Download presentation
Presentation is loading. Please wait.

1
CLINICAL APPROACH TO PERIPHERAL NEUROPATHY
Prof Dr.B.P.Shelley Department of Neurology Yenepoya Medical College

2
“Pattern recognition algorithm”
A stepwise approach “Pattern recognition algorithm”

3
Peripheral Neuropathies
Diagnostic conundrum: Diagnostic challenge, large number of potential causes, literally thousands of possible causes; is potentially frustrating, time consuming and costly Despite best efforts, it is important to appreciate that a good percentage (~20%) of neuropathies will remain undiagnosed despite an exhaustive evaluation 1/3-genetic; 1/3-acquired; 1/3- idiopathic despite appropriate diagnostic evaluation “Pragmatists vs. Completists”: Need to set the direction and level of aggressiveness of the evaluation, should not have an umbrella “one size fits all” blanket strategy of evaluation to an all encompasive ‘excludogram’ approach i.e. an unnecessarily expensive “shotgun” approach
 of neuropathies will remain undiagnosed despite an exhaustive evaluation. 1/3-genetic; 1/3-acquired; 1/3- idiopathic despite appropriate diagnostic evaluation. Pragmatists vs. Completists : Need to set the direction and level of aggressiveness of the evaluation, should not have an umbrella one size fits all blanket strategy of evaluation to an all encompasive ‘excludogram’ approach i.e. an unnecessarily expensive shotgun approach.")
10
FIVE QUESTION APPROACH
1. Fiber type 2. Pattern of distribution 5. Pathology 3. Temporal course 4. Key features

11
1.What is the fiber type involved?
(motor, large sensory, small sensory, autonomic, combination) 2. What is the pattern of distribution? (distal or proximal, symmetric or asymmetric) 3. What is the temporal course? (acute, chronic, progressive, stepwise, relapsing remitting) 4. Are there any key features pointing to a specific etiology? (toxic/nutritional/malignancy) 5. What is the pathology? (axonal, demyelinating)
 2. What is the pattern of distribution (distal or proximal, symmetric or asymmetric) 3. What is the temporal course (acute, chronic, progressive, stepwise, relapsing remitting) 4. Are there any key features pointing to a specific etiology (toxic/nutritional/malignancy) 5. What is the pathology (axonal, demyelinating)")
12
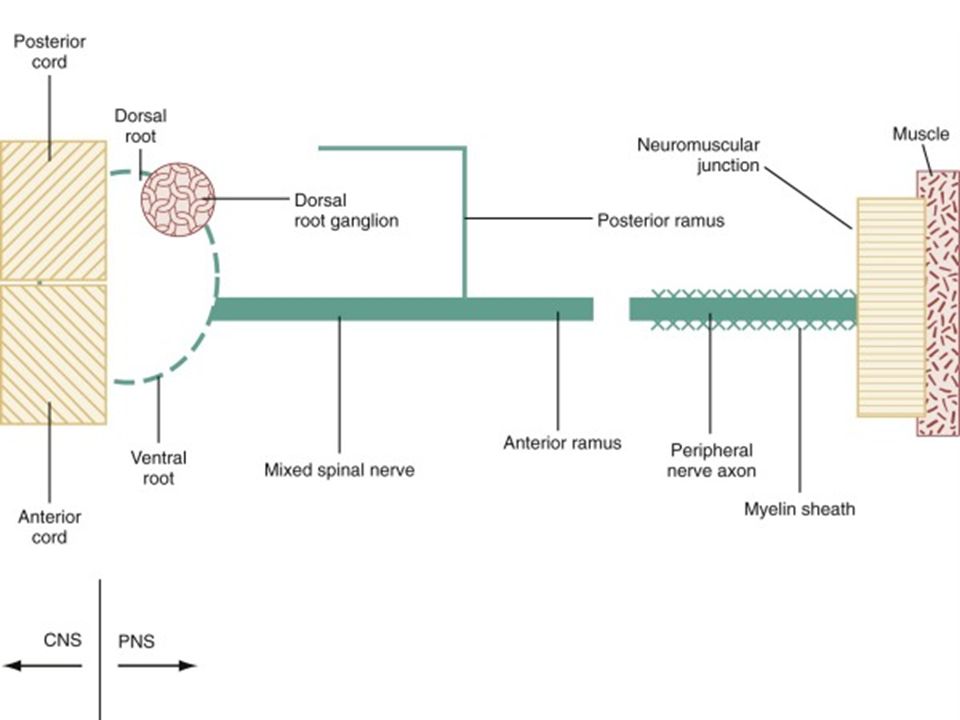
Pathological Process (1) Wallerian degeneration, which is the response to axonal interruption; (2) Axonal degeneration or axonopathy; (3) Primary neuronal degeneration or neuronopathy; (4) Segmental demyelination
 Primary neuronal degeneration or neuronopathy; (4) Segmental demyelination.")
13
Axonal degeneration Most common pathological reaction of peripheral nerve Caused by :Systemic metabolic disorders, toxin exposure, and some inherited neuropathies Also called dying-back or length-dependent neuropathy: The myelin sheath breaks down along with the axon in a process that starts at the most distal part of the nerve fiber and progresses toward the nerve cell body.

