopathy or skeletal myopathy with hypotonia Secondary carnitine deficiency is due to diet ( esp. I.V alimentation or ketogenic diet ) , renal losses , drug therapy ( esp. valproic acid) and other metabolic disorders ( esp. disorders of fatty acid oxidation and organic acidemias ) Prognosis depends on the cause of the carnitine abnormality. Free and esterified carnitine can be measured in blood. Oral or I.V. L-carnitine is used in carnitine deficiency or lnsufficiency in doses of mg/kgm/day or higher.
 , renal losses , drug therapy ( esp. valproic acid) and other metabolic disorders ( esp. disorders of fatty acid oxidation and organic acidemias ) Prognosis depends on the cause of the carnitine abnormality. Free and esterified carnitine can be measured in blood. Oral or I.V. L-carnitine is used in carnitine deficiency or lnsufficiency in doses of mg/kgm/day or higher.")
40
ORGANIC ACIDEMIA Disorder Enzyme Methyl malonic Acidemia.
Propionic Acidemia. Multiple carboxylase deficiency. Ketothiolase deficiency . Enzyme Methyl malonyl COA mutase. Propionyl COA Carboxylase. Malfunction of all carboxylase. 2 methylacetyl COA thiolase def.

41
ORGANIC ACIDEMIA Clinical Features Treatment Vomiting, ketosis.
Thrombocytopenia , neutropenia. Osteoporosis. Mental retardation. Hydration / alkali. Calories to catabolic state. Exchange transfusion. Low protein diet.

42
ORGANIC ACIDEMIA

43
LYSOSOMAL STORAGE DISORDERS
Glycogen Storage Diseases Sphingolipidoses common in eastern jews (Lipidoses And Mucolipidoses) Mucopolysaccharidoses
 Mucopolysaccharidoses.")
44
Lysosomal Storage Disease
Enzyme Defiency Major Accumulating Metabolite Glycogenosis Type II (Pompe disease) Glucosidase Glycogen Sphingolipidoses GM1 gangliosidoses GM2 gangliosidoses Tay-Sachs disease Gaucher disease Niemann-Pick disease β-galactosidase Hexosaminidase A Glucocerebrosidase Sphingomyelinase GM1 gangliosides, galactose-containing oligosaccharides GM2 ganglioside Glucocerebroside Sphingomyelin Mucopolysaccharidoses MPS I H (Hurler) MPS II (Hunter) (X-linked recessive) α-L-Iduronidase L-Iduronosulfate sulfatase Heparan sulfate Dermatan sulfate
 Glucosidase. Glycogen. Sphingolipidoses. GM1 gangliosidoses. GM2 gangliosidoses. Tay-Sachs disease. Gaucher disease. Niemann-Pick disease. β-galactosidase. Hexosaminidase A. Glucocerebrosidase. Sphingomyelinase. GM1 gangliosides, galactose-containing oligosaccharides. GM2 ganglioside. Glucocerebroside. Sphingomyelin. Mucopolysaccharidoses. MPS I H (Hurler) MPS II (Hunter) (X-linked recessive) α-L-Iduronidase. L-Iduronosulfate sulfatase. Heparan sulfate. Dermatan sulfate.")
45
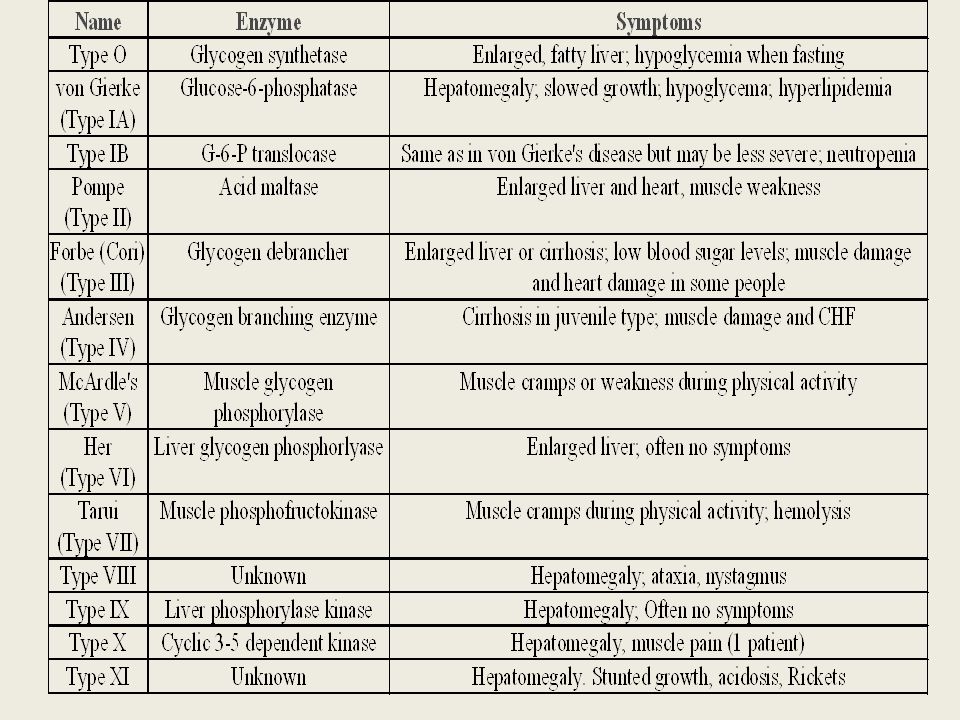
Glycogen Storage Diseases

