Download presentation
Presentation is loading. Please wait.

1
EPIDEMIOLOGY OF HIV/AIDS IN PENNSYLVANIA Module 1 *Introduction to Epidemiologic Methods for Assessment of Unmet Needs for HIV-related Primary Medical Care Benjamin Richard H. Muthambi, DrPH, MPH State HIV/AIDS Epidemiologist

2
Outline for Module 1 Components of HRSA’s Framework of Comprehensive Needs Assessment – The Quandary of Definitions of Unmet Needs – Types of Needs Assessment Data

3
Definitions of Primary Health Care, Primary Medical Care, & Service Gaps – Collaboration between Prevention & Care: Opportunities & Challenges Characteristics of a Comprehensive Needs Assessment Importance of/Rationale for Estimating Unmet Needs for Primary Health Care Assessment of Unmet Need Within the Care Act Planning Processes; Methodological Considerations in Estimating Unmet Needs; Methods: HRSA-Defined Framework for Measuring Unmet Need; – Introduction – Definitions for Calculating Unmet Needs for HIV Primary Medical Care – The Unmet Needs Framework – Data Sources – Setting Up the Unmet Needs Framework – Population Input Examples – Care Input Example – Calculating Unmet Needs Estimates – Costs – Integrating the Unmet Needs Framework with Other Needs Assessment Activities

4
Components of HRSA’s Framework for Comprehensive Needs Assessment Integrated Epidemiologic Profile of HIV; Assessment of service needs among affected populations; Resource inventory; Profile of provider capacity and capability; Assessment of unmet need and service gaps; Annual Updates;

5
Integrated Epidemiologic Profile of HIV: – Describes the current status of the epidemic in the service area: of greater relevance to care, the Epidemiologic profile specifically describes the prevalence of HIV and AIDS overall and among defined subpopulations; Components of HRSA’s Framework for Comprehensive Needs Assessment

6
Resource inventory: – Describes organizations and individuals providing services across the full spectrum of HIV services accessible to PLWH in the service area, regardless of funding source. www.stophiv.pitt.eduwww.stophiv.pitt.edu Profile of provider capacity and capability: – Identifies the extent to which services identified in the resource inventory are accessible, available, and appropriate for PLWH, including specific subpopulations; Describe Capacity: how much of which services a provider can deliver ; Describe Capability: the degree to which a provider is actually accessible and has the needed expertise to provide services ; Assessment of barriers to PLWH receiving services is an important aspect of this component (i.e., the profile should inquire from PLWH directly or service providers the barriers faced in accessing services); Provider profiles may also explore client perceptions of service quality and appropriateness: assessment of client satisfaction is a complex effort that should be undertaken thoroughly in the planning body's quality improvement process. Components of HRSA’s Framework for Comprehensive Needs Assessment
; Provider profiles may also explore client perceptions of service quality and appropriateness: assessment of client satisfaction is a complex effort that should be undertaken thoroughly in the planning body s quality improvement process. Components of HRSA’s Framework for Comprehensive Needs Assessment.")
7
Assessment of service needs among affected populations: – Includes barriers that prevent PLWH from receiving needed services; – Information must be collected from multiple sources, among them PLWH and other community members, the health department, Medicaid agency, community-based providers and, where applicable, grantees of other CARE Act titles. Information must be obtained from and about HIV-positive individuals who know their status and are not in care. Assessment of unmet need and service gaps: – This should include an assessment of the unmet need for PLWH who know their HIV status but are not “in care” (unmet needs) and an assessment of service gaps for all PLWH—both in and out of care (service gaps); – This assessment should bring together the quantitative and qualitative data on service needs, resources, and barriers to help set priorities and allocate resources; Components of HRSA’s Framework for Comprehensive Needs Assessment
 and an assessment of service gaps for all PLWH—both in and out of care (service gaps); – This assessment should bring together the quantitative and qualitative data on service needs, resources, and barriers to help set priorities and allocate resources; Components of HRSA’s Framework for Comprehensive Needs Assessment.")
8
Updates of Components of the Comprehensive Needs Assessment Annual Updates: of Comprehensive Needs Assessment: – The comprehensive needs assessment need to be updated regularly – Certain aspects need to be updated annually; – Other aspects at least every 2 years; Timing of Updates of Each Component: – Integrated Epidemiologic Profile of HIV: Minor updates: Twice Yearly Major update: Every 2 years – Resource inventory: ?Every 1 – 2 Years? – Profile of provider capacity and capability: ?Every 1 – 2 Years? – Assessment of service needs among affected populations: ?Every 2 years? – Assessment of unmet need and service gaps: Annual Update; Comprehensive update: Every 2 years (reconciling unmet needs and service gaps)
.")
9
Basic Concepts: Unmet Needs, Primary Health Care, Primary Medical Care, and “In Care” HRSA/HAB defines unmet need as the need for HIV-related health services by individuals with HIV who are aware of their HIV status, but are not receiving regular primary health care; – Primary health care includes: *Primary Medical Care: Medical evaluation and clinical care that is consistent with Public Health Service guidelines, including CD4 cell monitoring, viral load testing, antiretroviral therapy, prophylaxis and treatment of opportunistic infections, malignancies, and other related conditions; ^Other Primary Health Care: –Oral health care –Outpatient mental health care –Outpatient substance abuse treatment –Nutritional services, and –Specialty medical care referrals. – The focus of assessment of unmet need is on need for HIV-related primary health care, more specifically Primary Medical Care;

10
The needs of individuals for other HIV-related services such as counseling and testing or case management is recognized; – Non-Medical Supportive Services: other services that facilitate a) access to/contribute to PLWH accessing primary medical care and b) remaining/retention in primary medical care; – By HRSA definition, the assessment of needs for these “non-primary health care” support services is referred to as assessment of service gaps (see next page); "In care” – means receiving primary medical care for HIV disease that is consistent with U.S. Public Health Service Treatment Guidelines. Persons who are accessing other health- related services and/or support services but are not receiving primary medical care are not considered to be "in care“. Hence, such persons are considered to “have unmet needs for primary medical care”. Basic Concepts: Unmet Needs, Primary Health Care, Primary Medical Care, and “In Care”