15
Role of nerve fibres in peripheralneuropathy

16
Dying-back neuropathy
Clinically, presents with symmetrical, distal loss of sensory and motor function in the lower extremities that extends proximally in a graded manner. The result is sensory loss in a stocking-like pattern, distal muscle weakness and atrophy, and loss of ankle reflexes

17
Neuronopathy Dorsal root ganglionopathy (inflammatory; drugnon neoplastic-NISP; Malignant sensory inflmmaory ganglionopathy-MISG) Primary loss or destruction of nerve cell bodies with resultant degeneration of their entire peripheral and central axons. Either lower motor neurons (AHC, motor axonopathy) or dorsal root ganglion cells may be affected. When anterior horn cells - poliomyelitis or motor neuron disease: focal weakness without sensory loss Sensory neuronopathy, or polyganglionopathy :damage to dorsal root ganglion neurons - inability to localize the limb in space, diffuse areflexia, and early gait/limb sensory ataxia; pain, paresthesia, numbness, cramps, fatigue, abnormal hot/cold sensations, nocturnal pains in UL/LLs, severe loss of JPS/vibration sense
 or dorsal root ganglion cells may be affected. When anterior horn cells - poliomyelitis or motor neuron disease: focal weakness without sensory loss. Sensory neuronopathy, or polyganglionopathy :damage to dorsal root ganglion neurons - inability to localize the limb in space, diffuse areflexia, and early gait/limb sensory ataxia; pain, paresthesia, numbness, cramps, fatigue, abnormal hot/cold sensations, nocturnal pains in UL/LLs, severe loss of JPS/vibration sense.")
18
Segmental demyelination
The term implies injury of either myelin sheaths or Schwann cells, resulting in breakdown of myelin with sparing of axons This occurs in immune-mediated demyelinating neuropathies and in hereditary disorders of Schwann cell/myelin metabolism.

19
Demyelinating neuropathies
Relative sparing of temperature and pinprick sensation + 1.Early generalized loss of reflexes (large fiber, predominantly motor neuropathy; immune mediated; acute-subacute) 2.Disproportionately mild muscle atrophy but DTRs affected 3.Presence of proximal and distal weakness (P>D/P=D; universal DTRs involvement) 4.Neuropathic tremor (Anti MAG-IgM paraproteinemic neuropathy- CIDP like) 5. Palpably enlarged nerves 6. CSF Albuminocytologic dissociation 7. ElectroDx changes: slowed NCV, CBs, TD (acquired demyelination, segmental demyelination; not uniform demyelination as in genetic determined CMT IA)
 2.Disproportionately mild muscle atrophy but DTRs affected. 3.Presence of proximal and distal weakness (P>D/P=D; universal DTRs involvement) 4.Neuropathic tremor (Anti MAG-IgM paraproteinemic neuropathy- CIDP like) 5. Palpably enlarged nerves. 6. CSF Albuminocytologic dissociation. 7. ElectroDx changes: slowed NCV, CBs, TD (acquired demyelination, segmental demyelination; not uniform demyelination as in genetic determined CMT IA)")
20
Diagnostic Clues from the History
1.Motor 2.Sensory 3.Autonomic disturbances Seek both positive and negative symptoms A. Motor: Positive : Muscle cramps, fasciculations, myokymia, or tremor Negative : early distal toe and ankle extensor weakness, resulting in tripping on rugs or uneven ground

21
Sensory symptoms Positive :
prickling, searing, burning, and tight bandlike sensations. Paresthesia: Unpleasant sensations arising spontaneously without apparent stimulus Allodynia: perception of nonpainful stimuli as painful. Hyperalgesia: Painful hypersensitivity to noxious stimuli Neuropathic pain: cardinal feature of many neuropathies.

22
Autonomic dysfunction
Positive or Negative symptoms Orthostatic lightheadedness Fainting spells Sweating reduced or excessive Heat intolerance Bladder, Bowel, and Sexual dysfunction Anorexia, early satiety, nausea, and vomiting Adie’s pupil Cardiovascular dysautonomia

23
TEMPORAL CLUES Onset, duration, and evolution of symptoms
Tempo of disease : acute, subacute, or chronic Course: monophasic, progressive, or relapsing Acute presentations: Guillain-Barré syndrome (GBS), acute porphyria, vasculitis, toxic neuropathies. Relapsing course : (CIDP), acute porphyria, Refsum's disease, hereditary neuropathy with liability to pressure palsies (HNPP), familial brachial plexus neuropathy, and repeated episodes of toxin exposure.
, acute porphyria, vasculitis, toxic neuropathies. Relapsing course : (CIDP), acute porphyria, Refsum s disease, hereditary neuropathy with liability to pressure palsies (HNPP), familial brachial plexus neuropathy, and repeated episodes of toxin exposure.")
24
Constitutional symptoms
Weight loss, malaise, and anorexia. DM hypothyroidism chronic renal failure liver disease intestinal malabsorption malignancy connective tissue diseases [HIV] drug use Vitamin B6 toxicity alcohol and dietary habits exposure to solvents, pesticides, or heavy metals.

