Download presentation
Presentation is loading. Please wait.

1
Tinnitus Diagnosis and Treatment Hossein Talebi; PhD of Audiology Assistant Professor of Audiology Isfahan University of Medical Sciences

2
Introduction Tinnitus is defined as sensations of hearing in the absence of external sounds

3
The burden of tinnitus

4
Introduction Prevalence increases with age 80% of people don’t seek help 6-8% of those affected are severe 40% of patients experience depression Can vary between barely perceptible noise to a deafening roar Very little is understood about its cause or cure

5
Sound features of tinnitus NOISE CRITERIAPOSSIBLE FEATURES OnsetSudden, gradual PatternPulsatile, intermittent, constant, fluctuating SiteRight or left ear, both ears, within head LoudnessWide range, varying over time QualityPure tone, noise, polyphonic PitchVery high, high, medium, low

6
Tinnitus sufferers Ludwig van Beethoven Vincent van Gogh Charles Darwin Neil Young Eric Clapton Ronald Regan

7
Types of Tinnitus Objective: caused by sounds generated somewhere in the body Subjective: perception of meaningless sounds without any physical sound being present Auditory hallucinations: perceptions of meaningful sounds such as music or speech

8
Causes

9
Effects of Tinnitus Concentration Hearing Insomnia Psychological

10
Ear Anatomy

12
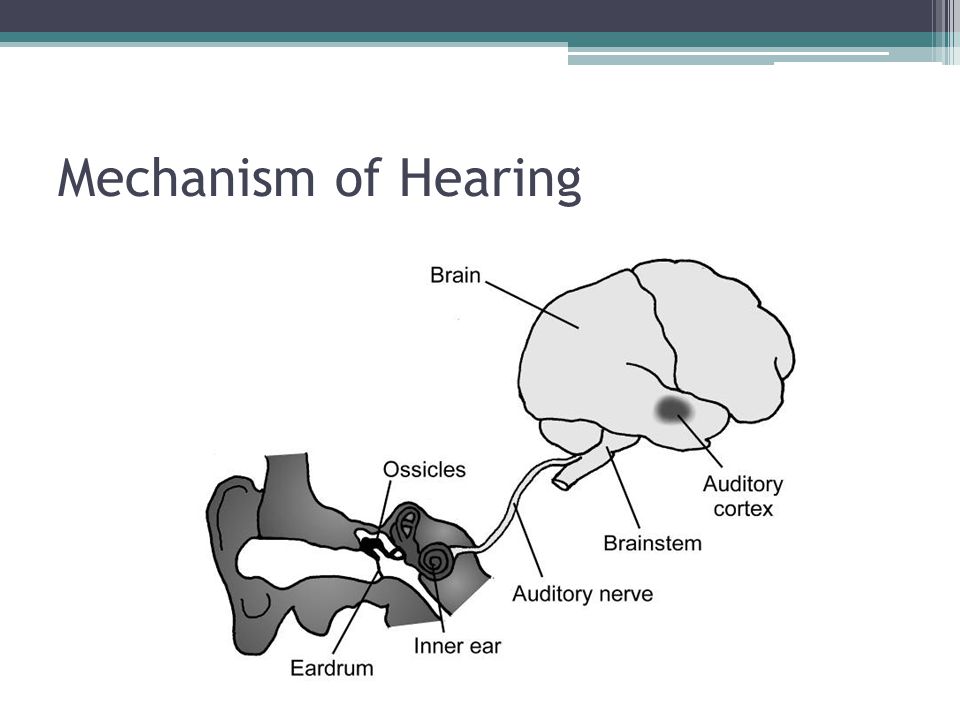
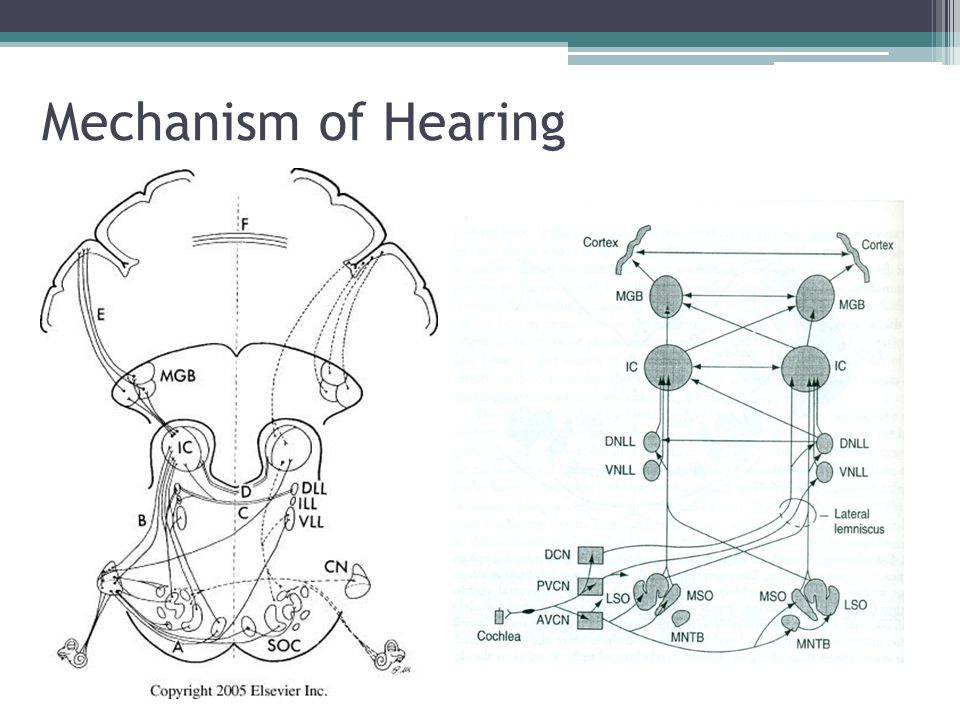
Mechanism of Hearing

