Download presentation
Presentation is loading. Please wait.

2
Discussion 8 April 23rd, 2007 Ryan Klimczak

3
Growing old successfully: Approximately 25% role of genetics in determining longevity (twin/family studies) Environmental affect on longevity (caloric restriction)
 Environmental affect on longevity (caloric restriction)")
5
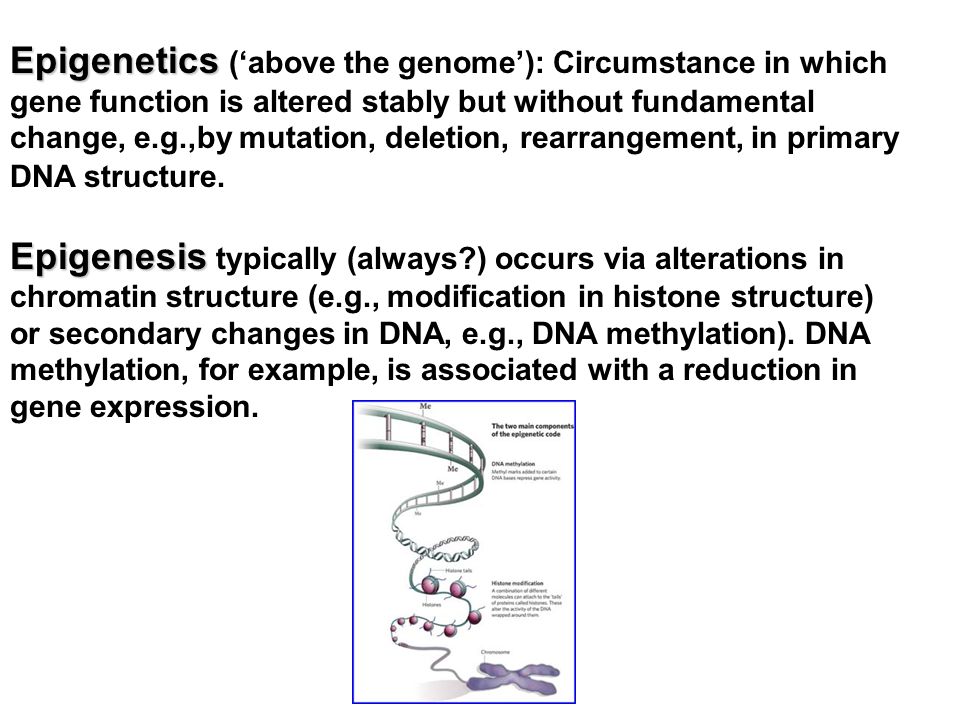
Epigenetics Epigenetics (‘above the genome’): Circumstance in which gene function is altered stably but without fundamental change, e.g.,by mutation, deletion, rearrangement, in primary DNA structure. Epigenesis Epigenesis typically (always?) occurs via alterations in chromatin structure (e.g., modification in histone structure) or secondary changes in DNA, e.g., DNA methylation). DNA methylation, for example, is associated with a reduction in gene expression.
 occurs via alterations in chromatin structure (e.g., modification in histone structure) or secondary changes in DNA, e.g., DNA methylation). DNA methylation, for example, is associated with a reduction in gene expression..")
6
Barker Hypothesis Prenatal events establish lifelong physiological patterns that may manifest as disease processes in later life Dutch famine