47
Principle Groups of Glycogen Storage Diseases

48
Von Gierke Disease

49
LYSOSOMAL STORAGE DISORDERS
Lipidoses And Mucolipidoses

50
In gaucher liver is enlarged but the rest of the body is very thin
Gauch. cell

51
In gaucher you see the cherry red spot appearance in the macula

52
Sandhoff - Dense thalam

53
Cerebral palsy --- scissoring of the legs
Lipid accumalation around the retinal arteries and veins Lipid-retina

54
LYSOSOMAL STORAGE DISORDERS
Mucopolysaccharidoses

55
Clinical And Pathological Ultra structure Of Mucopolysaccharidoses
Disease Clinical Manifestation Ultrastructure of Stored Material MPS type I Hurler Earliest, most severe developmental regression coarse facial features Hepatosplenomegaly dystosis of bone cardiac involvement corneal clouding present in hurler but absent in hunter Fibrillogranular mucopolysaccharides in cells of viscera and brain MPS type II Hunter X-linked Later developmental regression hepatosplenomegaly minimal corneal clouding

56
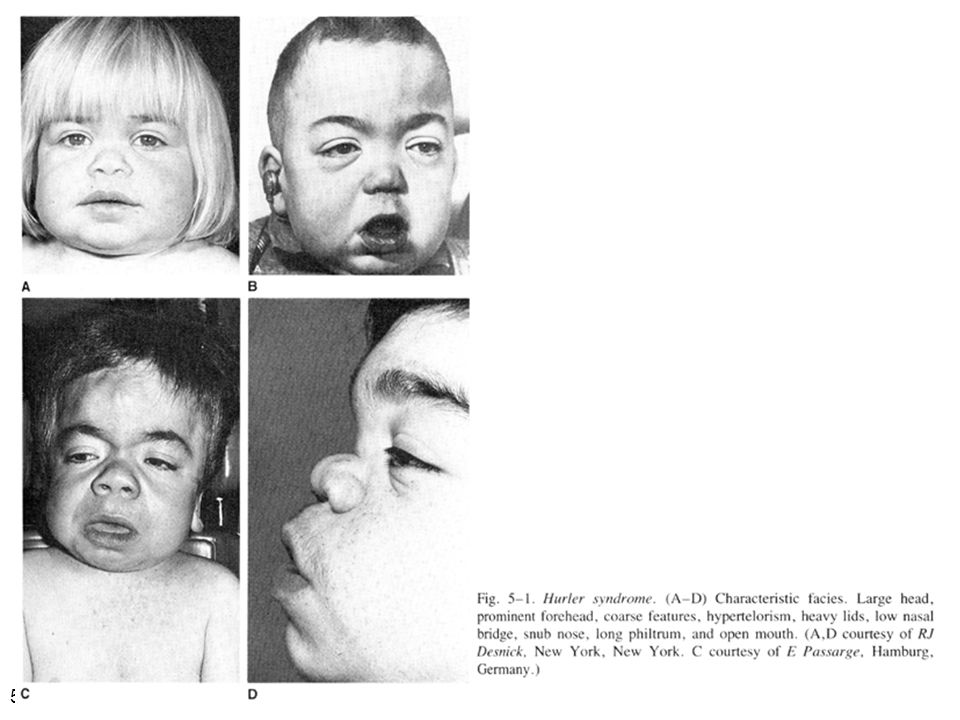
Hurler’s

57
In hurler : Nasal bridge is depressed , increase distance of philthrum , epicanthal folds, bossing of the head , thick eyebrows , upturn nostrils Hurler’s

