Download presentation
Presentation is loading. Please wait.

1
ASSOCIATE PROFESSOR Blidaru Iolanda-Elena, MD, PhD.

2
♣ a high-risk pregnancy early and excessive distension of the uterus inappropriate uterine contractility sharing the intracavitary space and placental nutrition IUGR abnormal fetal presentation placenta praevia velamentous insertion of the cord prematurity, HTA, caesarian section

3
Incidence multiple gestations → 12% of total conceptions 14% of these survive to term THE “VANISHING TWIN” - before the 2-nd trimester (20-60%) no evidence no risk
 no evidence no risk")
4
Clasification Monozygotic = identical twins a single fertilized ovum - a single fertilized ovum Dizygotic = fraternal twins Dizygotic = fraternal twins two separate ova - two separate ova - variable rate - 1.3 (Japan) - 49.0 (Nigeria)/ 1000 births - variable rate - 1.3 (Japan) - 49.0 (Nigeria)/ 1000 births - Recessive autosomal trait (female line) - Recessive autosomal trait (female line)
 (Nigeria)/ 1000 births - variable rate (Japan) (Nigeria)/ 1000 births - Recessive autosomal trait (female line) - Recessive autosomal trait (female line)")
6
Frequency of twins a- Monozygotic : 1:250 (independent) a- Monozygotic : 1:250 (independent) b- Dizygotic : 1:90 caucasians USA b- Dizygotic : 1:90 caucasians USA 1:20 Africans 1:20 Africans Depend on race, heredity, age of mother, parity, fertility drugs, post- OC use moment. Depend on race, heredity, age of mother, parity, fertility drugs, post- OC use moment.

7
Etiology – FSH LEVELS 1. Race - high in blacks, less in Asians 2. Heredity - mother more important than father 3. Age - peak incidence → 30-40 years 4. Parity 5. Drugs - inductors of ovulation 6. Assisted Reproductive Techniques (ART) 7. Season - frequent in summer
 7. Season - frequent in summer.")
8
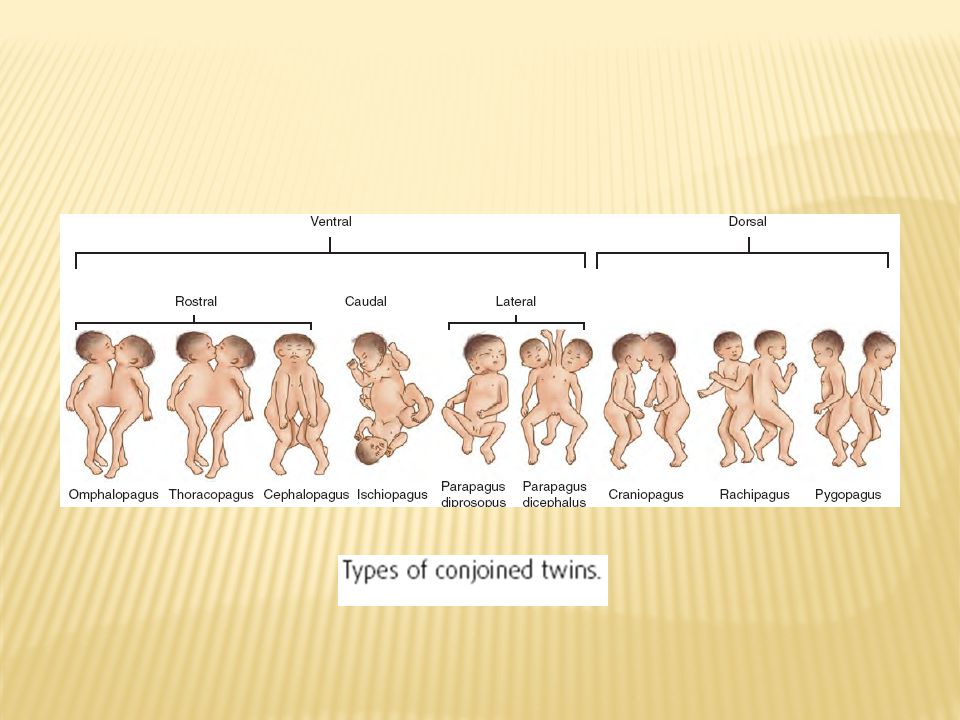
DIVISION First 72 hours two embryos, diamniotic, dichorionic. 4-8 days two embryos, diamniotic, monochorionic. About 8 - 14 days two embryos, monoamniotic, monochorionic. After 14 days cleavage is incomplete, conjoined twins.