25
Mononeuropathy Focal involvement of a single nerve and implies a local process: Direct trauma compression or entrapment vascular lesions neoplastic compression or infiltration

26
Mononeuropathy multiplex
simultaneous /sequential damage to multiple noncontiguous nerves. Ischemia caused by vasculitis Microangiopathy in diabetes mellitus Less common causes : Infectious, granulomatous, leukemic, or neoplastic infiltration, Hansen's disease (leprosy) and sarcoidosis.
 and sarcoidosis.")
27
Polyneuropathy Characterized by symmetrical, distal motor and sensory deficits that have a graded increase in severity distally and by distal attenuation of reflexes, Rarely predominantly proximal:(E.g: acute intermittent porphyria). The sensory deficits generally follow a length-dependent stocking- glove pattern
. The sensory deficits generally follow a length-dependent stocking- glove pattern.")
28
Motor deficits Dominate the clinical picture in 1. AIDP/CIDP
2. Hereditary motor and sensory neuropathies, 3. Neuropathies associated with osteosclerotic myeloma, porphyria, lead and organophosphate intoxications, and hypoglycemia.

29
Pattern of weakness Asymmetrical motor weakness without sensory loss suggests motor neuron disease or multifocal motor neuropathy with conduction block

30
Neuropathies with Facial Nerve Involvement
Guillain-Barré syndrome Chronic inflammatory polyradiculoneuropathy Lyme disease Sarcoidosis HIV

31
Predominant Sensory Celiac disease
Toxicity with cisplatin, thalidomide, or pyridoxine Inherited and idiopathic sensory neuropathies Diabetes Carcinoma; Sjögren's syndrome; Dysproteinemia; AIDS vitamin B12 deficiency

32
Autonomic dysfunction
GBS Diabetes Amyloid sensorimotor polyneuropathy

33
Small-Fiber Neuropathies
Idiopathic small fiber neuropathy Diabetes mellitus Amyloid neuropathy HIV-associated distal sensory neuropathy Hereditary sensory and autonomic neuropathies

34
Large-fiber Areflexia Pseudoathetosis
Loss of joint position and vibration sense Positive Romberg's sign

35
Algorithm Does the history and examination suggest that the pathological process is localized to the peripheral nerve? Masqueraders-parietal lesion, cervical spondylotic myelopathy, transverse myelitis; certain neuropathies co-exist with CNS disease (myeloneuropathies-vitamin B12 deficiency, adrenomyeloneuropathy) Has the presenting complaint been fully described? a thorough & meticulous history taking Have I obtained adequate past, family, occupational, and drug histories? What special features of diagnostic help might I pick up from the examination? (Pink urine-porphyria, umbilical angiokeratomas of Fabry’s disease, Mees line of Arsenic toxicity, orange tonsils of Tangier’s disease, ansomia in Refsum’s diase, Optic atrophy, Adie’s pupil for dysautonomia)
 Has the presenting complaint been fully described a thorough & meticulous history taking. Have I obtained adequate past, family, occupational, and drug histories What special features of diagnostic help might I pick up from the examination (Pink urine-porphyria, umbilical angiokeratomas of Fabry’s disease, Mees line of Arsenic toxicity, orange tonsils of Tangier’s disease, ansomia in Refsum’s diase, Optic atrophy, Adie’s pupil for dysautonomia)")
36
Algorithm Is the neuropathy focal, multifocal or generalized?
What is the relative extent of motor and sensory nerve involvement? Is there prominent small fibre and autonomic involvement? Is the neuropathy axonal or demyelinating on clinical grounds? (demyelinating- widespread DTR loss, proximal & distal in muscle groups that are not particularly weak or wasted, more proximal weakness/ axonal- selective distal/ankle DTRS absent in the presence of distal wasting and weakness, stocking distribution of sensory loss) What additional information can I expect from a neurophysiologic assessment? What screening tests should I perform? When should I do a nerve biopsy?
 What additional information can I expect from a neurophysiologic assessment What screening tests should I perform When should I do a nerve biopsy")
37
Stepwise approach Within the peripheral nervous system? Exclude CNS, spinal causes (UMN cause) What part of the peripheral nervous system? Root, plexus, single nerve, multiple nerves, peripheral neuropathy, radiculoplexopathy, myeloneuropathy; proximal (AIDP, CIDP, Porphyria, DRPN) or distal neuropathiy; cranial or trunkal neuropthy What is the time course? Acute, subacute, chronic, progressive, relapsing-remitting, event-linked What nerve fibers are involved? Sensory, motor, autonomic, combinations What is the primary pathology? Demyelination, axonal, mixed What are the other pertinent features? Family, medical, social histories, genetic history
 or distal neuropathiy; cranial or trunkal neuropthy. What is the time course Acute, subacute, chronic, progressive, relapsing-remitting, event-linked. What nerve fibers are involved Sensory, motor, autonomic, combinations. What is the primary pathology Demyelination, axonal, mixed. What are the other pertinent features Family, medical, social histories, genetic history.")
38
An easy approach to peripheral neuropathy