7
Aging of the Urinary Tract

8
Nephron & Renal Circulation

9
Table 19-1 Major Functions of the Kidney Water and electrolyte regulation Metabolic products excretion Hydrogen ion excretion and maintenance of blood pH Endocrine functions: Renin-angiotensin secretion (blood pressure) Vitamin D activation (Ca ++ metabolism) Erythropoietin secretion (hematopoiesis)
 Vitamin D activation (Ca ++ metabolism) Erythropoietin secretion (hematopoiesis)")
10
2. Renal Tubules divided into: Proximal Tubule, mostly reabsorption of water & solutes Loop of Henle, mostly reabsorption of water & salt Distal Tubule, mostly water & salt (under influence of aldosterone) reabsorption and acidification of urine Collecting Duct, water reabsorption under the influence of ADH (antidiuretic hormone from posterior pituitary) 1. Glomerulus: Tufts of capillaries between afferent and efferent renal arterioles. Filtration is through a fenestrated endothelium separated from the basal membrane by podocytes. Filtrate is the same as plasma but without proteins.
 reabsorption and acidification of urine Collecting Duct, water reabsorption under the influence of ADH (antidiuretic hormone from posterior pituitary) 1. Glomerulus: Tufts of capillaries between afferent and efferent renal arterioles. Filtration is through a fenestrated endothelium separated from the basal membrane by podocytes. Filtrate is the same as plasma but without proteins..")
11
Distal and Collecting Tubules function is regulated by ADH (antidiuretic hormone) secreted by neuroendocrine hypothalamus stored and released from the posterior pituitary Juxtaglomerular Apparatus : located between afferent artery and distal tubule secretes the enzyme renin renin acts on the liver protein angiotensinogen to form angiotensin I, and angiotensin is transformed into angiotensin II in the lungs angiotensin II is a very potent hypertensive substance; it also stimulates the release of aldosterone from the adrenal cortex Regulation of Kidney function:
 secreted by neuroendocrine hypothalamus stored and released from the posterior pituitary Juxtaglomerular Apparatus : located between afferent artery and distal tubule secretes the enzyme renin renin acts on the liver protein angiotensinogen to form angiotensin I, and angiotensin is transformed into angiotensin II in the lungs angiotensin II is a very potent hypertensive substance; it also stimulates the release of aldosterone from the adrenal cortex Regulation of Kidney function:")
12
Hypothalamus, Posterior Hypophysis, and their Hormones Hypothalamus

13
Table 19-2 Common Renal Problems in the Elderly Renal Failure Impaired drug excretion ( Think about kidney when giving a drug) Urinary tract infections Hypertension Miscellaneous disorders: Tuberculosis Nephritis Diabetes, etc.
 Urinary tract infections Hypertension Miscellaneous disorders: Tuberculosis Nephritis Diabetes, etc.")
14
Table 19-3 Some Signs of Renal Failure Generalized edema Acidosis Increased circulating non-protein nitrogen (urea) Increased circulating urinary retention products (e.g. creatinine, uric acid)
.")
15
Table 19-4 Selected Causes of Acute Renal Failure PRE-RENAL: (problems BEFORE the kidney) Loss of body fluids Inadequate fluid intake Surgical shock or myocardial infarction RENAL: (problems IN the kidney) Drug toxicity ( Think about kidney when giving a drug) Immune reactions Infectious diseases Thrombosis POST-RENAL: (problems AFTER the kidney) Urinary tract obstruction
 Loss of body fluids Inadequate fluid intake Surgical shock or myocardial infarction RENAL: (problems IN the kidney) Drug toxicity ( Think about kidney when giving a drug) Immune reactions Infectious diseases Thrombosis POST-RENAL: (problems AFTER the kidney) Urinary tract obstruction")
16
Functions of the bladder Filling with urine from the kidneys Micturition: emptying of bladder by muscle contraction and opening of sphincters. Principle muscle: Detrusor muscle (bladder’s body): when it contracts, the bladder empties Sphincters: Internal (involuntary; smooth muscle) and external (voluntary to some degree; skeletal muscle)
: when it contracts, the bladder empties Sphincters: Internal (involuntary; smooth muscle) and external (voluntary to some degree; skeletal muscle).")
17
For Micturition: 1. Internal and external sphincters have to relax 2. Bladder has to contract (detrosor muscle)
.")
18
Storage: Table 19-7 Physiologic Requirements for Continence No involuntary bladder contractions Appropriate bladder sensation Closed bladder outlet Low pressure accommodation of urine Motivation to be continent Adequate cognitive function Adequate mobility and dexterity Normal lower urinary tract function

19
Emptying: Table 19-7 Physiologic Requirements for Continence Normal bladder contraction Lack of anatomic obstruction Coordinated sphincter relaxation & bladder contraction Absence of environmental/iatrogenic barriers

20
Figure 19-6: Mnemonic device for causes of acute urinary incontinence

21
Table 19-8 Age-Related Changes Contributing to Incontinence In Females Estrogen deficiency Weak pelvic floor and bladder outlet Decreased urethral muscle tone Atrophic vaginitis In Males Increased prostatic size Impaired urinary flow Urinary retention Detrusor muscle instability

22
Weakness of pelvic muscles Inability to avoid voiding when bladder full overdistended, non-contractile blood cognitive, emotional problems

23
Questions What are the major parts of the kidney and what control mechanisms act at each part? What are the muscles involved in micturition? What are the requirements for continence? What are some causes of incontinence? How might these be treated?