9
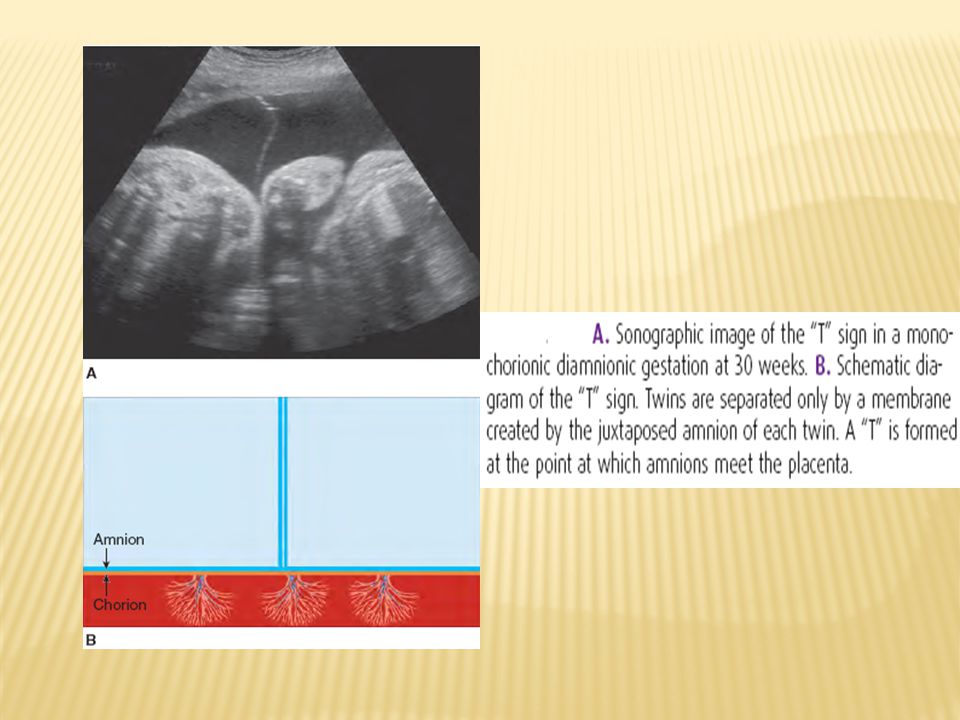
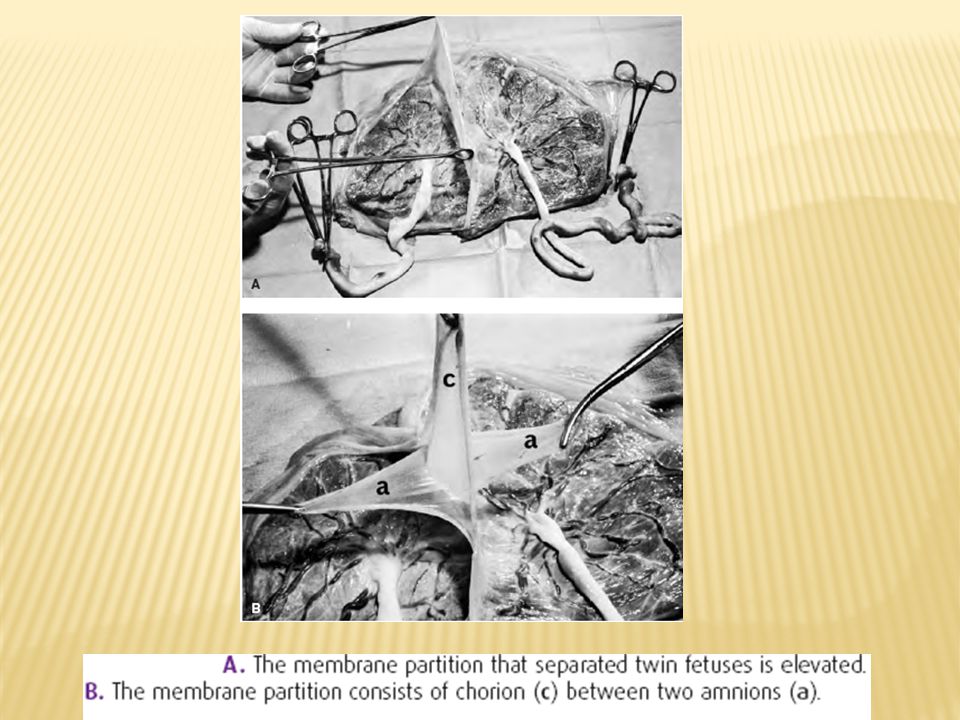
Determination of ZYGOSITY and CHORIONICITY US evaluation of chorionicity “twin peak” sign, ”T” sign fetal gender placental examination