39
“WHAT. ”, “WHERE. ”, “WHEN. ” and “WHAT SETTING
“WHAT?”, “WHERE?”, “WHEN?” and “WHAT SETTING?” ‘user friendly approach’ What: Nerve fiber type- Sensory (S), motor (M), or autonomic (A) (small fiber vs. large fiber; positive vs. negative symptoms; demyelinating vs. axonal (Myelinopathy, Axonopathy, Neuronopathy); Painful vs. painless) SM, Pure M, Pure S, M>S, S>M, pure autonomic; helpful to rank them in order of symptom predominance- predominantly motor-immune mediated neuropathies/ sensory predominant-small fiber, length dependant, dying back (axonal-Wallerian degeneration) neuropathies related to toxic, metabolic, nutritional, or ischemic-vasculitic etiologies. Ranking them by predominance can help direct evaluation of neuropathies (Harrison’s tabular column)
, motor (M), or autonomic (A) (small fiber vs. large fiber; positive vs. negative symptoms; demyelinating vs. axonal (Myelinopathy, Axonopathy, Neuronopathy); Painful vs. painless) SM, Pure M, Pure S, M>S, S>M, pure autonomic; helpful to rank them in order of symptom predominance- predominantly motor-immune mediated neuropathies/ sensory predominant-small fiber, length dependant, dying back (axonal-Wallerian degeneration) neuropathies related to toxic, metabolic, nutritional, or ischemic-vasculitic etiologies. Ranking them by predominance can help direct evaluation of neuropathies (Harrison’s tabular column)")
40
Autonomic-Diabetes, Amyloid, GBS, Sjogren’s related neuropathies, Paraneoplastic, HSAN) Sensory neuropathic symptom profile: Patients with acquired polyneuropathies usually complain of positive neuropathic sensory symptoms (PNSS), whereas patients with inherited polyneuropathies only rarely do. Painful neuropathies (allodynia, hyperalgesia) suggest toxic, metabolic, or ischemic/vasculitic causes of neuropathy involving small fibers (small fiber neuropathy). Pure sensory neuropathies or neuronopathies can result from drug toxicity (e.g., thalidomide, cisplatin, paraneoplastic syndromes or nutritional deficiencies-thiamine; uremia. Predominantly motor neuropathies: AIDP, CIDP, MMN, Prophyria, Diptheria, SLE/PAN, TOCP, Lead. Small fiber sensory neuropathies: DM, Hansen’s, Thiamine, Uremia, Amyloid, Paraneoplastic, HSN. Small fiber autonomic neuropathies: Diabetes, amyloid, Fabry’s disease, Tangier’s, Sjogrens, HSAN) Fiber Types: Myelinated Aα, Aβ (motor); Thinly myelinated Aδ/C (sensory); Unmyelinated (Type C); Pseudo-syringomyelic neuropathy
; Thinly myelinated Aδ/C (sensory); Unmyelinated (Type C); Pseudo-syringomyelic neuropathy.")
41
Where: The distribution of nerve involvement: symmetrical/asymmetrical/multifocal Proximal or length dependant distal; mono, multiple mononeuritis, polyneuropathies; plexopathy; neuronopathy; radiculoplexopathy; radiculoneuropathy; myeloneuropathy); cranial/trunkal neuropathies Motor neuronopathies (eg, amyotrophic lateral sclerosis), Sensory neuronopathies (eg, paraneoplastic), polyradiculoneuropathies (Guillain-Barré syndrome, CIDP), and mononeuritis multiplex (caused by vasculitis), Diabetic radiculoplexopathy, Hepatic/Nutritional-Cassava-Konzo-Tropical Myeloneuropathies (TSP). Multifocal: Vasculitis, Amyloid, Diabetes, MMN, HNPP
; cranial/trunkal neuropathies. Motor neuronopathies (eg, amyotrophic lateral sclerosis), Sensory neuronopathies (eg, paraneoplastic), polyradiculoneuropathies (Guillain-Barré syndrome, CIDP), and mononeuritis multiplex (caused by vasculitis), Diabetic radiculoplexopathy, Hepatic/Nutritional-Cassava-Konzo-Tropical Myeloneuropathies (TSP). Multifocal: Vasculitis, Amyloid, Diabetes, MMN, HNPP.")
42
When? , What setting? When (disease course): The time course of signs and symptoms: acute, subacute, chronic, recurrent & relapsing; Acute/subacute onset often suggests an immune-mediated or infectious process. What setting (Etiological): Hereditary-inheritance pattern; familial/ Acquired-MINI- Metabolic, Immune, Neoplastic, Infectious: medical history, medications, social and family history, review of systems (Hereditary/genetic; Acquired- infectious, toxic, metabolic, drugs, endocrine, paraneoplastic, immune mediated, infiltrative, inflammatory-vasculitic); with neurocutaneous markers; hammer toes; claw feet; pes cavus; “champagne bottle” legs, trophic painless ulcers-valuable clues for genetical neuropathies; malignancy; bariatric surgeries-Vit B1 B12 deficiencies; gastrectomy related ‘SCD like picture’ with normal Vit B12-copper myeloneuropathy
: The time course of signs and symptoms: acute, subacute, chronic, recurrent & relapsing; Acute/subacute onset often suggests an immune-mediated or infectious process. What setting (Etiological): Hereditary-inheritance pattern; familial/ Acquired-MINI- Metabolic, Immune, Neoplastic, Infectious: medical history, medications, social and family history, review of systems (Hereditary/genetic; Acquired- infectious, toxic, metabolic, drugs, endocrine, paraneoplastic, immune mediated, infiltrative, inflammatory-vasculitic); with neurocutaneous markers; hammer toes; claw feet; pes cavus; champagne bottle legs, trophic painless ulcers-valuable clues for genetical neuropathies; malignancy; bariatric surgeries-Vit B1 B12 deficiencies; gastrectomy related ‘SCD like picture’ with normal Vit B12-copper myeloneuropathy.")
43
Pearls for classification of peripheral neuropathies A suggested construct for the approach to neuropathy, using the “what, where, when, and what setting” approach to characterizing the neuropathy and placing the neuropathy into a presumed etiologic ... Figure Pearls for classification of peripheral neuropathies A suggested construct for the approach to neuropathy, using the “what, where, when, and what setting” approach to characterizing the neuropathy and placing the neuropathy into a presumed etiologic category. PNSS = positive neuropathic sensory symptoms; CMT = Charcot-Marie-Tooth; HMSN = hereditary motor and sensory neuropathies; HNPP = hereditary neuropathy with liability to pressure palsy; GBS = Guillain-Barré syndrome; CIDP = chronic inflammatory demyelinating polyradiculoneuropathy; MMN = multifocal motor neuropathy; PAN = polyarteritis nodosa; SLE = systemic lupus erythematosus; RA = rheumatoid arthritis. Modified and reprinted with permission from Mauermann ML, Burns TM. The evaluation of acquired neuropathies. Semin Neurol 2008;28:133–151.6 Mauermann M, Burns T. Neurology 2009;72:e28-e31 ©2009 by Lippincott Williams & Wilkins