59
Mcopolysacch. Morquio

60
PEROXISOMAL DISORDERS
Peroxisomes = Subcellular organelles involved in various essential anabolic or catabolic processes, biosynthesis of Plasmalogens and bile acids. Due to dysfunction of a single or multiple peroxisomal enzymes, or to failure to form or maintain a normal number of functional peroxisomes.

61
PEROXISOMAL DISORDERS
Clinical Manifestations: Hypotonia. Dysmorphia. Psychomotor delay and seizures. Hepatomegaly. Abnormal eye findings such as retinitis pigmentosa or cataract. Hearing impairment.

62
Peroxisomal Disorders
Zellweger Syndrome is autosomal recessive disorder. (Cerebro-hepato-renal syndrome) Typical and easily recognized dysmorphic facies. Progressive degeneration of Brain/Liver/Kidney, with death ~6 mo after onset. When screening for PDs. obtain serum Very Long Chain Fatty Acids- VLCFAs
 Typical and easily recognized dysmorphic facies. Progressive degeneration of Brain/Liver/Kidney, with death ~6 mo after onset. When screening for PDs. obtain serum Very Long Chain Fatty Acids- VLCFAs.")
63
Zellweger

64
PEROXISOMAL DISORDERS
Diagnosis: Immunochemical studies for Peroxisomes. V. Long Chain FA ( VLCFA ) level. Chor. Vill. Samp. or/ amniocytes culture Plasmalogens synthesis. Treatment: Supportive, multidisciplinary interventions. Diet: VLCFA, phytanic acid. Organ transplantation.
 level. Chor. Vill. Samp. or/ amniocytes culture Plasmalogens synthesis. Treatment: Supportive, multidisciplinary interventions. Diet: VLCFA, phytanic acid. Organ transplantation.")
65
Peroxisomal Disorders
GROUP I : BIOGENSIS OF PEROXISOME GROUP III : POSITIVE PEROXISOMES BUT MULTIPLE DEFECTIVE ENZYME Zellweger syndrome (cerebrohepatorenal syndrome). Neonatal adrenoleukodystrophy. Infantile Refsum disease. Hyperpipecolic acidemia. Zellweger – Like. Pseudo – infantile Refsum disease. Rhizomelic chondro-dysplasia punctata GROUP II : PERSOXISOMAL ENZYME DEFECTS Refsum disease. X - linked Adreno-Leuko-Dystrophy. Pseudo – Zellweger syndrome. Hyperoxaluria….etc.
. Neonatal adrenoleukodystrophy. Infantile Refsum disease. Hyperpipecolic acidemia. Zellweger – Like. Pseudo – infantile Refsum disease. Rhizomelic chondro-dysplasia punctata. GROUP II : PERSOXISOMAL ENZYME DEFECTS Refsum disease. X - linked Adreno-Leuko-Dystrophy. Pseudo – Zellweger syndrome. Hyperoxaluria….etc.")
66
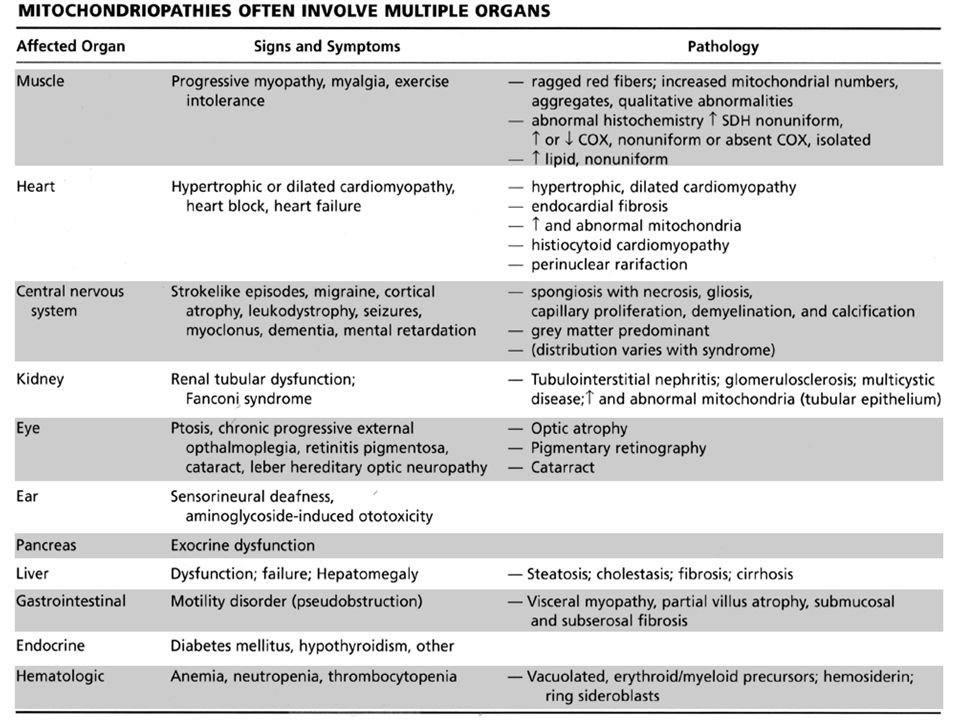
Mitochondrial Disorders
Classically involve mutations in mitochondrial DNA Follow a maternal pattern of inheritance Highly variable with regard to penetrance and expressivity based on the variability in tissue distribution of abnormal mitochondria