15
Pathophysiology Poorly understood Range of theories from loss of outer hair cell function to increased spontaneous activity of central nerves Can be generated from any part of the auditory system from the ear to the Central Nervous System (CNS) This then may become modified by the CNS
 This then may become modified by the CNS")
16
Peripheral events lead to central neurological changes

17
Brain response to auditory deprivation Patients with tinnitus exhibit enhanced auditory sensitivity This is caused by hyperactivity of the auditory central nervous system In patients with tinnitus and hearing loss, the tinnitus pitch and the hearing loss frequency spectrum are usually matched DECREASED SOUND INPUT INCREASED SOUND SENSITIVITY

18
Tinnitus is a balance of sensory input and spontaneous activity The decreased input from the cochlea, due to outer hair cell damage, results in readjustments in the central auditory system resulting in abnormal neural activity including hyperactivity, bursting discharges and increases in neural synchrony. TINNITUS AUDITORY DEPRIVATION AND CENTRAL GAIN ALTERED SPONTANEOUS NEURONAL ACTIVITY

19
Pathophysiology When the perception of tinnitus is associated with negative reinforcement, the autonomic nervous system is activated. Physiological and psychological reactions then lead to enhancement of the tinnitus signal Often compared with chronic pain

20
Pathophysiology

21
Psychological associations with tinnitus

22
A Team Approach Thorough evaluation to rule out significant pathology Treatment of other ear disorders eg. infection Explanation of test results Explanation of tinnitus mechanisms Treatment options Treatment of severe psychological disorders Follow-up

23
Differential Diagnosis Idiopathic (most common) Outer ear disease – Wax, foreign body, infection Middle ear disease – Infection, perforated eardrum, ossicular problems, tumour
 Outer ear disease – Wax, foreign body, infection Middle ear disease – Infection, perforated eardrum, ossicular problems, tumour")
24
Differential Diagnosis Inner ear disease – Presbyacusis (older age hearing loss) – Meniere’s disease – Acoustic neuroma – Noise exposure – Drugs
 – Meniere’s disease – Acoustic neuroma – Noise exposure – Drugs")
26
Evaluation of Tinnitus Thorough history Duration, nature, effects Non vs. pulsatile Noise exposure Other ear symptoms Ear examination Rule out outer/middle ear disease Tuning fork tests

