Download presentation
Presentation is loading. Please wait.

1
Medication Reconciliation Networking Session Steve Rough, MS., RPh. Director of Pharmacy University of Wisconsin Hospital and Clinics

2
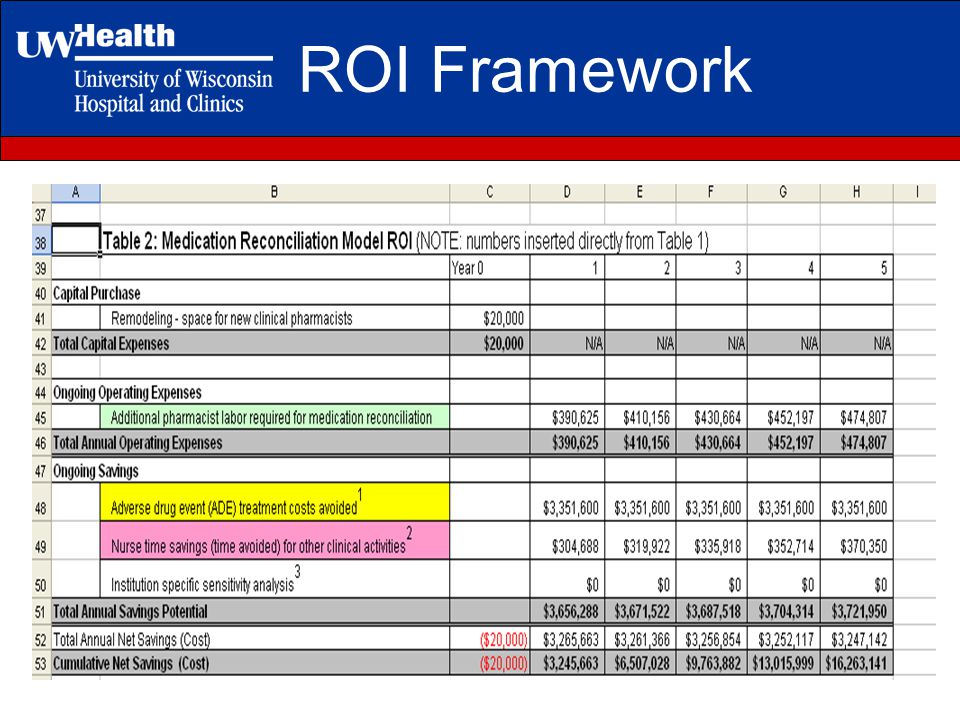
Objectives Provide a return on investment (ROI) framework for cost-justifying additional pharmacist resources for medication reconciliation Review a strategy for implementing medication reconciliation in non- inpatient care areas (clinics, procedure areas, emergency department, etc )
 framework for cost-justifying additional pharmacist resources for medication reconciliation Review a strategy for implementing medication reconciliation in non- inpatient care areas (clinics, procedure areas, emergency department, etc )")
3
ROI Framework

6
Approach for implementing medication reconciliation in non-inpatient areas

7
Key stakeholders identified –Medical staff, pharmacists, nurses, and representation from the OR, radiology, cath lab, medical records, quality, risk management, public affairs, and IT Establishment of Medication Reconciliation Steering Committee –Charged with leading the implementation process –Pharmacy and Nurse Managers serve as co-chairs –Membership from each key stakeholder group Resident major project Step 1: Prepare

8
Charge of the Medication Reconciliation Steering Committee –Developing standardized medication reconciliation processes and workflows –Developing training materials, tools and resources –Outlining specific accountabilities for staff training and implementation –Develop auditing mechanisms to ensure compliance and measure sustained compliance

9
Step 2: Assess the current system Identify all impacted areas and the manager of each area (91 areas) Gap analysis to determine levels of performance in clinics, procedure areas, emergency department –Identify all access points for patients within the organization –For each element of performance, determine areas where not fully compliant with standards Essentially 100% non-compliance!
 Gap analysis to determine levels of performance in clinics, procedure areas, emergency department –Identify all access points for patients within the organization –For each element of performance, determine areas where not fully compliant with standards Essentially 100% non-compliance!")
10
Example of Accountabilities

11
Step 3: Analyze Meet with leaders/managers from four major areas –Clinics (2 nursing directors over all 80 clinics) –Procedure areas (Radiology, Cath Lab, Infusion Center, Peds Sedation, GI, etc, etc) –Perioperative areas (Inpatient and ambulatory surgery, recovery) –Emergency Department Educate them on the required elements of NPSG 8a & 8b
 –Procedure areas (Radiology, Cath Lab, Infusion Center, Peds Sedation, GI, etc, etc) –Perioperative areas (Inpatient and ambulatory surgery, recovery) –Emergency Department Educate them on the required elements of NPSG 8a & 8b")
12
Step 3: Analyze Workflows documented for each area to fit with patient flow –Four workflows established: Paper Traditional electronic medical record (WISCR/ADS) Health Link (Epic) – new electronic health record Transplant database
 Health Link (Epic) – new electronic health record Transplant database")
13
Example of workflow diagram

14
Step 4: Plan Identify responsible person for implementation in each clinic site –Documentation of medication history, reconciliation, updates, providing list to patient and next provider of care Quantify resources needed by area –Computers –Access to information –Education –Personnel

15
Step 4: Plan Develop education materials –Include the case for medication reconciliation- it’s the right thing to do for our patients! –Steps for obtaining a complete medication list Include name, dose, route, frequency, last dose taken, indication –How to perform reconciliation –Policy expectations documentation of history and allergies on every patient providing every patient with discharge medication list send list to next provider if medication changes

16
Step 4: Plan Development of documentation tools –Paper documentation form for areas without electronic documentation –Modifications to electronic tools already available to include patient friendly terms, easier to read information provider-entered information prints out in patient-friendly format

17
Example of Paper Documentation

18
Step 4: Plan Development of auditing tools that are sustainable –Include questions on all five elements of performance on Joint Commission tracer History documented Reconciliation Clarification of discrepancies List to patient List to next provider of care

19
Step 5 & 6: Execute and Measure Educational road shows and web casts for managers and front line staff Rolling implementation, not pilots –Start with high risk area: ED, Radiology, Cath lab, surgery clinics Pharmacy resident and students audit compliance for 6 months Implement changes and improvements on the fly as needed

20
Step 7&8: Communicate & Replicate Communicate audit results to key stakeholders Big bang go-live in all remaining areas over 2 month timeframe Poster showcase for Joint Commission surveyors Optimize processes in Health Link

21
Tools Available on ASHP Website Policy and Procedure Workflows Forms Training materials ROI spreadsheet http://www.ashp.org/s_ashp/cat1c.asp?CID=489&DID=7607

22
Questions

Similar presentations







 Update to COEC John D. Halamka MD Justine M. Carr MD.>")








 introduced.>")