11
Service Gaps vs. Unmet Needs: Parts of Comprehensive Needs Assessment Service gaps: all service needs not currently being met for all PLWH except for the need for primary health care for individuals who know their status but are not in care; – includes additional need for primary health care for those already receiving primary medical care ("in care"); – also includes the need for supportive services for individuals not receiving primary medical care ("not in care"). The needs assessment will help the planning body set service priorities and advise the grantee about how best to meet those priorities: – Hence, your needs assessment will need to address not only the unmet need for primary health care but also other service needs—referred to as service gaps to distinguish them from unmet needs;
; – also includes the need for supportive services for individuals not receiving primary medical care ( not in care ). The needs assessment will help the planning body set service priorities and advise the grantee about how best to meet those priorities: – Hence, your needs assessment will need to address not only the unmet need for primary health care but also other service needs—referred to as service gaps to distinguish them from unmet needs;.")
12
Service Gaps vs. Unmet Needs: Parts of Comprehensive Needs Assessment Service gaps may occur because no services are currently available or because available services are either not appropriate for or not accessible to the target population. For example: – A service area that includes Latino PLWH with limited English proficiency but lacks Spanish-English bilingual case managers may have a service gap for bilingual case management services; – A rural service area that has a high incidence of injection drug use but lacks substance abuse services may have a lack of residential treatment facilities; Assessing unmet needs should be part of a coordinated overall comprehensive needs assessment process conducted in each jurisdiction: – Requires finding and determining the needs and service gaps of PLWH who are not receiving primary health care (Such individuals are likely to be members of traditionally underserved populations and may be among those with the greatest need for and dependence on CARE Act services) ;
 ;.")
13
Types of Needs Assessment Data Secondary source data: – Existing information that is primarily documented for a different purpose and obtained/abstracted and used secondarily for Epidemiologic purposes; viz. HIV Surveillance data; or Primary source data: – Information collected by the grantee, planning body, or applicant through such methods as surveys, interviews, and focus groups; Secondary and primary source data can be: – Quantitative: numerical information, such as epidemiologic data, and/or – Qualitative: descriptive or narrative information, such as focus group input.

14
Collaboration between Prevention & Care: Opportunities & Challenges Some components of Comprehensive Needs Assessment may be an Avenue for Collaboration between Prevention and Care Planning: – Preparation and presentation of an epidemiologic profile: Data on AIDS cases, HIV cases, and co-morbidities are of similar importance in both prevention and care planning. These data are typically compiled by the same State or local health department, which may find it more efficient to compile them once a year for both users Mutual accomodation is needed as data needs are not identical. – Preparation of a resource inventory: A resource inventory that catalogues available prevention and care services— including a description of services provided, clients served, and funding levels and sources—is needed by both prevention and care planners; Sharing of mailing lists can be the beginning of collaboration on such an inventory. A joint provider survey can be conducted to obtain data needed by either or both groups, with shared data analysis responsibility. The CARE Act planning body analyzes information needed only for care planning; the prevention group analyzes data needed only for prevention planning

15
Characteristics of a Comprehensive Needs Assessment Collective experience indicates that a sound needs assessment—a needs assessment that provides the information needed for priority setting, planning, and the design of service systems to address service gaps and unmet needs—typically has the following characteristics: – It is comprehensive, looking at a broad range of service categories, populations, and geographic areas. – It is broadly participatory, including input from population groups affected by the local epidemic—including individuals who know their HIV status but are not in care—and collaborates (where feasible) with other HIV/AIDS planning efforts. – It includes both quantitative and qualitative information. – It develops and follows a process that results in community acceptance of the outcome. – It is designed with specific "end uses and users" in mind. – It includes year-round efforts to identify and assess the service needs of individuals who know their HIV status but are not receiving primary health care.
 with other HIV/AIDS planning efforts. – It includes both quantitative and qualitative information. – It develops and follows a process that results in community acceptance of the outcome. – It is designed with specific end uses and users in mind. – It includes year-round efforts to identify and assess the service needs of individuals who know their HIV status but are not receiving primary health care..")
16
Importance/Rationale for Estimating Unmet Needs for Primary Health Care + 75% of HIV-infected Americans know their HIV status, ~ 650,000 (CDC) + 33% of the 650,000 who know their status (233,000) are not receiving HIV-related primary health care (I.e. they have HRSA-defined unmet needs); Analysis in PA shows that HIV continues to disproportionately affect historically underserved populations; Some people living with HIV (PLWH) populations are disproportionately less likely than others to be receiving primary health care (HRSA); HRSA guidelines call for getting more PLWH into primary care, particularly those who are disproportionately affected; Care Act Amendment of 2000 requirements include: – An assessment of the unmet needs of PLWH “who know their HIV status and are not receiving HIV-related services”, Particularly those from “disproportionately affected and historically underserved populations.” Care Act resources are to be kept “focused on early intervention and care delivery rather than expansion into prevention areas such as outreach to persons who do not know their HIV status; Targeting the needs of the “disproportionately affected and historically underserved populations” requires assessment of unmet need. Understanding the magnitude and determinants of unmet needs will enable public health program planners and implementing partners to craft strategies to address service barriers, deliver primary health care and also avail other support services that enable those in need to obtain and maintain primary care.
; Analysis in PA shows that HIV continues to disproportionately affect historically underserved populations; Some people living with HIV (PLWH) populations are disproportionately less likely than others to be receiving primary health care (HRSA); HRSA guidelines call for getting more PLWH into primary care, particularly those who are disproportionately affected; Care Act Amendment of 2000 requirements include: – An assessment of the unmet needs of PLWH who know their HIV status and are not receiving HIV-related services , Particularly those from disproportionately affected and historically underserved populations. Care Act resources are to be kept focused on early intervention and care delivery rather than expansion into prevention areas such as outreach to persons who do not know their HIV status; Targeting the needs of the disproportionately affected and historically underserved populations requires assessment of unmet need. Understanding the magnitude and determinants of unmet needs will enable public health program planners and implementing partners to craft strategies to address service barriers, deliver primary health care and also avail other support services that enable those in need to obtain and maintain primary care..")
17
Assessment of Unmet Need Within the Care Act Planning Process

