Download presentation
Presentation is loading. Please wait.

2
Anticoagulant in Ischemic Stroke : An Evidence based medicine approach

3
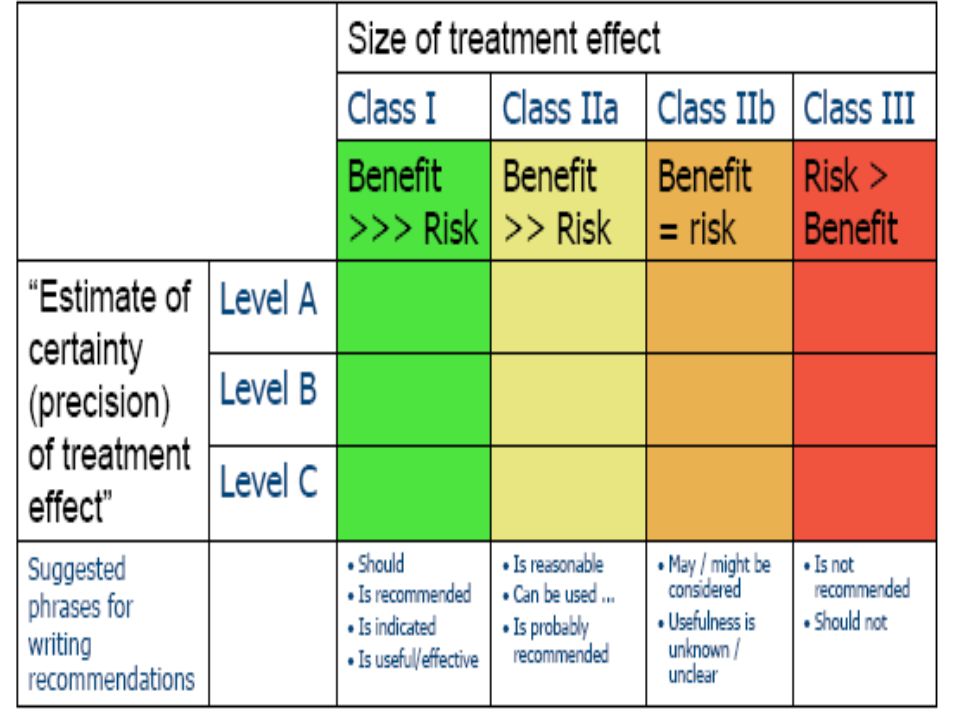
Definitions Class I Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective Class II Conditions for which there is conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of a procedure or treatment Class IIa Weight of evidence or opinion is in favor of the procedure or treatment. Class IIb Usefulness/efficacy is less well established by evidence or opinion Class III Conditions for which there is evidence and/or general agreement that the procedure or treatment is not useful/effective and in some cases may be harmful

4
Definitions Level of Evidence A: Data derived from multiple randomized clinical trials Level of Evidence B: Data derived from a single randomized trial or nonrandomized studies Level of Evidence C: Expert opinion or case studies

9
recent definition Stroke: either symptoms lasting 24 hours or imaging of an acute clinically relevant brain lesion in patients with rapidly vanishing symptoms. TIA :brief episode of neurological dysfunction caused by a focal disturbance of brain or retinal ischemia with clinical symptoms typically lasting less than 1 hour, and without evidence of infarction. ”TIA :brief episode of neurological dysfunction caused by a focal disturbance of brain or retinal ischemia with clinical symptoms typically lasting less than 1 hour, and without evidence of infarction. ”

10
Stroke subtypes The use of anti-thrombotic agents is complicated by the existence of different stroke etiologic subtypes, each of which imparts a differential risk of outcomes. In the early hours of presentation with an acute stroke, the mechanism of the infarction is frequently not clear and decisions regarding therapy are based on presumptive diagnostic subtypes.