27
Normal Ear vs. Diseased Ear

28
Evaluation of Tinnitus Audiological (hearing) Tests Audiogram, tympanogram Specialized hearing tests: SOAE, ECochG, ABR MRI Associated symptoms Asymmetric hearing loss
 Tests Audiogram, tympanogram Specialized hearing tests: SOAE, ECochG, ABR MRI Associated symptoms Asymmetric hearing loss")
29
Evaluation - Subjective Tinnitus Audiometry - assymetrical hearing loss, unilateral tinnitus - MRI r/o post fossa Complete questionnaire for perceived severity:THI

30
Measurement of Tinnitus Pitch, loudness, minimum masking level, residual inhibition/post masking Minimum masking level most clinical use Pitch - match most prominent pure tone, poor reliability, octave difference Loudness - Adjust pure tone to tinnitus Most < 7 dB SL, may be 2 dB

31
Measurement of Tinnitus Minimal masking level - number of decibels to cover tinnitus Residual inhibition - response of patients tinnitus post masking

32
ENT Referral

33
Acoustic Neuroma

34
Treatment Aim to improve habituation rather than “cure” tinnitus Most people don’t seek treatment Multitude of potential treatments Problems with scientific evidence

35
Treatment Basic advice Hearing Aid Tinnitus Masking Device Tinnitus Instrument Tinnitus Retraining Therapy Psychological Treatment Medication Alternative Treatments

36
Basic Advice Reassurance The first step is to understand the problem Avoid aggravating factors eg. noise, NSAIDs Decreased intake of stimulants eg. caffeine and nicotine Relaxation Avoiding silence White noise eg. Detuned radio

37
Treatment Basic advice Hearing Aid Tinnitus Masking Device Tinnitus Instrument Tinnitus Retraining Therapy Psychological Treatment Medication Alternative Treatments

38
Hearing Aids Essentially for poor hearing Increases ambient noise Decreases stress of poor hearing Various shapes and sizes Cost Limitations Up to 90% may benefit

39
Hearing Aids

40
Hearing aids are central to tinnitus management Reports of the use of hearing aids in the management of tinnitus go back over 60 years Because hearing loss is often associated with tinnitus, at least partial restoration of hearing should help to reduce the central gain in auditory perception that is a feature of tinnitus A recent scoping review of studies of hearing aids in tinnitus revealed that 17/18 publications showed improvements in tinnitus symptoms by fitting hearing aids

41
Treatment Basic advice Hearing Aid Tinnitus Masking Device Tinnitus Instrument Tinnitus Retraining Therapy Psychological Treatment Medication Alternative Treatments

42
Tinnitus Masking Device Essentially counteracts tinnitus Generate noise bands Tinnitus Instruments Combination of hearing aid and masker

43
Wide Band Noise Generators Emit ‘white noise’ Elimination of silence White noise boring: tendency to ignore Gives the tinnitus sufferer something tangible to work with Reduce the starkness of the tinnitus signal

44
Treatment Basic advice Hearing Aid Tinnitus Masking Device Tinnitus Instrument Tinnitus Retraining Therapy Psychological Treatment Medication Alternative Treatments

45
Tinnitus Retraining Therapy Based on evidence that a person can habituate to acoustic noise in the environment Goal is to weaken or remove the functional connections between the auditory pathways Key elements: counseling and sound therapy

46
Normal Condition

47
Tinnitus Condition

48
Counseling alone

49
Sound Therapy alone

50
Counseling and Sound Therapy

51
Tinnitus Retraining Therapy May take several months to take effect Minimum 12 months treatment Involves wearing ear noise generator, table top generator