18
Methodological Considerations in Estimating Unmet Needs Capacity: – Methodologically complicated process; requires capacity to collect needed data, integrate and use data from multiple data sources, combine quantitative and qualitative data, and translate information into understandable form for use in planning and priority setting; Data Limitations: – Availability and access limitations in relation to need for HIV reporting data; Limitations of surveillance data/databases; Lack of agreed-upon key questions and "core variables; Cross-title issues regarding data collection and data sharing; Lack of access to data from non-CARE Act sources/providers including other Federal agencies; need for client-level databases; Non-generalizable data; matching data from different databases; Confidentiality concerns; Use of Multiple Data Sets: Resource Limitations: – Financial and personnel resources; Limitations of surveys addressing unmet need; Burden of developing methodologies;

19
Intro to HRSA-Defined Framework for Measuring Unmet Need HRSA-recommended framework to estimate the number of individuals in service area who are aware of their HIV status (PLWH/aware) but not receiving HIV- related primary medical care; – Primary medical care is roughly equivalent to "medical evaluation and clinical care" in the HRSA definition of primary health care; Goal is to calculate how many PLWH/aware individuals in a particular area are "in" and "out" of primary medical care; Why HRSA framework focuses on PLWH/aware and not total PLWH (true HIV and AIDS prevalence): – A diagnosis of HIV must be made before receiving HIV primary medical care; – The CARE Act legislation requires grantees to focus on individuals who are aware of their status; Framework differentiates PLWH/aware into 2 main subsets: – PLWA(HIV+/AIDS)/aware – PLWH (HIV+/non-AIDS)/aware
 but not receiving HIV- related primary medical care; – Primary medical care is roughly equivalent to medical evaluation and clinical care in the HRSA definition of primary health care; Goal is to calculate how many PLWH/aware individuals in a particular area are in and out of primary medical care; Why HRSA framework focuses on PLWH/aware and not total PLWH (true HIV and AIDS prevalence): – A diagnosis of HIV must be made before receiving HIV primary medical care; – The CARE Act legislation requires grantees to focus on individuals who are aware of their status; Framework differentiates PLWH/aware into 2 main subsets: – PLWA(HIV+/AIDS)/aware – PLWH (HIV+/non-AIDS)/aware")
20
Definitions for Calculating Unmet Needs for HIV Primary Medical Care: Outcome Measures Unmet need for HIV primary medical care: – No evidence of any of the following three components of HIV primary medical care during a specified 12-month time frame: Viral Load (VL) Testing, CD4 Count, or Provision of Anti-Retroviral Therapy (ART). Met need for HIV primary medical care: – Demonstration of any one or more of the three measures during the specified 12-month time frame.

21
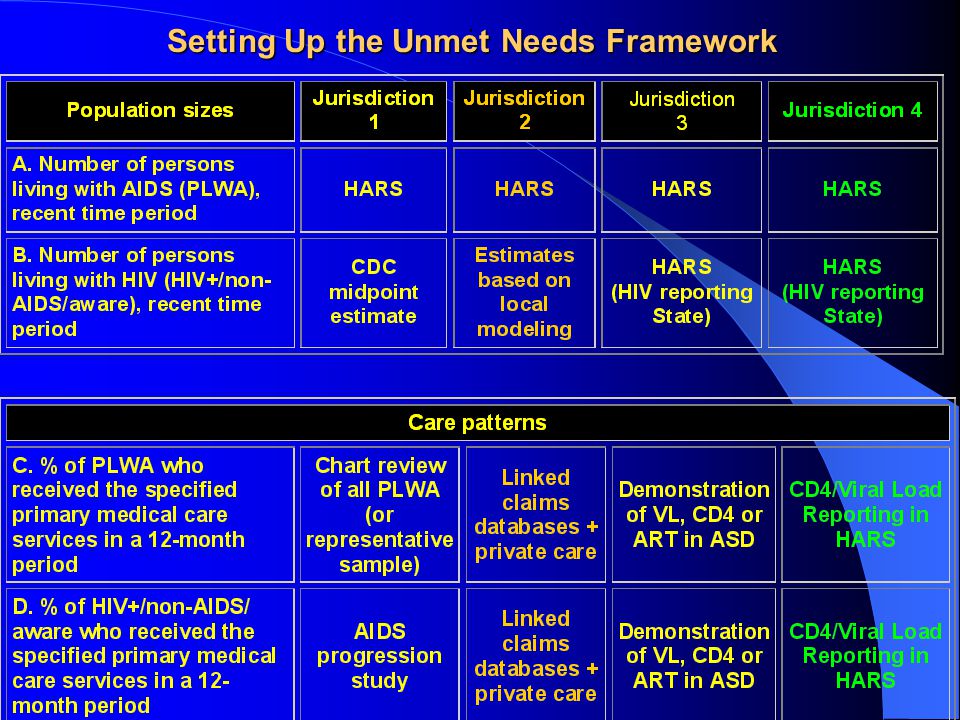
The Unmet Needs Framework: Data Needed 2 Primary Inputs for Unmet Needs Calculation => Care Input / Population Input Population Size Data Needed: # diagnosed with HIV in service area during time period => PLWH (AIDS AND NON-AIDS) => (A) # PLWA & (B) # PLWH HIV+/non-AIDS/aware) Care Patterns Data Needed: # receiving primary care from any provider => % PLWH (AIDS AND NON-AIDS) meeting primary care definition => (A) % PLWA meeting primary care definition & (B) % PLWH HIV+/non- AIDS/aware) meeting primary care definition
 => (A) # PLWA & (B) # PLWH HIV+/non-AIDS/aware) Care Patterns Data Needed: # receiving primary care from any provider => % PLWH (AIDS AND NON-AIDS) meeting primary care definition => (A) % PLWA meeting primary care definition & (B) % PLWH HIV+/non- AIDS/aware) meeting primary care definition")
22
Data Sources Number of People Living with AIDS (PLWA): <= AIDS Surveillance [State HIV/AIDS Reporting System (HARS)] Number of People Diagnosed and Living with HIV/non-AIDS (HIV+/non- AIDS/aware): <= HIV Surveillance [State HIV/AIDS Reporting System (HARS)] Percent or number of PLWH/aware (AIDS and non-AIDS) meeting primary medical care definition: – Surveillance data: – Linked utilization data: Linking billing or service information in various client-level databases, with the use of adequate measures to protect confidentiality (use of a non-identifying unique identifier or soundex code, e.g. –Combining data from CARE Act (ideally Titles I-IV), Medicaid, and Veterans Administration (VA) will cover the largest sources of HIV primary medical care. –Adjust for care received privately; – Special studies data: AIDS Spectrum of Disease (ASD) Supplemental HIV/AIDS Survey (SHAS), Other approaches
![Data Sources Number of People Living with AIDS (PLWA): <= AIDS Surveillance [State HIV/AIDS Reporting System (HARS)] Number of People Diagnosed and Living with HIV/non-AIDS (HIV+/non- AIDS/aware): <= HIV Surveillance [State HIV/AIDS Reporting System (HARS)] Percent or number of PLWH/aware (AIDS and non-AIDS) meeting primary medical care definition: – Surveillance data: – Linked utilization data: Linking billing or service information in various client-level databases, with the use of adequate measures to protect confidentiality (use of a non-identifying unique identifier or soundex code, e.g.](http://images.slideplayer.com/15/4792933/slides/slide_22.jpg "–Combining data from CARE Act (ideally Titles I-IV), Medicaid, and Veterans Administration (VA) will cover the largest sources of HIV primary medical care. –Adjust for care received privately; – Special studies data: AIDS Spectrum of Disease (ASD) Supplemental HIV/AIDS Survey (SHAS), Other approaches.")
23
All HIV+/aware eligible for Case Surveillance Cohort From Risk of Infection to Infection through Disease Progression: Order of Data Collection from Surveillance & Supplementary Sources (E+) HIV+ (E-) HIV+ Presence of Adverse Outcomes e.g: Unmet Needs; Poor Survival; or Deceased Absence of Adverse Outcome E.g. Met Needs; Better Survival; or Alive; Retrospective Lookback Prospective Follow-up HIV Diagnosis Disease Progression, AIDS, etc At Risk for HIV Adverse Outcome HIV Infection Retrospective review of Pre-Infection to Infection stage for “negatives”: Past exposures ascertained through lookback review of medical charts at time of entry into cohort (i.e. reported diagnoses of HIV/AIDS meeting CDC surveillance case definition); past exposures/ risk info may be supplemented through linkage studies with STD surveillance, case reports from confidential C&T, etc (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prospective follow-up of HIV+/aware persons, service data, intermediate disease progression and final outcomes assessed: Subjects followed through time, service data, intermediate and final outcomes assessed: “In Care” service indicator data collected in surveillance and other linkable service provider datasets; viz. Treatment, Adherence Case Management, etc. Intermediate outcomes/end-points are used to monitor disease progression with ongoing reports of laboratory test results of CD4, Viral Load (and Antiretroviral treatment) as indicators of disease progression or access/delivery of services; Potential outcome of death is ascertained through regular matching with the death registry
; past exposures/ risk info may be supplemented through linkage studies with STD surveillance, case reports from confidential C&T, etc (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prospective follow-up of HIV+/aware persons, service data, intermediate disease progression and final outcomes assessed: Subjects followed through time, service data, intermediate and final outcomes assessed: In Care service indicator data collected in surveillance and other linkable service provider datasets; viz. Treatment, Adherence Case Management, etc. Intermediate outcomes/end-points are used to monitor disease progression with ongoing reports of laboratory test results of CD4, Viral Load (and Antiretroviral treatment) as indicators of disease progression or access/delivery of services; Potential outcome of death is ascertained through regular matching with the death registry.")
24
Study subjects enter the cohort study at diagnosis (which may be at different calendar time points =~dynamic cohort) and are followed up through death, The Study cohort on this slide was derived from the Pennsylvania AIDS surveillance database and included all 12,804 adult AIDS cases diagnosed in PA before January 1995, The cohort was followed up through December 31, 1998, allowing for at least 48 months after the last diagnosis. Study Design II: A Conceptual Framework of the Dynamic Cohort Study Design and Study Population in the HIV/AIDS Reporting System