11
Stroke subtypes: large artery disease Strokes caused by extracranial or intracranial large artery atherosclerosis appear to have the greatest risk of worsening and recurrence in the early period after hospitalization American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S

12
Stroke subtypes: large artery disease In the NINDS Stroke Data Bank, the atherosclerotic stroke subgroup had a 30% risk of worsening during the acute hospitalization and a 7.9% risk of stroke recurrence within 30 days. Sacco RL et al. Stroke 1989; 20:983-989

13
Stroke subtypes: large artery disease In the North American Symptomatic Carotid Endarterectomy Trial (NASCET), medically treated patients with transient ischemic attack (TIA) or stroke and ipsilateral carotid stenosis > 70% had a 26% risk of ipsilateral stroke at 2 years. N Engl J Med 1991; 325:445-453

14
Stroke subtypes: large artery disease Causes of worsening and recurrence in patients with large artery atherosclerotic stroke include propagation or progression of the thrombosis, distal embolism, or failure of collateral vessels to compensate for the reduced cerebral perfusion.

15
Stroke subtypes: embolic stroke one study found a high rate of early recurrence in a large group of cardioembolic stroke patients who had rheumatic heart disease, prosthetic valves, or documented intracardiac thrombi, but a sigdicantly lower recurrence rate in atrial fibrillation patients. Berge E et al. Lancet 2000; 355:120Fj-1210 Arch Intern Med 1994; 154:1449 -1457

16
Stroke subtypes: lacunar infarct Infarcts caused by small artery occlusions (lacunar strokes) have the lowest early recurrence risk and the best survival rates, but still cause significant functional morbidity.
 have the lowest early recurrence risk and the best survival rates, but still cause significant functional morbidity.")
17
Stroke subtypes: cryptogenic stroke Some strokes are difficult to reliably classify into these categories and have been labeled cyptogenic infarcts. Noninvasive vascular imaging fails to demonstrate an underlying large vessel occlusion or stenosis. No cardiac source of embolism is uncovered by echocardiography, ECG, or Holter monitoring

18
Anticoagulants for acute non-cardioembolic Stroke Studies performed in the 1950s and 1960s suggested that IV heparin therapy may be beneficial for patients with unstable ischemic stroke with as much as a 50% reduction in the likelihood of further worsening. These studies, however, were either not randomized or blinded, had poorly defined inclusion and exclusion criteria, or did not use standardized assessments for outcomes. Sage JI.. Arch Neurol l9&5; 42:315-317

19
Anticoagulants for acute non-cardioembolic Stroke Despite the clinical use of full-dose IV unfractured heparin, to our knowledge, only a single randomized trial had evaluated this regimen compared with placebo for patients with acute stable stroke since 1980. No significant difference in stroke progression or neurologic outcome was detected in this relatively small study (n = 225).lo3T his trial had a broad treatment window of 48 h from stroke onset and excluded patients with progressing stroke. Duke RJ et al. Ann Intern Med 1986; 105:825-828
.lo3T his trial had a broad treatment window of 48 h from stroke onset and excluded patients with progressing stroke. Duke RJ et al. Ann Intern Med 1986; 105:")
20
Anticoagulants for acute non-cardioembolic Stroke A large metaanalysis of 22 trials among 23,547 patients showed that immediate anticoagulation of patients with acute ischemic stroke was not associated with a significant reduction in death or dependency. Cochrane Database Syst Rev 2004. CD000024

21
Anticoagulants for acute non-cardioembolic Stroke For patients with acute ischemic stroke, we recommend against full-dose anticoagulation with IV, SC, or low- molecular-weight heparins or heparinoids (Grade 1B) American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S

22
Anticoagulants for acute non-cardioembolic Stroke Urgent anticoagulation with the goal of preventing early recurrent stroke, halting neurological worsening or improving outcomes after acute ischemic stroke is not recommended for treatment of patients with acute ischemic stroke (Class III, Level of Evidence A). Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association Circulation 2007;115;e478-e534

23
Urgent anticoagulation is not recommended for patients with moderate to severe strokes because of an increased risk of serious intracranial hemorrhagic complications (Class III, Level of Evidence A). Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association Circulation 2007;115;e478-e534