44
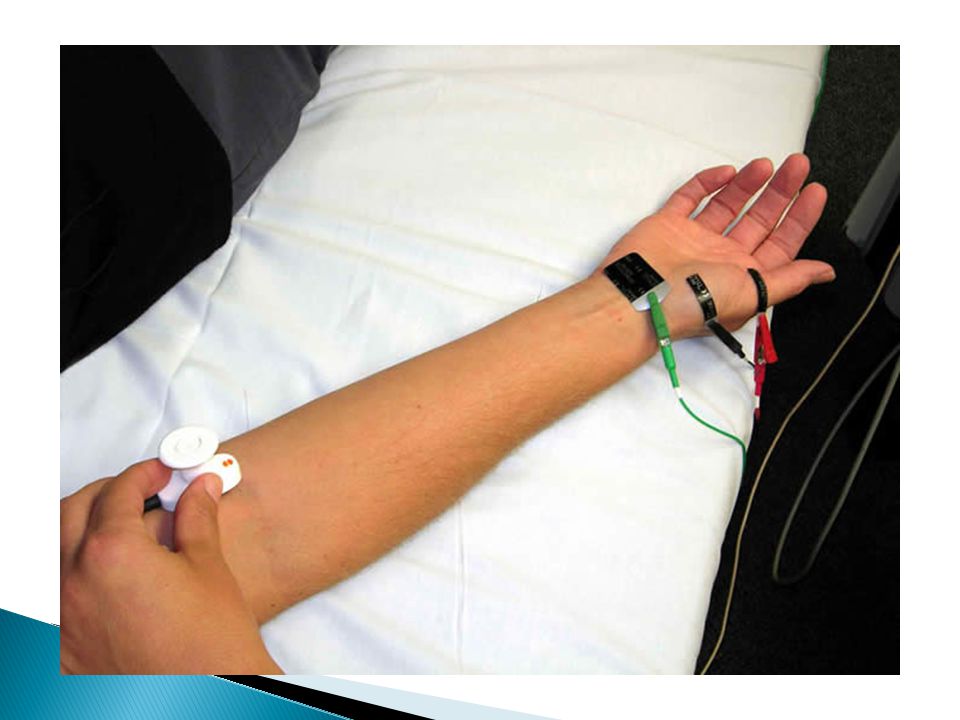
Electrodiagnosis ElectroDx: Electrodiagnostic testing assists in characterizing the neuropathic process as sensory, motor or sensorimotor (What?). Electrodiagnostic testing helps characterize a neuropathy as primarily demyelinating, primarily axonal, or mixed demyelinating and axonal; help localize the neuropathic process (the “where”-symmetrical, asymmetrical, proximal, distal, localization to roots, plexus, nerve, radiculoplexopathy, radiculoneuropathy); help gauge the severity of neuropathy; help assess treatment response
. Electrodiagnostic testing helps characterize a neuropathy as primarily demyelinating, primarily axonal, or mixed demyelinating and axonal; help localize the neuropathic process (the where -symmetrical, asymmetrical, proximal, distal, localization to roots, plexus, nerve, radiculoplexopathy, radiculoneuropathy); help gauge the severity of neuropathy; help assess treatment response.")
45
Algorithm showing a stepwise approach to the assessment and investigation of a possible neuropathy. CIDP, chronic inflammatory demyelinating polyradiculoneuropathy; CMT, Charcot-Marie-Tooth; EMG, electromyography; GBS, Guillain-Barre syndrome; HNPP, hereditary neuropathy with liability to pressure palsies; NCS, nerve conduction studies. Willison, H. J et al. J Neurol Neurosurg Psychiatry 2003;74:3-8ii Copyright ©2003 BMJ Publishing Group Ltd.