25
Another Perspective: The study subjects enter the cohort study at diagnosis through case report by physician, laboratory and ICD-9/lab data audits of provider reporting; Follow-up data on disease progression is monitored through ongoing reporting of lab test results and AIDS- defining illnesses derived from physician reports and matches with facility diagnostic codes in discharge summaries and other data sources; Cases are followed up through death which is ascertained through matches with the death registry; All prevalent HIV infections { Death Study Design III: A Conceptual Framework of the Dynamic Cohort Study Design and Study Population in the HIV/AIDS Reporting System

26
Setting Up the Unmet Needs Framework

28
Calculating Unmet Needs Estimates w/out HIV Reporting Data Pop Inputs Care Inputs Calculations ANALYSES RESULTS FOR DEMONSTRATION ONLY

29
Calculating Unmet Needs Estimates w/out HIV Reporting Data Pop Inputs Care Inputs Calculations ANALYSES RESULTS FOR DEMONSTRATION ONLY

30
Calculating Unmet Needs Estimates w/out HIV Reporting Data Pop Inputs Care Inputs Calculations ANALYSES RESULTS FOR DEMONSTRATION ONLY

31
Calculating Unmet Needs Estimates in Area w/HIV Reporting PRELIM. ANALYSES RESULTS FOR DEMONSTRATION ONLY Pop Inputs Care Inputs Calculations

32
Calculating Unmet Needs Estimates in Area w/HIV Reporting PRELIM. ANALYSES RESULTS FOR DEMONSTRATION ONLY Pop Inputs Care Inputs Calculations

33
Calculating Unmet Needs Estimates in Area w/HIV Reporting PRELIM. ANALYSES RESULTS FOR DEMONSTRATION ONLY Pop Inputs Care Inputs Calculations

34
Integrating the Unmet Needs Framework with Other Needs Assessment Analyses and Activities Further analyses needed in addition to calculating how many PLWH who know their status are not receiving HIV-related primary medical care: – Describe who these people are and where they are. The planning body can consider what can be done in the State or locality to improve primary care access. Data needed to estimate the number of PLWH who not receiving primary medical care generally also allow sub-analyses: – By characteristics of people with unmet needs in terms of gender, race/ethnicity, and other important sociodemographic characteristics; – Some population and care data can also be analyzed for smaller geographic areas, such as counties, regions, or Public Health Service Areas, allowing for better targeting of resources and activities; – To assess the relationship between service gaps and unmet needs, correlation analyses of the relationship between unmet needs and ecological variables such as levels of service gaps may also identify larger contextual forces that may be associated with aggregate measures of indicators of unmet need;