24
Antiaggregants for acute non-cardioembolic Stroke For patients with acute ischemic stroke who are not receiving thrombolysis, we recommend early aspirin therapy (initial dose of 150-325 mg) [Grade lA]. American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
![Antiaggregants for acute non-cardioembolic Stroke For patients with acute ischemic stroke who are not receiving thrombolysis, we recommend early aspirin therapy (initial dose of mg) [Grade lA].](http://images.slideplayer.com/15/4795556/slides/slide_24.jpg "American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S.")
25
Prevention of Noncardioembolic Cerebral Ischemic Events For patients with noncardioembolic stroke or TIA, we recommend antiplatelet agents over oral anticoagulation (Grade 1A). American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
26
(Class III, Level of Evidence C). The administration of clopidogrel alone or in combination with aspirin is not recommended for the treatment of acute ischemic stroke Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association Circulation 2007;115;e478-e534

27
recent acute myocardial infarction, other acute coronary syndrome In those with a recent acute myocardial infarction, other acute coronary syndrome, or a recently placed coronary stent, we recommend clopidogrel plus aspirin (75 to 100 mg) [Grade 1A]. The optimal duration of dual antiplatelet therapy depends on the specific cardiac indications In those with a recent acute myocardial infarction, other acute coronary syndrome, or a recently placed coronary stent, we recommend clopidogrel plus aspirin (75 to 100 mg) [Grade 1A]. The optimal duration of dual antiplatelet therapy depends on the specific cardiac indications
![recent acute myocardial infarction, other acute coronary syndrome In those with a recent acute myocardial infarction, other acute coronary syndrome, or a recently placed coronary stent, we recommend clopidogrel plus aspirin (75 to 100 mg) [Grade 1A].](http://images.slideplayer.com/15/4795556/slides/slide_27.jpg "The optimal duration of dual antiplatelet therapy depends on the specific cardiac indications In those with a recent acute myocardial infarction, other acute coronary syndrome, or a recently placed coronary stent, we recommend clopidogrel plus aspirin (75 to 100 mg) [Grade 1A]. The optimal duration of dual antiplatelet therapy depends on the specific cardiac indications.")
28
atrial fibrillation In patients with atrial fibrillation who have suffered a recent stroke or TIA, we recommend long-term oral anticoagulation (target INR, 2.5; range, 2.0 to 3.0) [Grade 1A]. In patients with atrial fibrillation who have suffered a recent stroke or TIA, we recommend long-term oral anticoagulation (target INR, 2.5; range, 2.0 to 3.0) [Grade 1A].
![atrial fibrillation In patients with atrial fibrillation who have suffered a recent stroke or TIA, we recommend long-term oral anticoagulation (target INR, 2.5; range, 2.0 to 3.0) [Grade 1A].](http://images.slideplayer.com/15/4795556/slides/slide_28.jpg "In patients with atrial fibrillation who have suffered a recent stroke or TIA, we recommend long-term oral anticoagulation (target INR, 2.5; range, 2.0 to 3.0) [Grade 1A]..")
29
atrial fibrillation we recommend initiation of oral anticoagulation therapy within 2 weeks of a cardioembolic stroke; however, for patients with large infarcts or other risk factors for hemorrhage, additional delays may be appropriate.we recommend initiation of oral anticoagulation therapy within 2 weeks of a cardioembolic stroke; however, for patients with large infarcts or other risk factors for hemorrhage, additional delays may be appropriate.

30
aortic atherosclerotic lesions In patients with stroke associated with, we recommend antiplatelet therapy over no therapy (Grade 1A). In patients with stroke associated with, we recommend antiplatelet therapy over no therapy (Grade 1A).
..")
31
mobile aortic arch thrombi For patients with cryptogenic stroke associated with mobile aortic arch thrombi, we suggest either oral anticoagulation or antiplatelet agents (Grade 2C). For patients with cryptogenic stroke associated with mobile aortic arch thrombi, we suggest either oral anticoagulation or antiplatelet agents (Grade 2C).
..")
32
cryptogenic ischemic stroke and a PFO In patients with cryptogenic ischemic stroke and a PFO, we recommend antiplatelet therapy over no therapy (Grade 1A) and suggest antiplatelet therapy over warfarin (Grade 2A). In patients with cryptogenic ischemic stroke and a PFO, we recommend antiplatelet therapy over no therapy (Grade 1A) and suggest antiplatelet therapy over warfarin (Grade 2A).
 and suggest antiplatelet therapy over warfarin (Grade 2A)..")
33
mitral valve strands or prolapse In patients with mitral valve strands or prolapse who have a history of TIA or stroke, we recommend antiplatelet therapy (Grade 1A). In patients with mitral valve strands or prolapse who have a history of TIA or stroke, we recommend antiplatelet therapy (Grade 1A).
..")
34
Embolic Stroke: Atrial fibrillation(AF) For patients with ischemic stroke or TIA with persistent or paroxysmal (intermittent) AF, anticoagulation with adjusted-dose warfarin (target INR, 2.5; range, 2.0 to 3.0) is recommended (Class I, Level of Evidence A) For patients with ischemic stroke or TIA with persistent or paroxysmal (intermittent) AF, anticoagulation with adjusted-dose warfarin (target INR, 2.5; range, 2.0 to 3.0) is recommended (Class I, Level of Evidence A) Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