46
(1) Confirming the presence of neuropathy,
(2) Locating focal nerve lesions, (3) Nature of the underlying nerve pathology
 Locating focal nerve lesions, (3) Nature of the underlying nerve pathology.")
48
Distal motor latency prolonged
Nerve conduction velocity slow Reduced action potential

49
Nerve biopsy In vasculitis, amyloid neuropathy, leprosy, CIDP, Inherited disorders of myelin, and rare axonopathies The Sural nerve is selected most commonly The superficial peroneal nerve – alternative; :advantage of allowing simultaneous biopsy of the peroneus brevis muscle through the same incision. This combined nerve and muscle biopsy procedure increases the yield of identifying suspected vasculitis

50
Neuropathies + Serum Autoantibodies
Antibodies against Gangliosides GM1 : Multifocal motor neuropathy GM1, GD1a : Guillain-Barré syndrome GQ1b : Miller Fisher variant Antibodies against Glycoproteins Myelin-associated glycoprotein : MGUS Antibodies against RNA-binding proteins Anti-Hu, antineuronal nuclear antibody 1: Malignant inflammatory polyganglionopathy

51
SUMMARY A. Clinical pattern of neurologic findings Polyneuropathy, Neuronopathy, Mononeuropathy, Multiple mononeuropathy, Plexopathies B. Functional disturbance: Motor, Sensory, Autonomic, Mixed C. Mode of onset : 1.Acute 2.Subacute 3.Chronic 4.Relapsing

52
D. Pathological and electrophysiological criteria:
1.Demyelinating disease vs Axonopathy 2.Wallerian degeneration - trauma 3.Dying back neuropathy - toxic, metabolic E. Etiology: Metabolic, immune mediated, toxic, vasculitis, dysproteinemic, inherited, Nutritional deficiency F. Diagnosis 1.Clinical data 2.Electrophysiologic test : NCS, EMG 3.Biochemical test : metabolic, nutritional, toxic Laboratory Tests: Serology, CSF, Blood sugar, Liver function tests, Vitamin B12, Paraprotein screen, Thyroid function, Full blood count, Erythrocyte sedimentation rate, vasculitic screen 4.CSF study 5. Nerve & muscle biopsy Nerve biopsy: helpful in very specific cases to diagnose vasculitis, leprosy, amyloid neuropathy, leukodystrophies, sarcoidosis and, occasionally, CIDP 6. Measurement of Ig & anti-neural antibody 7. Genetic study

53
History taking; Pertinent question (Pearls & Oysters)
Time frame/Onset: Acute (0-4 weeks), Sub acute (4-8 weeks), Chronic (> 8 weeks) Course: Monophasic; Multifocal; Progressive; Relapsing/Recurrent (CIDP/Refsum’s disease; porphyria; beri-beri; Tangier’s disease; Toxic: HIV) Distribution: Focal or Multifocal (MADSAM; HNPP; Vasculitic; Entrapment); Diffuse/Generalised; Symmetrical or Asymmetrical (mononeuritis multiplex-DM; vasculitic, PAN, SLE; Wegner’s; Churg- Strauss; cryogloulinemia; Sjogren’s; HNPP; HIV; lymphoma; carcinoma) Fiber Type: Type A alpha; Type A beta (myelinated); Type A delta (thinly myelinated); Type C (unmyelinated); Large fiber vs. Small fiber neuropathy Positive and Negative Symptoms Associated with Nerve Damage
, Sub acute (4-8 weeks), Chronic (> 8 weeks) Course: Monophasic; Multifocal; Progressive; Relapsing/Recurrent (CIDP/Refsum’s disease; porphyria; beri-beri; Tangier’s disease; Toxic: HIV) Distribution: Focal or Multifocal (MADSAM; HNPP; Vasculitic; Entrapment); Diffuse/Generalised; Symmetrical or Asymmetrical (mononeuritis multiplex-DM; vasculitic, PAN, SLE; Wegner’s; Churg- Strauss; cryogloulinemia; Sjogren’s; HNPP; HIV; lymphoma; carcinoma) Fiber Type: Type A alpha; Type A beta (myelinated); Type A delta (thinly myelinated); Type C (unmyelinated); Large fiber vs. Small fiber neuropathy. Positive and Negative Symptoms Associated with Nerve Damage.")
54
History taking; Pertinent question (Pearls & Oysters)
Clinical pattern: Motor, Sensory, SM, Autonomic; Cranial neuropathies Painful [Neuropathic pain] vs. Painless neuropathies/ Painful neuropathies are axonal secondary to toxic, metabolic, nutritional causes Recurrent/Relapsing neuropathies Mononeuropathy, Mononeuritis multiplex, Polyneuropathy, Autonomic, Myeloneuropathies, Radiculoneuropathies Polyneuropathy with clinical combinations/associations: skin changes; eye lesions; ear lesions; pyramidal deficits; ataxia; mental- cognitive-behavioural-neuropsychiatric disorders; orange tonsils; dwarfism; thickened Achilles tendon