35
Adapted from Katz MH et al. Ann Intern Med. 2001 Oct 16;135(8 Pt 1):557-65. RESULTS: At baseline, 56.5% of the sample studied had contact with a case manager in the previous 6 months. In multiple logistic regression analyses that adjusted for potential confounders, contact with a case manager at baseline was associated with decreased unmet need for income assistance (odds ratio [OR], 0.57 [95% CI, 0.36 to 0.91]), health insurance (OR, 0.54 [CI, 0.33 to 0.89]), home health care (OR, 0.29 [CI, 0.15 to 0.56]), and emotional counseling (OR, 0.62 [CI, 0.41 to 0.94]) at follow-up. Contact with case managers was not significantly associated with utilization of ambulatory care (OR, 0.77 [CI, 0.57 to 1.04]), hospitalization (OR, 1.13 [CI, 0.84 to 1.54]), or emergency department visits (OR, 1.30 [CI, 0.97 to 1.73]) but was associated with higher utilization of two-drug (OR, 1.58 [CI, 1.23 to 2.03]) and three-drug (OR, 1.34 [CI, 1.00 to 1.80]) antiretroviral regimens and of treatment with protease inhibitors or non-nucleoside reverse transcriptase inhibitors (OR, 1.29 [CI, 1.02 to 1.64]) at follow-up. CONCLUSIONS: Case management appears to be associated with fewer unmet needs and higher use of HIV medications in patients receiving HIV treatment. Findings of Investigations of Effect of HIV Case Management on Unmet Needs for Primary Medical Care
, health insurance (OR, 0.54 [CI, 0.33 to 0.89]), home health care (OR, 0.29 [CI, 0.15 to 0.56]), and emotional counseling (OR, 0.62 [CI, 0.41 to 0.94]) at follow-up. Contact with case managers was not significantly associated with utilization of ambulatory care (OR, 0.77 [CI, 0.57 to 1.04]), hospitalization (OR, 1.13 [CI, 0.84 to 1.54]), or emergency department visits (OR, 1.30 [CI, 0.97 to 1.73]) but was associated with higher utilization of two-drug (OR, 1.58 [CI, 1.23 to 2.03]) and three-drug (OR, 1.34 [CI, 1.00 to 1.80]) antiretroviral regimens and of treatment with protease inhibitors or non-nucleoside reverse transcriptase inhibitors (OR, 1.29 [CI, 1.02 to 1.64]) at follow-up. CONCLUSIONS: Case management appears to be associated with fewer unmet needs and higher use of HIV medications in patients receiving HIV treatment. Findings of Investigations of Effect of HIV Case Management on Unmet Needs for Primary Medical Care.")
37
EPIDEMIOLOGY OF HIV/AIDS IN PENNSYLVANIA Module 2 *Epidemiology Methods: Conceptualization, Design, Conduct and Outcome Evaluation of Response Plans & Intervention Programs (to address unmet needs) Benjamin Richard H. Muthambi, DrPH, MPH State HIV/AIDS Epidemiologist