35
Embolic Stroke: Atrial fibrillation(AF) For patients unable to take oral anticoagulants, aspirin 325 mg/d is recommended (Class I, Level of Evidence A). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449 ….75-325 mg/d (Grade 1B). American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S.")
36
Embolic Stroke: recent Myocardial infarction For patients with an ischemic stroke or TIA caused by an acute MI in whom LV mural thrombus is identified by echocardiography or another form of cardiac imaging, oral anticoagulation is reasonable, aiming for an INR of 2.0 to 3.0 for at least 3 months and up to 1 year (Class IIa, Level of Evidence B). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

37
Embolic Stroke: recent Myocardial infarction Aspirin should be used concurrently for ischemic coronary artery disease during oral anticoagulant therapy in doses up to 162 mg/d (Class IIa, Level of Evidence A). Aspirin should be used concurrently for ischemic coronary artery disease during oral anticoagulant therapy in doses up to 162 mg/d (Class IIa, Level of Evidence A). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449
. Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449.")
38
Embolic Stroke: dilated cardiomyipathy For patients with ischemic stroke or TIA who have dilated cardiomyopathy, either warfarin (INR, 2.0 to 3.0) or antiplatelet therapy may be considered for prevention of recurrent events (Class IIb, Level of Evidence C) Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

39
Embolic Stroke: mitral valve disease For patients with ischemic stroke or TIA who have rheumatic mitral valve disease, whether or not AF is present, long-term warfarin therapy is reasonable, with a target INR of 2.5 (range, 2.0 to 3.0) (Class IIa, Level of Evidence C). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

40
Embolic Stroke: mitral valve disease Antiplatelet agents should not routinely be added to warfarin to avoid the additional bleeding risk (Class III, Level of Evidence C). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

41
Embolic Stroke: mitral valve disease For patients with ischemic stroke or TIA with rheumatic mitral valve disease, whether or not AF is present, who have a recurrent embolism while receiving warfarin, adding aspirin (81 mg/d) is suggested (Class IIa, Level of Evidence C) For patients with ischemic stroke or TIA with rheumatic mitral valve disease, whether or not AF is present, who have a recurrent embolism while receiving warfarin, adding aspirin (81 mg/d) is suggested (Class IIa, Level of Evidence C) Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

42
Embolic Stroke: mitral valve prolapse For patients with mitral valve prolapse who have ischemic stroke or TIAs, antiplatelet therapy is reasonable (ClassIIa, Level of Evidence C) Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449 …..Grade I A American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
43
Embolic Stroke: Mitral Annular Calcification(MAC) For patients with ischemic stroke or TIA and Mitral Annular Calcification(MAC) not documented to be calcific, antiplatelet therapy may be considered (Class IIb, Level of Evidence C). For patients with ischemic stroke or TIA and Mitral Annular Calcification(MAC) not documented to be calcific, antiplatelet therapy may be considered (Class IIb, Level of Evidence C). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449
 not documented to be calcific, antiplatelet therapy may be considered (Class IIb, Level of Evidence C). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449.")
44
Embolic Stroke: Mitral Annular Calcification(MAC) Among patients with mitral regurgitation caused by MAC without AF, antiplatelet or warfarin therapy may be considered (Class IIb, Level of Evidence C) Among patients with mitral regurgitation caused by MAC without AF, antiplatelet or warfarin therapy may be considered (Class IIb, Level of Evidence C) Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