12
Dichorionic diamniotic dizygotic or monozygotic dizygotic or monozygotic Monochorionic diamniotic monozygotic monozygotic Monochorionic monoamniotic monozygotic monozygotic

14
Monozygotic 30% single egg; an unique placenta, with vascular anastomoses; unique or double amniotic sacs; phenotypic and genotypic identity; twin-twin transfusion syndrome (TTTS); hydramnios; malformations. Dizygotic 70% eggs distinctly separated (dichorionic-diamniotic); absence of vascular anastomoses; normal volume of amniotic fluid; fetuses without phenotypic or genotypic identity; same or different sex.
; absence of vascular anastomoses; normal volume of amniotic fluid; fetuses without phenotypic or genotypic identity; same or different sex..")
16
Conjoined twins or Siamese twins

18
Vascular anastomoses between fetuses ♣ only in monochorionic twins (≈100%). ♣ 3 variants of vascular relationships: hemodynamic balance ; marked asymmetry (15 to 30%); the perfused fetus presents hypervolemia, heart failure, acute polyhydramnios, hyperbilirubinemia, hepatosplenomegaly; the hypo-perfused fetus has hypoxemia and oligohydramnios (twin-twin transfusion syndrome); slight asymmetry - slow transfusion (the tranfused fetus has higher weight and mild polycytemia.
; the perfused fetus presents hypervolemia, heart failure, acute polyhydramnios, hyperbilirubinemia, hepatosplenomegaly; the hypo-perfused fetus has hypoxemia and oligohydramnios (twin-twin transfusion syndrome); slight asymmetry - slow transfusion (the tranfused fetus has higher weight and mild polycytemia..")
19
TWIN TO TWIN TRANSFUSION SYNDROME (TTTS) Due to the common placental circulation and the anastomosis of the 2 fetal circulations FETUS PAPYRACEOUS One will regress in size, with oligohydramnios in its sac (if 2 sacs), may perish; then becomes dehydrated and mummified.
 Due to the common placental circulation and the anastomosis of the 2 fetal circulations FETUS PAPYRACEOUS One will regress in size, with oligohydramnios in its sac (if 2 sacs), may perish; then becomes dehydrated and mummified.")
21
PLACENTAL ANASTOMOSES