38
Key Steps in the Conceptualization, Design, Conduct and Outcome Evaluation of Response Plans & Intervention Programs Review Sources of Summary Information on Potential Risk-Factors and Outcomes in Comprehensive Unmet Needs Assessment Conceptualize Response Plans & Intervention Programs to Address Unmet Needs; (incorporating other components of the comprehensive assessment of unmet needs); Design Response Plans & Intervention Programs/Practice Protocols to Address Unmet Needs Conduct/Implement Response Plans & Intervention Program/Practice Protocols to Address Unmet Needs; Outcome Evaluation of Response Plans & Intervention Program/Practice Protocols to Address Unmet Needs;
; Design Response Plans & Intervention Programs/Practice Protocols to Address Unmet Needs Conduct/Implement Response Plans & Intervention Program/Practice Protocols to Address Unmet Needs; Outcome Evaluation of Response Plans & Intervention Program/Practice Protocols to Address Unmet Needs;")
39
Development and Evaluation of Response Plans & Intervention Programs Review the comprehensive needs assessment and identify data-driven findings and recommended public health actions as a basis for a series of program plans to address each recommendation; Prioritize risk factors based on findings of relative importance of risk factors identified in multivariate analyses of comprehensive unmet need data: a key factor in such prioritization is the projected potential for preventing unmet needs (based on the concept of “attributable risk”, “prevented fraction” is the proportion of unmet needs that would be prevented by eliminating or reducing a given risk factor or determinant);
;")
40
Sources of Summary Information on Potential Risk-Factors and Outcomes in Comprehensive Unmet Needs Assessment Integrated Epidemiologic Profile of HIV: – Describes the current status of the epidemic in the service area: of greater relevance to care, specifically describe the prevalence (burden of disease) of HIV and AIDS overall and among defined subpopulations; Assessment of service needs among affected populations: – Includes barriers that prevent PLWH from receiving needed services; – Information must be collected from multiple sources, among them PLWH and other community members, the health department, Medicaid agency, community-based providers and, where applicable, grantees of other CARE Act titles. Information must be obtained from and about HIV-positive individuals who know their status and are not in care. Resource inventory: – Describes organizations and individuals providing services across the full spectrum of HIV services accessible to PLWH in the service area, regardless of funding source. Profile of provider capacity and capability: – Identifies the extent to which services identified in the resource inventory are accessible, available, and appropriate for PLWH, including specific subpopulations; Describe Capacity: how much of which services a provider can deliver ; Describe Capability: the degree to which a provider is actually accessible and has the needed expertise to provide services ; Assessment of barriers to PLWH receiving services is an important aspect of this component (i.e., the profile should inquire from PLWH directly or service providers the barriers faced in accessing services); Provider profiles may also explore client perceptions of service quality and appropriateness: assessment of client satisfaction is a complex effort that should be undertaken thoroughly in the planning body's quality improvement process. Assessment of unmet need and service gaps: – This should include an assessment of the unmet need for PLWH who know their HIV status but are not in care and an assessment of service gaps for all PLWH—both in and out of care; – This assessment should bring together the quantitative and qualitative data on service needs, resources, and barriers to help set priorities and allocate resources; – Gap analyses are used to correlate services, morbidity, unmet needs, etc Annual Updates: Certain components of the needs assessment should be expanded and/or updated, depending on trends and special issues facing the State, EMA, or other service area.
; Provider profiles may also explore client perceptions of service quality and appropriateness: assessment of client satisfaction is a complex effort that should be undertaken thoroughly in the planning body s quality improvement process. Assessment of unmet need and service gaps: – This should include an assessment of the unmet need for PLWH who know their HIV status but are not in care and an assessment of service gaps for all PLWH—both in and out of care; – This assessment should bring together the quantitative and qualitative data on service needs, resources, and barriers to help set priorities and allocate resources; – Gap analyses are used to correlate services, morbidity, unmet needs, etc Annual Updates: Certain components of the needs assessment should be expanded and/or updated, depending on trends and special issues facing the State, EMA, or other service area..")
41
Adapted from Katz MH et al. Ann Intern Med. 2001 Oct 16;135(8 Pt 1):557-65. RESULTS: At baseline, 56.5% of the sample studied had contact with a case manager in the previous 6 months. In multiple logistic regression analyses that adjusted for potential confounders, contact with a case manager at baseline was associated with decreased unmet need for income assistance (odds ratio [OR], 0.57 [95% CI, 0.36 to 0.91]), health insurance (OR, 0.54 [CI, 0.33 to 0.89]), home health care (OR, 0.29 [CI, 0.15 to 0.56]), and emotional counseling (OR, 0.62 [CI, 0.41 to 0.94]) at follow-up. Contact with case managers was not significantly associated with utilization of ambulatory care (OR, 0.77 [CI, 0.57 to 1.04]), hospitalization (OR, 1.13 [CI, 0.84 to 1.54]), or emergency department visits (OR, 1.30 [CI, 0.97 to 1.73]) but was associated with higher utilization of two-drug (OR, 1.58 [CI, 1.23 to 2.03]) and three-drug (OR, 1.34 [CI, 1.00 to 1.80]) antiretroviral regimens and of treatment with protease inhibitors or non-nucleoside reverse transcriptase inhibitors (OR, 1.29 [CI, 1.02 to 1.64]) at follow-up. CONCLUSIONS: Case management appears to be associated with fewer unmet needs and higher use of HIV medications in patients receiving HIV treatment. Findings of Comprehensive Investigations of Effect of HIV Case Management as a Predictor of Unmet Needs for Primary Medical Care
, health insurance (OR, 0.54 [CI, 0.33 to 0.89]), home health care (OR, 0.29 [CI, 0.15 to 0.56]), and emotional counseling (OR, 0.62 [CI, 0.41 to 0.94]) at follow-up. Contact with case managers was not significantly associated with utilization of ambulatory care (OR, 0.77 [CI, 0.57 to 1.04]), hospitalization (OR, 1.13 [CI, 0.84 to 1.54]), or emergency department visits (OR, 1.30 [CI, 0.97 to 1.73]) but was associated with higher utilization of two-drug (OR, 1.58 [CI, 1.23 to 2.03]) and three-drug (OR, 1.34 [CI, 1.00 to 1.80]) antiretroviral regimens and of treatment with protease inhibitors or non-nucleoside reverse transcriptase inhibitors (OR, 1.29 [CI, 1.02 to 1.64]) at follow-up. CONCLUSIONS: Case management appears to be associated with fewer unmet needs and higher use of HIV medications in patients receiving HIV treatment. Findings of Comprehensive Investigations of Effect of HIV Case Management as a Predictor of Unmet Needs for Primary Medical Care.")
42
All HIV+/aware eligible for Case Surveillance Cohort From Risk of Infection to Infection through Disease Progression : Predictors/Determinants/Risk Factors of Unmet Need (E+) HIV+ (E-) HIV+ Presence of Adverse Outcomes e.g: Unmet Needs; Poor Survival; or Deceased Absence of Adverse Outcome E.g. Met Needs; Better Survival; or Alive; Retrospective Lookback Prospective Follow-up HIV Diagnosis Disease Progression, AIDS, etc At Risk for HIV Adverse Outcome HIV Infection Predictors/Determinants/Risk Factors of Unmet Need: Demographic, Socioeconomic & other factors; Referral & Linkage to Primary Medical Care to prevent & monitor progression; “In Care Indicators”: Rx, CD4+, VL Outreach/”Marketing” of care to HIV+/aware not in care & referral to care; Adherence Case Management; Other Support Services; (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prioritize risk factors based on findings of relative importance of risk factors identified in multivariate analyses of comprehensive unmet need data: a key factor in such prioritization is the projected potential for preventing unmet needs (based on the concept of “attributable risk”, “prevented fraction” is the proportion of unmet needs that would be prevented by eliminating or reducing a given risk factor or determinant);
 Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prioritize risk factors based on findings of relative importance of risk factors identified in multivariate analyses of comprehensive unmet need data: a key factor in such prioritization is the projected potential for preventing unmet needs (based on the concept of attributable risk , prevented fraction is the proportion of unmet needs that would be prevented by eliminating or reducing a given risk factor or determinant);.")
43
Development and Evaluation of Response Plans & Intervention Programs Review the comprehensive needs assessment and identify data-driven findings and recommended public health actions as a basis for a series of program plans to address each recommendation; Prioritize risk factors based on findings of relative importance of risk factors identified in multivariate analyses of comprehensive unmet need data: a key factor in such prioritization is the projected potential for preventing unmet needs (based on the concept of “attributable risk”, “prevented fraction” is the proportion of unmet needs that would be prevented by eliminating or reducing a given risk factor or determinant); Conceptualize response programs to be used to target and decrease the identified influential/key risk factors of unmet need in affected communities; Develop and/or implement response program protocols targeting the identified key risk factors or indicators of unmet need in affected communities and systematically embed measurement and documentation of relevant outcome indicators during program implementation;
; Conceptualize response programs to be used to target and decrease the identified influential/key risk factors of unmet need in affected communities; Develop and/or implement response program protocols targeting the identified key risk factors or indicators of unmet need in affected communities and systematically embed measurement and documentation of relevant outcome indicators during program implementation;")
44
All HIV+/aware eligible for Case Surveillance Cohort From Risk of Infection to Infection through Disease Progression : Framework of Opportunities/Avenues for Prevention and Care Services (E+) HIV+ (E-) HIV+ Presence of Adverse Outcomes e.g: Unmet Needs; Poor Survival; or Deceased Absence of Adverse Outcome E.g. Met Needs; Better Survival; or Alive; Retrospective Lookback Prospective Follow-up HIV Diagnosis Disease Progression, AIDS, etc At Risk for HIV Adverse Outcome HIV Infection Primary Prevention for “negatives”: Outreach; C & T; PCRS; PCM; etc… Prevention for “Positives”: HIV+/aware likely to Transmit HIV; Outreach & risk assessment; Ongoing PCRS; Prevention Case Management; etc… (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Primary Prevention: Prophylaxis for PCP, TB, etc. Secondary Prevention: Referral & Linkage to Primary Medical Care to prevent & monitor progression; Rx, CD4+, VL Outreach/”Marketing” to HIV+/aware not in care & referral to care; Adherence Case Management; Other Support Services;
 Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Primary Prevention: Prophylaxis for PCP, TB, etc. Secondary Prevention: Referral & Linkage to Primary Medical Care to prevent & monitor progression; Rx, CD4+, VL Outreach/ Marketing to HIV+/aware not in care & referral to care; Adherence Case Management; Other Support Services;.")
45
All HIV+/aware eligible for Case Surveillance Cohort From Risk of Infection to Disease Progression: Focus on Opportunities/Avenues for Care Services (E+) HIV+ (E-) HIV+ Presence of Adverse Outcomes e.g: Unmet Needs; Poor Survival; or Deceased Absence of Adverse Outcome E.g. Met Needs; Better Survival; or Alive; Retrospective Lookback Prospective Follow-up HIV Diagnosis Disease Progression, AIDS, etc At Risk for HIV Post Intervention Outcome Measurement HIV Infection Primary Prevention for “negatives”: Outreach; C & T; PCRS; PCM; etc… Primary Prevention: Prophylaxis for PCP, TB, etc. Secondary Prevention Interventions: Referral & Linkage to Primary Medical Care to prevent & monitor progression: -Rx, CD4+, VL Outreach/”Marketing” to HIV+/aware not in care & referral to care; Adherence Case Management; Other Support Services: housing, etc Prevention for “Positives”: HIV+/aware likely To transmit; Outreach; Ongoing PCRS; Prevention Case Management,etc (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; à2 o Interventions à2 o Interventions Pre-Intervention Measurement
 Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; à2 o Interventions à2 o Interventions Pre-Intervention Measurement.")
46
Development and Evaluation of Response Plans & Intervention Programs Review the comprehensive needs assessment and identify data-driven findings and recommended public health actions as a basis for a series of program plans to address each recommendation; Prioritize risk factors based on findings of relative importance of risk factors identified in multivariate analyses of comprehensive unmet need data: a key factor in such prioritization is the projected potential for preventing unmet needs (based on the concept of “attributable risk”, “prevented fraction” is the proportion of unmet needs that would be prevented by eliminating or reducing a given risk factor or determinant); Conceptualize response programs to be used to target and decrease the identified influential/key risk factors of unmet need in affected communities; Develop and/or implement response program protocols targeting the identified key risk factors or indicators of unmet need in affected communities and systematically embed measurement and documentation of relevant outcome indicators during program implementation; To determine the impact/outcomes of response programs, conduct outcome evaluations in progressive stages; and repeat service gap analyses : – Assess the reduction in risk factors targeted by response programs, e.g. targeting a risk factor/determinant/predictor variable of unmet needs such as “lack of case management” through redirecting adherence case management resources and outreach to/linkage of those with unmet need may increase intermediate outcomes such as the number of persons under adherence case management; – Assess changes in outcomes in unmet needs such as retention in primary medical care and adherence to medications; – Evaluate the relationship between changes in unmet needs, levels of bio-markers of health status and long-term outcomes such as survival in which response programs are implemented; Assess change by comparing pre- and post- intervention levels of outcome measures and service gaps;