24
Evidence for Decline in Immune Function with Aging Aged Individuals have: 1) Increased incidence of INFECTIONS: For example: pneumonia, influenza, tuberculosis, meningitis, urinary tract infections 2) Increased incidence of AUTOIMMUNE DISEASE: For example: rheumatoid arthritis, lupus, hepatitis, thyroiditis (graves- hyper/hashimotos-hypo), multiple sclerosis(Predisposition toward these diseases is related to Human Leukocyte Antigens HLA genes) 3) Increased CANCER INCIDENCE: For Example: prostate, breast, lung, throat/neck/head, stomach/colon/bladder, skin, leukemia, pancreatic 4) TOLERANCE to organ transplants: Kidneys, skin, bone marrow, heart (valves), liver, pancreas, lungs
 Increased incidence of INFECTIONS: For example: pneumonia, influenza, tuberculosis, meningitis, urinary tract infections 2) Increased incidence of AUTOIMMUNE DISEASE: For example: rheumatoid arthritis, lupus, hepatitis, thyroiditis (graves- hyper/hashimotos-hypo), multiple sclerosis(Predisposition toward these diseases is related to Human Leukocyte Antigens HLA genes) 3) Increased CANCER INCIDENCE: For Example: prostate, breast, lung, throat/neck/head, stomach/colon/bladder, skin, leukemia, pancreatic 4) TOLERANCE to organ transplants: Kidneys, skin, bone marrow, heart (valves), liver, pancreas, lungs")
25
Function of Immune System is PROTECTION against: 1.Bacteria 2.Virus 3.Fungus/ multicellular parasites 4.Cancer 5.Toxins 6.( 5,000 daltons--protein/lipid/CHO/nucleic acids)
")
26
Tissues and Organs Important for Immune Function Cells derived from stem cells: liver, bone marrow Cells are stored, multiply, interact, and mature in: thymus, spleen, lymph nodes, blood Transport: lymphatic vessels Important Cell types: Lymphocytes, neutrophils, macrophages, natural killer cells Accessory Organs Appendix, tonsils, intestines

27
A) T cells: stored & mature in thymus-migrate throughout the body -Killer Cells Perform lysis (infected cells) Cell mediated immune response -Helper Cells Enhance T killer or B cell activity -Suppressor Cells Reduce/suppress immune activity May help prevent auto immune disease Lymphocytes
 T cells: stored & mature in thymus-migrate throughout the body -Killer Cells Perform lysis (infected cells) Cell mediated immune response -Helper Cells Enhance T killer or B cell activity -Suppressor Cells Reduce/suppress immune activity May help prevent auto immune disease Lymphocytes")
28
B)B-Cells: stored and mature in spleen secrete highly specific Ab to bind foreign substance (antigen: Ag), form Ab-Ag complex responsible for humoral response perform antigen processing and presentation differentiate into plasma cells (large Ab secretion) Lymphocytes (cont.)
B-Cells: stored and mature in spleen secrete highly specific Ab to bind foreign substance (antigen: Ag), form Ab-Ag complex responsible for humoral response perform antigen processing and presentation differentiate into plasma cells (large Ab secretion) Lymphocytes (cont.)")
29
Other cell types Neutrophils- found throughout body, in blood. Phagocytosis of Ab-Ag CX Macrophages- throughout body, blood, lymphatics –Phagocytose non-specifically and specifically (non Ab coated Ag) –perform Ag processing and presentation –secrete lymphokines/ cytokines to stimulate T helpers Natural Killer Cells-in blood throughout body –destroy cancer cells
 –perform Ag processing and presentation –secrete lymphokines/ cytokines to stimulate T helpers Natural Killer Cells-in blood throughout body –destroy cancer cells.")
30
Complement Series of enzymes which are sequentially activated and result in lysis of cell membrane of infected cell at bacterium Complement binding and activation ~35 enzymes and factors involved in cascade