23
FETUS PAPYRACEOUS IN TRANSFUSION SYNDROME

24
TWIN TO TWIN TRANSFUSION SYNDROME

25
CLINICAL DIAGNOSIS 1. History. 2. Clinical Examination. 3. Investigations.

26
HISTORY Family history (maternal side) History of ovulation induction High parity Advanced maternal age Greater weight gain than expected Abdominal size >duration of amenorrhea Pressure symptoms (dyspnea, dyspepsia) Marked edema of lower limb.
 History of ovulation induction High parity Advanced maternal age Greater weight gain than expected Abdominal size >duration of amenorrhea Pressure symptoms (dyspnea, dyspepsia) Marked edema of lower limb.")
27
CLINICAL EXAMINATION ● Uterine size - larger than expected for GA + 5 cm (II trim.) ●Palor, early edema, varicose veins ●Glossy skin, striae, evident colateral circulation. ●Uterine palpation → two fetal heads or multiple similar fetal parts. ●Auscultation of FHS: 2 different sites and different frequency

28
CLINICAL EXAMINATION Bimanual examination a fetal pole, smaller than expected (related to uterine size) sometimes, in hypogastrum the fetal poles can't be detected uterine cervix may be effaced the membranes are under tension.
 sometimes, in hypogastrum the fetal poles can t be detected uterine cervix may be effaced the membranes are under tension.")
30
Ultrasound examination → the number of fetuses → type of placentation → fetal size and possible anomalies → presentation, position and relation to each other → fetal well-being and growth pattern for each → guidance to perform some maneuvers: amniocentesis, villous sampling

31
INVESTIGATIONS Biochemical tests 1. hCG in plasma and in urine 2. AFP level (alone is not diagnostic) 3. estriol 4. HPL
 3. estriol 4. HPL.")
32
Differential diagnosis 1. Hydramnios. 2. Hydatidiform mole. 3. Uterine myomas / ovarian cyst. 4. Fetal macrosomia ( single pregnancy ) 5. Elevation of the uterus by distended bladder.
 5. Elevation of the uterus by distended bladder..")
33
Maternal responses Cardiac output Plasma volume by 1/3 > singletons Red cell mass 300 ml > singletons Pre-eclampsia 5-10 times more Postpartum depression ↓ Hematocrit and hemoglobin ↓ Renal blood flow ↓ Iron stores

34
Fetal complications Spontaneous early pregnancy loss rate Discordant twins Twin to twin transfusion syndrome (TTTS) Intertwining of umbilical cords (monoamniotic twins) Conjoined twins Twin-reversed arterial perfusion sequence (TRAP) = acardiac twin Intrauterine growth restriction (IUGR) Preterm labour Cerebral palsy > 3 times > in twins 10 times > in triplets 10 times > in triplets
 Intertwining of umbilical cords (monoamniotic twins) Conjoined twins Twin-reversed arterial perfusion sequence (TRAP) = acardiac twin Intrauterine growth restriction (IUGR) Preterm labour Cerebral palsy > 3 times > in twins 10 times > in triplets 10 times > in triplets")
35
Acardiac twin weighing 475 grams. The underdeveloped head is indicated by the black arrow. Its viable donor co-twin was delivered vaginally at 36 weeks and weighed 2325 grams.

36
The perinatal mortality The principal causes of fetal death - prematurity, - IUGR - prolapsed cord, - infection, - hypoxia during delivery, - malformations, - transfusion syndrome.

37
Preterm birth: a- The most common complication of multiple pregnancies affecting long term outcome. b- prophylactic use Tocolytics Bed rest Cerclage

38
MANAGEMENT 1. ANTENATAL 2. IN LABOR 2. IN LABOR

39
(US) Early diagnosis (US) 1- Caloric consumption increased by 300 Kcal per day. 2- Iron 60-100 mg per day. 3- Folic acid 1mg per day. Adequate nutrition: 1- Caloric consumption increased by 300 Kcal per day. 2- Iron 60-100 mg per day. 3- Folic acid 1mg per day. - observe maternal and fetal complications 1- Frequent ultra sound fetal growth, congenital anomalies, amniotic fluid. 2- Doppler. Frequent prenatal visits - observe maternal and fetal complications 1- Frequent ultra sound fetal growth, congenital anomalies, amniotic fluid. 2- Doppler.