45
Embolic Stroke: aortic valve disease For patients with ischemic stroke or TIA and who do not have AF, antiplatelet therapy may be considered (Class IIb, Level of Evidence C) For patients with ischemic stroke or TIA and who do not have AF, antiplatelet therapy may be considered (Class IIb, Level of Evidence C) Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

46
Embolic Stroke: prosthetic heart valves For patients with ischemic stroke or TIA who have modern mechanical prosthetic heart valves, oral anticoagulants are recommended, with an INR target of 3.0 (range, 2.5 to 3.5) (Class I, Level ofEvidence B). For patients with ischemic stroke or TIA who have modern mechanical prosthetic heart valves, oral anticoagulants are recommended, with an INR target of 3.0 (range, 2.5 to 3.5) (Class I, Level ofEvidence B). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449
 (Class I, Level ofEvidence B). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449.")
47
Embolic Stroke: prosthetic heart valves For patients with mechanical prosthetic heart valves who have an ischemic stroke or systemic embolism despite adequate therapy with oral anticoagulants, aspirin 75 to 100 mg/d in addition to oral anticoagulants and maintenance of the INR at a target of 3.0(range 2.5 to 3.5) are reasonable (Class IIa, Level of Evidence B). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449

48
Embolic Stroke: prosthetic heart valves For patients with ischemic stroke or TIA who have bioprosthetic heart valves with no other source of thromboembolism, anticoagulation with warfarin (INR 2.0 to 3.0) may be considered (Class IIb, Levelof Evidence C). For patients with ischemic stroke or TIA who have bioprosthetic heart valves with no other source of thromboembolism, anticoagulation with warfarin (INR 2.0 to 3.0) may be considered (Class IIb, Levelof Evidence C). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449
 may be considered (Class IIb, Levelof Evidence C). Guidelines for Prevention of Stroke in Patients With Ischemic Stroke orTransient Ischemic Attack. Circulation. 2006;113;e409-e449.")
49
Embolic stroke: patent foramen ovale In patients with cryptogenic ischemic stroke and a patent foramen ovale, we recom- mend antiplatelet therapy over no therapy (Grade 1A) and suggest antiplatelet agents over anticoagulation (Grade 2A). American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
50
Embolic stroke: aortic plaque In patients with stroke associated with aor tic atherosclerotic lesions, we recommend anti-platelet therapy over no therapy (Grade 1A). American College of Chest Physicians Gvidenc Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S- 669S
. CHEST 2008; 133:630S- 669S.")
51
Embolic stroke: aortic plaque For patients with cryptogenic stroke associated with mobile aortic arch thrombi, we suggest either oral anticoagulation or antiplatelet agents (Grade 2C). American College of Chest Physicians Gvidenc Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
52
venous sinus thrombosis we recommend that clinicians use UFH (Grade 1B) or low-molecular-weight heparin (Grade 1B) over no anticoagulant therapy during the acute phase, even in the presence of hemorrhagic infarction. In these patients, we recommend continued use of vitamin K antagonist therapy for up to 12 months (target INR, 2.5; range, 2.0 – 3.0) [Grade 1B]. we recommend that clinicians use UFH (Grade 1B) or low-molecular-weight heparin (Grade 1B) over no anticoagulant therapy during the acute phase, even in the presence of hemorrhagic infarction. In these patients, we recommend continued use of vitamin K antagonist therapy for up to 12 months (target INR, 2.5; range, 2.0 – 3.0) [Grade 1B].
 [Grade 1B]. we recommend that clinicians use UFH (Grade 1B) or low-molecular-weight heparin (Grade 1B) over no anticoagulant therapy during the acute phase, even in the presence of hemorrhagic infarction. In these patients, we recommend continued use of vitamin K antagonist therapy for up to 12 months (target INR, 2.5; range, 2.0 – 3.0) [Grade 1B]..")
53
neuroprotective actions At present, no intervention with putative neuroprotective actions has been established as effective in improving outcomes after stroke, and therefore none currently can be recommended (Class III, Level of Evidence A). Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association Circulation 2007;115;e478- e534