55
History taking; Pertinent question (Pearls & Oysters)
Polyneuropathies with “the company it keeps” Skin: Refsum’s disease/Abetalipoproteinemia (icthyosis); xeroderma pigmentosum, Cockayne syndrome; Varigate porphyria (UV light hypersensitivity); Fabry’s disease (angiokeratoma corporis diffusum) Curly reddish hair: Giant axonal neuropathy (alopecia-Thallium neuropathy) Eye: Refsum’s disease; Cockayne syndrome; Abetalipoproteinemia; NARP (Retinitis pigmentosa); ALD (retinal degenartion); HMSN (Optic atrophy); Fabry’s disease, Tangier’s disease; Familial amyloid neuropathy Type 4 (corneal dystrophy); Refsum’s disease/abetalipoproteinemia (night blindness); Marinesco-Sjogren’s syndrome (cataract) Ear: Fabry’s disease Cardiac: Refsum’s disease, Refsum’s disease (ataxia; neuropathy; cardiomyopathy; phytanic acid elevated; cataract; SN deafness; icthyosis)
; xeroderma pigmentosum, Cockayne syndrome; Varigate porphyria (UV light hypersensitivity); Fabry’s disease (angiokeratoma corporis diffusum) Curly reddish hair: Giant axonal neuropathy (alopecia-Thallium neuropathy) Eye: Refsum’s disease; Cockayne syndrome; Abetalipoproteinemia; NARP (Retinitis pigmentosa); ALD (retinal degenartion); HMSN (Optic atrophy); Fabry’s disease, Tangier’s disease; Familial amyloid neuropathy Type 4 (corneal dystrophy); Refsum’s disease/abetalipoproteinemia (night blindness); Marinesco-Sjogren’s syndrome (cataract) Ear: Fabry’s disease. Cardiac: Refsum’s disease, Refsum’s disease (ataxia; neuropathy; cardiomyopathy; phytanic acid elevated; cataract; SN deafness; icthyosis)")
56
History taking; Pertinent question (Pearls & Oysters)
GI symptoms: Whipple’s disease; Malabsorption syndromes; Celiac disease; Arsenic neuropathy (abdominal pain, diarrhea, vomiting Adrenal insuffiency: ALD Pyramidal: Krabbe, Metachromatic leucodystrophy; HMSN type 5; SCD-anemia/Vit E/Copper myeloneuropathies; HSP; TSP; Tropical Myeloneuropathies Ataxia: Mitochondrial cytopathies; Ataxia telangiectasia; Abetalipoproteinemia (LDL C low); Refsum’s disease; Xeroderma pigmentosum; Cockayne syndrome, SCD, Friederich’s ataxia; Roussy Levy Disease Mental retardation: Leucodystrophy; Cockayne syndrome; ADL Neuropsychiatry: Porphyria Yellow Orange tonsils: Tangier’s disease (HDL C low) Short stature/Dwarfism: Cockayne syndrome; mitochondrial cytopathies Thickened TA tendon: Cerebrotendinous xanthomatosis
; Refsum’s disease; Xeroderma pigmentosum; Cockayne syndrome, SCD, Friederich’s ataxia; Roussy Levy Disease. Mental retardation: Leucodystrophy; Cockayne syndrome; ADL. Neuropsychiatry: Porphyria. Yellow Orange tonsils: Tangier’s disease (HDL C low) Short stature/Dwarfism: Cockayne syndrome; mitochondrial cytopathies. Thickened TA tendon: Cerebrotendinous xanthomatosis.")
57
History taking; Pertinent question (Pearls & Oysters)
Upper limb/Bibrachial neuropathies: Lead neuropathy, brachial neuritis, amyloid neuropathy type II, Porphyria, AIDP/GBS, MMNCB, ALS, Hirayama’s diasease, Bibrachial amyotrophic diplegia, HypoK paralysis Neuropathies with cranial nerve involvement:AIDP/GBS, CIDP, Hansen’s disease; Diabetes mellitus, HIV, Sarcoidosis, Diptheria Asymmetrical neuropathies:Mononeuritis multiplex, Vasculitic PAN, SLE, Wegeners’ granulomatosis, Cryoglobulinemia, Sjogren’s syndrome, HNPP, HIV, Lymphoma, Carcinoma