47
All HIV+/aware eligible for Case Surveillance Cohort From Risk of Infection to Infection through Disease Progression : Order of Data Collection from Surveillance & Supplementary Sources (E+) HIV+ (E-) HIV+ Presence of Adverse Outcomes e.g: Unmet Needs; Poor Survival; or Deceased Absence of Adverse Outcome E.g. Met Needs; Better Survival; or Alive; Retrospective Lookback Prospective Follow-up HIV Diagnosis Disease Progression, AIDS, etc At Risk for HIV Adverse Outcome HIV Infection Retrospective review of Pre-Infection to Infection stage for “negatives”: Past exposures ascertained through look back review of medical charts at time of entry into cohort (i.e. reported diagnoses of HIV/AIDS meeting CDC surveillance case definition); past exposures/ risk info may be supplemented through linkage studies with STD surveillance, case reports from confidential C&T, etc (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prospective follow-up of HIV+/aware persons, service data, intermediate disease progression and final outcomes assessed: PLWH (HIV+/aware) followed through time, service data, intermediate and final outcomes assessed: “In Care” service indicator data collected in surveillance and other linkable service provider datasets; e.g. Treatment, Adherence Case Management, etc. Intermediate outcomes/end-points/indicators of “being in care” for monitoring disease progression: ongoing reports of laboratory test results of CD4, Viral Load (and Antiretroviral treatment) as indicators of disease progression or access/delivery of services; Potential outcome of death is ascertained through regular death matching
; past exposures/ risk info may be supplemented through linkage studies with STD surveillance, case reports from confidential C&T, etc (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prospective follow-up of HIV+/aware persons, service data, intermediate disease progression and final outcomes assessed: PLWH (HIV+/aware) followed through time, service data, intermediate and final outcomes assessed: In Care service indicator data collected in surveillance and other linkable service provider datasets; e.g. Treatment, Adherence Case Management, etc. Intermediate outcomes/end-points/indicators of being in care for monitoring disease progression: ongoing reports of laboratory test results of CD4, Viral Load (and Antiretroviral treatment) as indicators of disease progression or access/delivery of services; Potential outcome of death is ascertained through regular death matching.")
48
All HIV+/aware eligible for Case Surveillance Cohort From Risk of Infection to Infection through Disease Progression : From Risk of Infection to Infection through Disease Progression : Comprehensive Evaluation of Outcomes through Surveillance & Supplementary Sources (E+) HIV+ (E-) HIV+ Presence of Adverse Outcomes e.g: Unmet Needs; Poor Survival; or Deceased Absence of Adverse Outcome E.g. Met Needs; Better Survival; or Alive; Retrospective Lookback Prospective Follow-up HIV Diagnosis Disease Progression, AIDS, etc At Risk for HIV Adverse Outcome HIV Infection (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prospective follow-up of HIV+/aware persons, service data, intermediate disease progression and final outcomes assessed: To determine the impact/outcomes of response programs, conduct comprehensive outcome evaluations in progressive stages; and repeat service gap analyses : – Assess change/likelihood of reduction in risk factors targeted by response programs, e.g. targeting a risk factor/determinant/predictor variable of unmet needs such as “lack of case management” through redirecting adherence case management resources and outreach to/linkage of those with unmet need may increase intermediate outcomes such as the number of persons under adherence case management; – Assess changes in outcomes in unmet needs such as retention in primary medical care and adherence to medications; – Evaluate the relationship between changes in unmet needs, levels of bio-markers of health status and long-term outcomes such as survival in which response programs are implemented; Assess change by comparing pre- and post- intervention levels of outcome measures and service gaps;
 Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; Prospective follow-up of HIV+/aware persons, service data, intermediate disease progression and final outcomes assessed: To determine the impact/outcomes of response programs, conduct comprehensive outcome evaluations in progressive stages; and repeat service gap analyses : – Assess change/likelihood of reduction in risk factors targeted by response programs, e.g. targeting a risk factor/determinant/predictor variable of unmet needs such as lack of case management through redirecting adherence case management resources and outreach to/linkage of those with unmet need may increase intermediate outcomes such as the number of persons under adherence case management; – Assess changes in outcomes in unmet needs such as retention in primary medical care and adherence to medications; – Evaluate the relationship between changes in unmet needs, levels of bio-markers of health status and long-term outcomes such as survival in which response programs are implemented; Assess change by comparing pre- and post- intervention levels of outcome measures and service gaps;.")
49
Development and Evaluation of Response Plans & Intervention Programs Review the comprehensive needs assessment and identify data-driven findings and recommended public health actions as a basis for a series of program plans to address each recommendation; Prioritize risk factors based on findings of relative importance of risk factors identified in multivariate analyses of comprehensive unmet need data: a key factor in such prioritization is the projected potential for preventing unmet needs (based on the concept of “attributable risk”, “prevented fraction” is the proportion of unmet needs that would be prevented by eliminating or reducing a given risk factor or determinant); Conceptualize response programs to be used to target and decrease the identified influential/key risk factors of unmet need in affected communities; Develop and/or implement response program protocols targeting the identified key risk factors or indicators of unmet need in affected communities and systematically embed measurement and documentation of relevant outcome indicators during program implementation; To determine the impact/outcomes of response programs, conduct outcome evaluations in progressive stages; and repeat service gap analyses : – Assess change/likelihood of reduction in risk factors targeted by response programs, e.g. targeting a risk factor/determinant/predictor variable of unmet needs such as “lack of case management” through redirecting adherence case management resources and outreach to/linkage of those with unmet need may increase intermediate outcomes such as the number of persons under adherence case management; – Assess changes in outcomes in unmet needs such as retention in primary medical care and adherence to medications; – Evaluate the relationship between changes in unmet needs, levels of bio-markers of health status and long-term outcomes such as survival in which response programs are implemented; Assess change by comparing pre- and post- intervention levels of outcome measures and service gaps;