52
Tinnitus Retraining Therapy

53
Treatment Basic advice Hearing Aid Tinnitus Masking Device Tinnitus Instrument Tinnitus Retraining Therapy Psychological Treatment Medication Alternative Treatments

54
Psychological Treatment Relaxation therapy Hypnosis Cognitive Behavioural Therapy Information, managing aggravating factors Applied relaxation Cognitive restructuring of thoughts and beliefs Sleep management advice Improvement in quality of life, not tinnitus itself Medication

55
Psychological and behavioural support INTERVENTIONDESCRIPTION Counselling and education Delivered in person, to groups and via the internet Variable results may depend on personal characteristics Cognitive behavioural therapy Designed to modify maladaptive behavioural and emotional responses One-to-one and group settings, delivered by psychologists or psychiatrists, or via internet Statistically significant reductions in severity of tinnitus symptoms (P<0.05) Relaxation therapy May help reduce tinnitus symptoms and depressive symptoms
 Relaxation therapy May help reduce tinnitus symptoms and depressive symptoms")
56
Treatment Basic advice Hearing Aid Tinnitus Masking Device Tinnitus Instrument Tinnitus Retraining Therapy Psychological Treatment Medication Alternative Treatments

57
Medications No approved drugs (European Medicines Agency [EMA] or US Food and Drug Administration [FDA]) Some psychopharmacological agents may help reduce the severity of psychological issues associated with tinnitus, and some may also lessen tinnitus symptoms DRUG CLASSEXAMPLES OF DRUGS USED IN TINNITUS Antidepressantstricyclics, selective serotonin reuptake inhibitors Antipsychoticssulpiride Mood stabilisersgabapentin, valproate Sedatives/hypnoti cs benzodiazepines
![Medications No approved drugs (European Medicines Agency [EMA] or US Food and Drug Administration [FDA]) Some psychopharmacological agents may help reduce the severity of psychological issues associated with tinnitus, and some may also lessen tinnitus symptoms DRUG CLASSEXAMPLES OF DRUGS USED IN TINNITUS Antidepressantstricyclics, selective serotonin reuptake inhibitors Antipsychoticssulpiride Mood stabilisersgabapentin, valproate Sedatives/hypnoti cs benzodiazepines](http://images.slideplayer.com/16/4904782/slides/slide_57.jpg "Medications No approved drugs (European Medicines Agency [EMA] or US Food and Drug Administration [FDA]) Some psychopharmacological agents may help reduce the severity of psychological issues associated with tinnitus, and some may also lessen tinnitus symptoms DRUG CLASSEXAMPLES OF DRUGS USED IN TINNITUS Antidepressantstricyclics, selective serotonin reuptake inhibitors Antipsychoticssulpiride Mood stabilisersgabapentin, valproate Sedatives/hypnoti cs benzodiazepines")
58
Treatment Basic advice Hearing Aid Tinnitus Masking Device Tinnitus Instrument Tinnitus Retraining Therapy Psychological Treatment Medication Alternative Treatments

59
Alternative Therapies Vitamins B1, B3, B6, B12, zinc, calcium, Mg Laser Therapy Germany Thought to increase ATP in cochlea

60
Alternative Therapies Hypnotherapy Acupuncture Ear canal magnets

61
Transcranial Magnetic Stimulation Brain stimulation ▫Identify active areas with PET ▫Apply magnetic stimulation (rTMS) ▫Evidence in small trials that there is some effect on tinnitus ▫More detailed research awaited Questions ▫Can this be clinically useful or is it just an experimental technique? ▫Long term safety?

62
Conclusion Tinnitus is a common condition Main role of ENT Surgeon is to exclude major illness and co-ordinate further treatment Basic advice and counseling as well as empathic support is paramount More severe cases may require psychological support, masking devices or Tinnitus Retraining Therapy

63
Thank you for Your Attention

Similar presentations


















 ST1.>")