34
5 classes of Ig IgG: 150,000 m.w. most abundant in blood, cross placental barrier, fix complement, induce macrophage engulfment IgA: associated with mucus and secretory glands, respiratory tract, intestines, saliva, tears, milk variable size IgM: 900,000 m.w. 2nd most abundant, fix complement, induce macrophage engulfment, primary immune response

35
5 Classes of Ig IgD: Low level in blood, surface receptor on B- cell IgE: Binds receptor on mast cells (basophils) secretes histamine, role in allergic reactions Increased histamine leads to vasodilation, which leads to increase blood vessel permeability. This induces lymphocyte immigration swelling and redness.

36
Thymus involution

37
Experimental Evidence for Age Related Decrease in Immune Function Dependent on T & B cell function Sheep RBC (Antigen) 1st into human
 1st into human")
38
Table 15-2: Some Aging Related Effects on B-Cells Decreased number of circulating and peripheral blood B cells Alteration in B-cell repertoire (diversity) Decreased generation of primary and secondary memory B cells General decline in lymphoproliferative capacity
 Decreased generation of primary and secondary memory B cells General decline in lymphoproliferative capacity")
39
Table 15-14: Some Aging-Related Effects on T-cells General decline in cell mediated immunological function T-cell population is hyporesponsive Decrease T cell diversity Increase in proportion of memory and activated T-cells while naïve T-cells decrease

40
Table 15-16 Influence of Aging on Macrophages and Granulocytes General functional impairment of macrophages and granulocytes

41
Table 15-15 Aging-Related Changes in Natural Killer (NK) Cells General decline in cell function Good correlation between mortality risk and NK cell number—ie cancer Impairment of cytotoxic capacity per NK cell
 Cells General decline in cell function Good correlation between mortality risk and NK cell number—ie cancer Impairment of cytotoxic capacity per NK cell")
42
Table 15-13 Aging-Related Shifts in Antibodies General decrease in humoral responsiveness: Decline in high affinity protective antibody production Increased auto-antibodies: Organ specific and non-organ specific antibodies directed to self

43
Table 15-10 Some Aging-Related Shifts in Cytokines CYTOKINES - influence proliferation, differentiation, and survival of lymphoid cells; has numerous actions on other body cells Increased proinflammatory cytokines IL-1, IL-6, TNF- Increased cytokine production imbalance

44
Table 15-17 Major Diseases Associated with Aging in Immune Function Increased tumor incidence and cancer Increased incidence of infectious diseases caused by: E. Coli Streptococcus pneumonia Mycobacterium tuberculosis Pseudomonas aeruginosa Herpes virus Gastroenteritis, bronchitis, and influenza Reappearance of latent viral infection Autoimmune diseases and inflammatory reactions: Arthritis Diabetes Osteoporosis Dementia

45
Table 15-9 Hallmarks of Immunosenescence Atrophy of the thymus: decreased size decreased cellularity (fewer thymocytes and epithelial cells) morphologic disorganization Decline in the production of new cells from the bone marrow Decline in the number of cells exported by the thymus gland Decline in responsiveness to vaccines Reduction in formation and reactivity of germinal center nodules in lymph nodes where B-cells proliferate Decreased immune surveillance by T lymphocytes and NK cells
 morphologic disorganization Decline in the production of new cells from the bone marrow Decline in the number of cells exported by the thymus gland Decline in responsiveness to vaccines Reduction in formation and reactivity of germinal center nodules in lymph nodes where B-cells proliferate Decreased immune surveillance by T lymphocytes and NK cells")
46
Questions What are aging related changes in B cells? T cells? Cytokines? Antibodies? Natural killer cells? What disease is someone more likely to get if they have fewer/less functional NK cells?

Similar presentations












 Immune system.>")