54
osmotherapy Although aggressive medical measures, including osmotherapy, have been recommended for treatment of deteriorating patients with malignant brain edema after large cerebral infarction, these measures are unproven (Class IIa, Level of Evidence C). Hyperventilation is a short-lived intervention. Medical measures may delay decompressive surgery Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association Circulation 2007;115;e478-e534

55
anticonvulsants Prophylactic administration of anticonvulsants to patients with stroke but who have not had seizures is not recommended (Class III, Level of Evidence C). Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association Circulation 2007;115;e478-e534

56
Prevention of Deep Vein Thrombosis and Pulmonary Embolism For acute stroke patients with restricted mobility, we recommend prophylactic low- dose SC heparin or low-molecular-weight heparins (Grade IA). American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
57
Prevention of Deep Vein Thrombosis and Pulmonary Embolism For patients who have contraindcations to anticoagulants, we recommend intennittent pneumatic compression (IPC) devices or elastic stockings(Grade 1B). American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
58
Prevention of Deep Vein Thrombosis and Pulmonary Embolism In patients with an acute intracerebral hematoma (ICH), we recommend the initial use of IPC devices (Grade 1B). American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
59
Prevention of Deep Vein Thrombosis and Pulmonary Embolism In stable patients with an acute intracerebral hematoma (ICH),, we suggest low-dose SCheparin as soon as the second day after the onset of the hemorrhage (Grade 2C) In stable patients with an acute intracerebral hematoma (ICH),, we suggest low-dose SCheparin as soon as the second day after the onset of the hemorrhage (Grade 2C) American College of Chest Physicians Gvidenc Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S

60
For acute stroke patients with restricted mobility, we recommend prophylactic low-dose SC heparin or low-molecular-weight heparins (Grade 1A). For acute stroke patients with restricted mobility, we recommend prophylactic low-dose SC heparin or low-molecular-weight heparins (Grade 1A).
..")
61
Thrombolytic Therapy

62
Inclusion Criteria Age ≥18 years,Age ≥18 years, clinical diagnosis of stroke with a clinically meaningful neurologic deficit,clinical diagnosis of stroke with a clinically meaningful neurologic deficit, clearly defined time of onset of <180 min before treatment,clearly defined time of onset of <180 min before treatment, baseline CT showing no evidence of intracranial hemorrhage. baseline CT showing no evidence of intracranial hemorrhage.

63
Exclusion Criteria Minor or rapidly improving symptoms or signs,Minor or rapidly improving symptoms or signs, CT signs of intracranial hemorrhage,CT signs of intracranial hemorrhage, a history of intracranial hemorrhage, seizure at stroke onset, stroke or serious head injury within 3 months,a history of intracranial hemorrhage, seizure at stroke onset, stroke or serious head injury within 3 months, major surgery or serious trauma within 2 weeks, major surgery or serious trauma within 2 weeks, GI or urinary tract hemorrhage within 3 weeks,GI or urinary tract hemorrhage within 3 weeks, systolic BP >185 mm Hg, diastolic BP >110 mm Hg, aggressive treatment required to lower BP,systolic BP >185 mm Hg, diastolic BP >110 mm Hg, aggressive treatment required to lower BP, glucose 400 mg/dL,glucose 400 mg/dL,