58
Evaluation of PN; Pearls & Oysters
Pathology: Fiber type: Small (Pseudosyringomyelic-Leprosy; DM; Tangier’s; Amyloid; Alcoholic ;) vs. Large fiber neuropathy (Positive & Negative symptoms); Burning feet syndrome/Gopalan syndrome-pantothenate deficiency; alcoholic; nutritional neuropathies; toxic-Arsenic/Thallium; HIV Small fiber: DTRs retained Positive: fasciculations; minipolymyoclonus; cramps; myokymia; neuromyotonia; dystonia; pseudoathetosis; tremors (CIDP/Anti MAG paraproteinemic neuropathy); paraesthesia; dysesthesia; allodynia; hyperpathia; hyperalgesia; restless leg syndrome/Ekbom’s syndrome; sensory ataxic neuropathies/ganglionopathies (pseudoathetosis-dancing fingers; pseudotabes-DM) Negative: Numbness; loss of temperature sensations Myelinopthy/Demeylination (segmental), Axonal-dying back neuropathy/Axonopathy, Mixed demyelinating-axonal; Neuronopathy (DRG/AHC) Demyelinating neuropathy: proximal > distal weakness; proximal DTRs affected; no atrophy; thickened nerves; CSF: AB cytologic dissociation; NCV changes & F latency Axonopathies: Distal weakness; distal areflexia; muscle atrophy; NCV changes; EMG DN pattern
 vs. Large fiber neuropathy (Positive & Negative symptoms); Burning feet syndrome/Gopalan syndrome-pantothenate deficiency; alcoholic; nutritional neuropathies; toxic-Arsenic/Thallium; HIV. Small fiber: DTRs retained. Positive: fasciculations; minipolymyoclonus; cramps; myokymia; neuromyotonia; dystonia; pseudoathetosis; tremors (CIDP/Anti MAG paraproteinemic neuropathy); paraesthesia; dysesthesia; allodynia; hyperpathia; hyperalgesia; restless leg syndrome/Ekbom’s syndrome; sensory ataxic neuropathies/ganglionopathies (pseudoathetosis-dancing fingers; pseudotabes-DM) Negative: Numbness; loss of temperature sensations. Myelinopthy/Demeylination (segmental), Axonal-dying back neuropathy/Axonopathy, Mixed demyelinating-axonal; Neuronopathy (DRG/AHC) Demyelinating neuropathy: proximal > distal weakness; proximal DTRs affected; no atrophy; thickened nerves; CSF: AB cytologic dissociation; NCV changes & F latency. Axonopathies: Distal weakness; distal areflexia; muscle atrophy; NCV changes; EMG DN pattern.")
59
Evaluation of PN; Pearls & Oysters
Etiological: MINI (Metabolic; Immune; Neoplastic/Nutritional; Infectious/Inherited) Hereditary/Genetic, Inflammatory, Infectious,Ischemic, Immunological, Nutritional, Metabolic, Toxic, Drug induced; Infiltrative, Paraneoplastic, Critical Illness; Idiopathic (30%) Topography: Proximal/Distal Neuropathies (length dependant neuropathies) [Proximal neuropathies: AIDP/SIDP/CIDP/Porphyric neuropathy; Diabetic plexoradiculopathy-Garland’s Diabetic amyotrophy] Genetic neuropathies: AR; AD; X-linked Mendelian inheritance (HMSN; HSAN) Enlarged peripheral nerves: Hansen’s disease; chronic recurrent/replacing neuropathies; CIDP; HMSN-CMT-1 (hypertrophic neuropathies); Neurofibromatosis; nerve tumors; Djerine Sottas neuropathy; Amyloid neuropathy [greater auricular-middle SSM; supraorbital; suprascapular; supraclavicular; cervical, ulnar; median (wrist); radial (radial groove); CPN; posterior tibial; superficial radial cutaneous-anatomical snuff box]
 Hereditary/Genetic, Inflammatory, Infectious,Ischemic, Immunological, Nutritional, Metabolic, Toxic, Drug induced; Infiltrative, Paraneoplastic, Critical Illness; Idiopathic (30%) Topography: Proximal/Distal Neuropathies (length dependant neuropathies) [Proximal neuropathies: AIDP/SIDP/CIDP/Porphyric neuropathy; Diabetic plexoradiculopathy-Garland’s Diabetic amyotrophy] Genetic neuropathies: AR; AD; X-linked Mendelian inheritance (HMSN; HSAN) Enlarged peripheral nerves: Hansen’s disease; chronic recurrent/replacing neuropathies; CIDP; HMSN-CMT-1 (hypertrophic neuropathies); Neurofibromatosis; nerve tumors; Djerine Sottas neuropathy; Amyloid neuropathy [greater auricular-middle SSM; supraorbital; suprascapular; supraclavicular; cervical, ulnar; median (wrist); radial (radial groove); CPN; posterior tibial; superficial radial cutaneous-anatomical snuff box]")
63
Causes of small fiber neuropathy
Diabetes Amyloidosis Fabry's disease Tangier's disease Hereditary sensory and autonomic neuropathy Sjogren's syndrome Chronic idiopathic small fiber sensory neuropathy

64
Causes of focal-multifocal neuropathies
Entrapment neuropathy: Carpal tunnel syndrome, ulnar nerve at the elbow, common peroneal at the fibular head Endocrinal: diabetes mellitus, myxedema, acromegaly, Amyloidosis Hereditary neuropathy susceptible to pressure palsy Vasculitis Multifocal motor neuropathy with conduction block

65
Causes of chronic axonal neuropathies
Drugs & Toxins: Alcohol, Vincristine, Phenytoin, TOCP, Organophosporus, Statins Infections: Leprosy, HIV, Borreliosis Connective tissue/Vasculitic: Sjogern’s syndrome; SLE; MCTD, RA Metabolic: DM, CRF Paraneoplastic: CA lung,ovary Inherited: CMT 2; CMT-X Vitamin deficiency: B12, Folate; Cobalamin, Vit E Endocrine: Hypothyroidism Paraproteinemia; Waldenstrom’s macroglobulinemia; MGUS; POEMS syndrome

66
NERVE BIOPSIES Granulomatous infiltration-Hansen’s disease Amyloidosis (Rectal biopsy) Leprosy Sarcoidosis Leucodystrophies Giant axonal neuropathy Vasculitides Demyelinating-CIDP (onion bulb formation-Schwann cell hyperplasia) Tomaculous neuropathy Mitochondrial neuropathies Refsum’s disease
 Tomaculous neuropathy. Mitochondrial neuropathies. Refsum’s disease.")
67
Learning Key Points Answer “what, when, where, & what setting?”
Perform electrodiagnosis Use laboratory testing judiciously Treat as appropriate

74
SCIENTIFIC WISDOM & ROOTS OF LIFE LONG LEARNNG
There are known knowns; there are things we know we know. We also know there are known unknowns; that is to say, we know there are some things we do not know. But there are also unknown unknowns – the ones we don’t know we don’t know. Donald Rumsfeld STAY HUNGRY [curiosity; critical thinking, self directed learning] STAY FOOLISH [ thirst for knowledge] Steve Jobs 'One thing I only know, & that is, I know nothing' Socrates.

75
THANK YOU

Similar presentations
















 Group of autoimmune conditions involving demyelination and acute axonal degeneration.>")

