67
Mitochondrial Syndromes Presenting in Childhood to Adult
Most Common Clinical Presentation Other Clinical Features Mt DNA Defect MELAS: myopathy, encephalopathy, lactic acidosis and stroke-like episodes Stroke-like episodes in the first and second decade of life often associated with migraine headache, blood lactate Deafness, myopathy, diabetes mellitus mtDNA mutations at 3243, tRNA mutations MERRF: Myoclonic epilepsy with ragged red fibers Progressive myoclonic epilepsy Ataxia, myopathy deafness, short stature MtDNA A8344G tRNA mutation NARP: Neurogenic weakness, ataxia and retinitis pigmentosa Peripheral neuropathy, myopathy, seizures Leigh syndrome MtDNA Complex V deficiency

69
Transient Hyperammonemia of Newborn:
Markedly high NH4 in an infant less than 24 HOL (hours of life), or first 1-2 DOL (day of life) before protein intake occurs. Often in context of large, premature infant with symptomatic pulmonary disease. Very sick infant. Unknown precipitant, unknown etiology (possible slow delayed urea cycle initiation), with potential for severe sequelae (20-30% death, 30-40% abnl dev.) if not treated. Does not recur after being treated.
, or first 1-2 DOL (day of life) before protein intake occurs. Often in context of large, premature infant with symptomatic pulmonary disease. Very sick infant. Unknown precipitant, unknown etiology (possible slow delayed urea cycle initiation), with potential for severe sequelae (20-30% death, 30-40% abnl dev.) if not treated. Does not recur after being treated.")
70
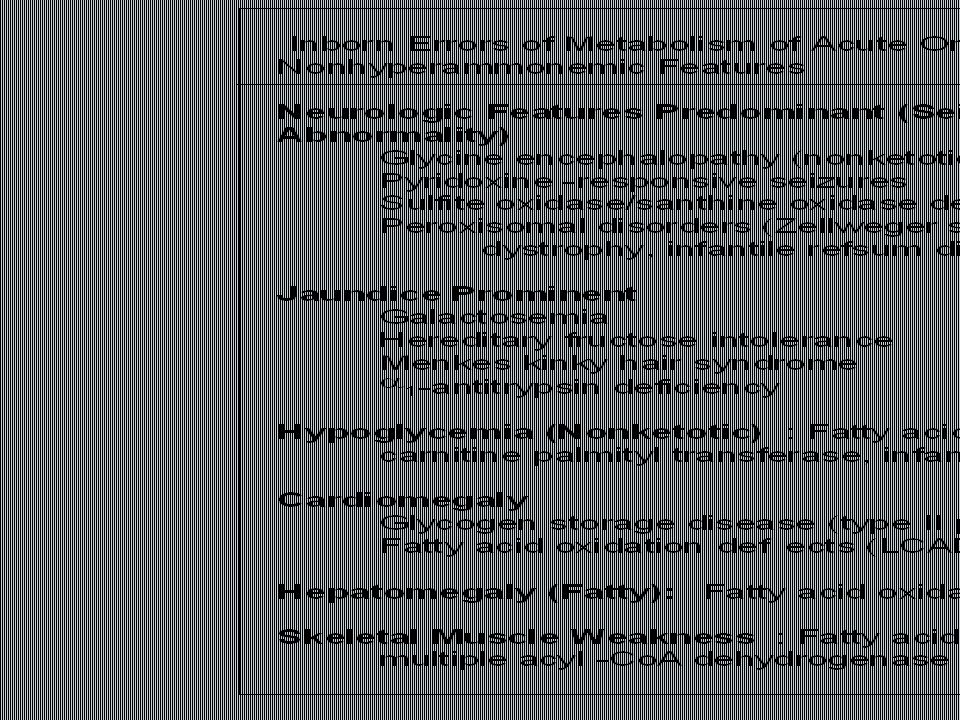
Clinical Presentation of Amino Acid Disorders
Clinical Abnormality Abnormal Amino Acid Presumptive Diagnosis Acute neonatal presentation with ketoacidosis Leucine, isoleucine, valine Organic Acid Disorders Maple syrup urine disease Methylmalonic acidemia Propionic acidemia Isovaleric acidemia Acute neonatal presentation with hyperammonemia Arginine, Citrulline Urea cycle disorders Ornithine transcarbamylase deficiency Argininosuccinate synthase deficiency Argininosuccinate lyase deficiency Marfanoid, strokes, ectopia lentis, mental retardation Homocystine & methionine Homocystinuria Severe developmental delay Phenylalanine Phenylketonuria