64
symptoms of subarachnoid hemorrhage,symptoms of subarachnoid hemorrhage, arterial puncture at a noncompressible site or lumbar puncture within 1 week,arterial puncture at a noncompressible site or lumbar puncture within 1 week, platelet count <100,000/mm3, platelet count <100,000/mm3, heparin therapy within 48 h associated with elevated activated partial thromboplastin time, heparin therapy within 48 h associated with elevated activated partial thromboplastin time, clinical presentation suggesting post-myocardial infarction pericarditis,clinical presentation suggesting post-myocardial infarction pericarditis, pregnant women, pregnant women, anticoagulation due to oral anticoagulants (international normalized ratio [INR] >1.7). anticoagulation due to oral anticoagulants (international normalized ratio [INR] >1.7).
![symptoms of subarachnoid hemorrhage,symptoms of subarachnoid hemorrhage, arterial puncture at a noncompressible site or lumbar puncture within 1 week,arterial puncture at a noncompressible site or lumbar puncture within 1 week, platelet count <100,000/mm3, platelet count <100,000/mm3, heparin therapy within 48 h associated with elevated activated partial thromboplastin time, heparin therapy within 48 h associated with elevated activated partial thromboplastin time, clinical presentation suggesting post-myocardial infarction pericarditis,clinical presentation suggesting post-myocardial infarction pericarditis, pregnant women, pregnant women, anticoagulation due to oral anticoagulants (international normalized ratio [INR] >1.7).](http://images.slideplayer.com/15/4795556/slides/slide_64.jpg "anticoagulation due to oral anticoagulants (international normalized ratio [INR] >1.7)..")
65
(Grade 1A). For eligible patients, we recommend administration of IV tPA in a dose of 0.9 mg/kg (maximum of 90 mg), with 10% of the total dose given as an initial bolus and the remainder infused over 60 min, provided that treatment is initiated within 3 h of clearly defined symptom onset For eligible patients, we recommend administration of IV tPA in a dose of 0.9 mg/kg (maximum of 90 mg), with 10% of the total dose given as an initial bolus and the remainder infused over 60 min, provided that treatment is initiated within 3 h of clearly defined symptom onset
, with 10% of the total dose given as an initial bolus and the remainder infused over 60 min, provided that treatment is initiated within 3 h of clearly defined symptom onset For eligible patients, we recommend administration of IV tPA in a dose of 0.9 mg/kg (maximum of 90 mg), with 10% of the total dose given as an initial bolus and the remainder infused over 60 min, provided that treatment is initiated within 3 h of clearly defined symptom onset.")
66
(Grade 2B) For patients with extensive (more than one third of the middle cerebral artery territory) and clearly identifiable hypodensity on CT, we suggest not using of tPA For patients with extensive (more than one third of the middle cerebral artery territory) and clearly identifiable hypodensity on CT, we suggest not using of tPA American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S

67
(Grade 2A) For patients with acute ischemic stroke of >3 h but 3 h but <4.5 h we suggest clinicians do not use IV tPA American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S- 669S

68
(Grade 1A). For patients with acute stroke onset of >4.5 h, we recommend against the use of IV tPA For patients with acute stroke onset of >4.5 h, we recommend against the use of IV tPA American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
69
(Grade 1A). For patients with acute ischemic stroke, we recommend against streptokinase For patients with acute ischemic stroke, we recommend against streptokinase American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
70
(Grade 2C) For patients with angiographically demonstrated middle cerebral artery occlusion and without major early infarct signs on the baseline CT or MRI scan, who can be treated within 6 h of symptom onset, we suggest intraarterial thrombolytic therapy with tPA for selected patients in centers with the appropriate neurologic and interventional expertise For patients with angiographically demonstrated middle cerebral artery occlusion and without major early infarct signs on the baseline CT or MRI scan, who can be treated within 6 h of symptom onset, we suggest intraarterial thrombolytic therapy with tPA for selected patients in centers with the appropriate neurologic and interventional expertise
 For patients with angiographically demonstrated middle cerebral artery occlusion and without major early infarct signs on the baseline CT or MRI scan, who can be treated within 6 h of symptom onset, we suggest intraarterial thrombolytic therapy with tPA for selected patients in centers with the appropriate neurologic and interventional expertise For patients with angiographically demonstrated middle cerebral artery occlusion and without major early infarct signs on the baseline CT or MRI scan, who can be treated within 6 h of symptom onset, we suggest intraarterial thrombolytic therapy with tPA for selected patients in centers with the appropriate neurologic and interventional expertise")
71
(Grade 2C). For patients with acute basilar artery thrombosis and without major CT/MRI evidence of infarction, we suggest either intraarterial or IV thrombolysis with tPA depending on available resources and capabilities For patients with acute basilar artery thrombosis and without major CT/MRI evidence of infarction, we suggest either intraarterial or IV thrombolysis with tPA depending on available resources and capabilities American College of Chest Physicians Evidence- Based Clinical Practice Guidelines (8th Edition). CHEST 2008; 133:630S-669S
. CHEST 2008; 133:630S-669S.")
Similar presentations