40
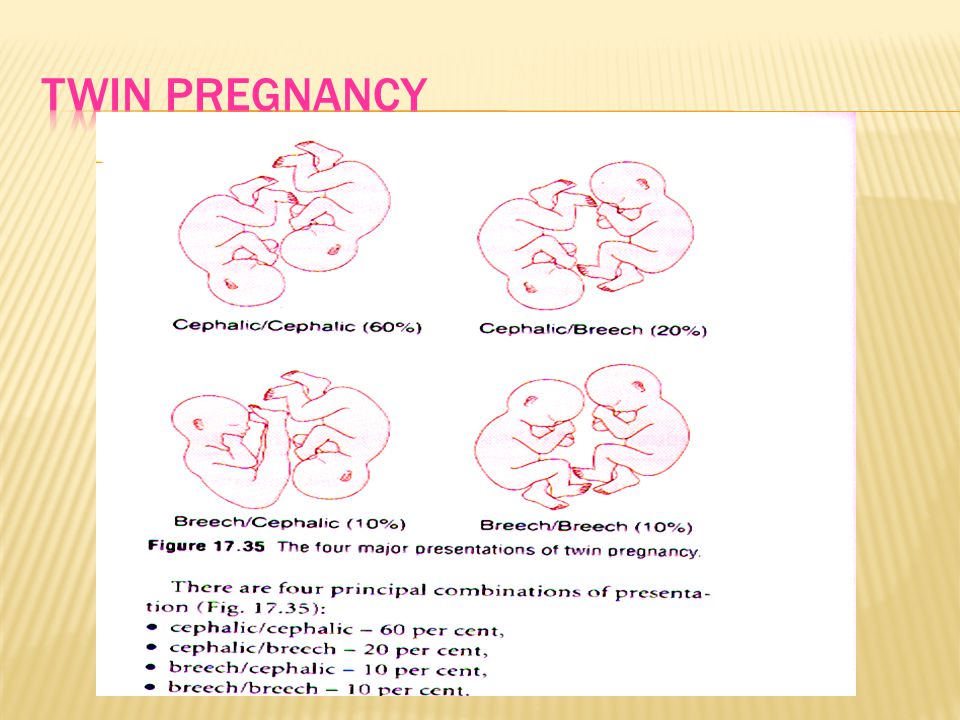
IN LABOR MANAGEMENT Trained obstetrical attendant. Available blood. Good access I.V line. Cardiotocography monitoring. Anesthetist. Pediatrician for each fetus. Mode of delivery - presentation of the first baby.

42
IN LABOR MANAGEMENT 40% of 0 P and 60% of parous women present in labor with a cervix dilated more than 3 cm. The latent phase is shorter. The active phase is longer. Uterine overdistension ▬ hypotonic uterine dysfunction. Increased risk of postpartum hemorrhage (uterine atony).
..")
43
Indications for cesarian section first twin presentation other than vertex hypotonic uterine dysfunction fetal distress prolapsed umbilical cord prematurity placenta praevia hypertension induced or aggravated by pregnancy.

44
The interval between delivery of the first and second twin is commonly cited to be safest if less than 30 minutes. Internal podalic version – for 2-nd twin If separation of the placenta is delayed or bleeding is brisk, extract the placenta manually after the final delivery. Postpartum hemorrhage is common. Hypotony should be treated promptly with oxytocin by rapid intravenous infusion and massage of the fundus.

Similar presentations









 MULTIPLE PARITY -Twins (two babies) -Monozygotic(Division of 1 ova fertilized.>")




 MULTIPLE PARITY -Twins (two babies) -Monozygotic(Division of 1 ova fertilized by the same sperm) -Dizygotic(Fertilization.>")