71
Organic and Amino Acid Disorders
Metabolic Profiles Organic and Amino Acid Disorders Predominanat Biochemical Clinical Findings Other Most Common Diagnosis KetoAcidosis Lethargy Odor Ammonia: Normal or slightly elevated Ketones: Elevated Glucose: Normal Maple syrup urine disease Acidosis Ammonia: Elevated Glucose: Normal or decreased Ketones: May be elevated Lactate: Slightly elevated Methylmalonic acidemia Propionic acidemia Isolvaleric acidemia Lactic Acidosis Acidosis: Usually present Ammonia: Normal or slightly elevated Ketones: May be elevated Pyruvate dehydrogenase Pyruvate carboxylase deficiency Respiratory chain disorder Hypoglycemia Ammonia: Lactate Acidosis Ketones: Absent or inappropriately low Fatty acid oxidation defects Hyperammonemia Acidosis: Absent Respiratory Alkalosis Urea cycle disorders Newborn screening is available dependent on population frequency for some Expanded newborn screening for fatty acid defects recently offered

72
CHILDREN AFTER THE NEONATAL PERIOD
Clinical Manifestation Mental retardation, Macro/Microcephaly. Coarse facial features/dysmorphia. Developmental regression. Convulsion. Myopathy / cardiomyopathy. Recurrent emesis with coma and hepatic dysfunction. Hypertonia / hypotonia. Failure to thrive. Ophthalmic – related problems : e.g. cataract, corneal cloudiness, cherry red spot, optic atrophy. Renal failure or renal tubular acidosis.

76
Management of IEM - NICU
Stop nutrient triggering disorder e.g. protein, galactose Give high-energy intake NICU care to correct tissue perfusion, dehydration, acidosis Hyperammonemia Rx with Na benzoate, Na phenylbutyrate, arginine Dialysis Insulin to control hyperglycemia and reduce catabolism Vitamins e.g Biotin, B6, B12 Specific therapy e.g. carnitine, glycine

77
MEDICAL Dependent on diagnosis and severity:
Dietary or vitamin therapy Drug therapy BMT Avoid known environmental triggers Surgery

Similar presentations












.>")




 IS A METABOLISM DISORDER PASSED DOWN THROUGH FAMILIES IN WHICH THE BODY CANNOT BREAK DOWN CERTAIN PARTS OF PROTEINS. URINE.>")