51
Outline for Module 3: Introduction to Applied HIV Epidemiology Collaboration Mechanisms Outline for Module 3: Introduction to Applied HIV Epidemiology Collaboration Mechanisms Addressing Unmet Needs at the Agency Level through Commissioned & Mentored In- Service Learning Projects Logistical Considerations for Design, Conduct and Comparative Evaluation of Competing Models for Linkage of Epidemiologic Case Surveillance to Intervention Activities;

52
Introduction to Applied HIV Epidemiology Collaboration Mechanisms Introduction to Applied HIV Epidemiology Collaboration Mechanisms Addressing Unmet Needs at the Agency Level through Commissioned & Mentored In- Service Learning Projects Applied HIV Epidemiology Collaboration Mechanisms for Local or Community-Based Research: Applied HIV Epidemiology Collaboration Mechanisms for Local or Community-Based Research: – Commissioned Projects; – Commissioned Mentored In-Service Learning Projects – What are the aspects of the project which may require technical support?

53
All HIV+/aware eligible for Case Surveillance Cohort From Risk of Infection to Disease Progression: Focus on Opportunities/Avenues for Care Services (E+) HIV+ (E-) HIV+ Presence of Adverse Outcomes e.g: Unmet Needs; Poor Survival; or Deceased Absence of Adverse Outcome E.g. Met Needs; Better Survival; or Alive; Retrospective Lookback Prospective Follow-up HIV Diagnosis Disease Progression, AIDS, etc At Risk for HIV Post Intervention Outcome Measurement HIV Infection Primary Prevention for “negatives”: Outreach; C & T; PCRS; PCM; etc… Primary Prevention: Prophylaxis for PCP, TB, etc. Secondary Prevention Interventions: Referral & Linkage to Primary Medical Care to prevent & monitor progression: -Rx, CD4+, VL Outreach/”Marketing” to HIV+/aware not in care & referral to care; Adherence Case Management; Other Support Services: housing, etc Prevention for “Positives”: HIV+/aware likely To transmit; Outreach; Ongoing PCRS; Prevention Case Management,etc (E+) Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; à2 o Interventions à2 o Interventions Pre-Intervention Measurement
 Certain Pre-infection Exposures Present; (E-) Certain Pre-infection Exposures Not Present; à2 o Interventions à2 o Interventions Pre-Intervention Measurement.")
54
Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care Establish Common Aims & Objectives (preferably, Applicable to All Participating Sites): Establish Common Aims & Objectives (preferably, Applicable to All Participating Sites): – The purpose of the study is to: To develop and implement and evaluate response plans to unmet needs assessment for primary medical care;
: Establish Common Aims & Objectives (preferably, Applicable to All Participating Sites): – The purpose of the study is to: To develop and implement and evaluate response plans to unmet needs assessment for primary medical care;")
55
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: Selecting potential study sites; Selecting common study design; Determine standard predictor and outcome variables to be measured; Establishing comparable study procedures; –Measurement Procedures: –Intervention Procedures: –Analyses Procedures: Defining common approaches for interpreting, sharing and publishing results and for translating findings into public health action to improve services; Develop standard study protocol; Seek Funding for Study; Obtain IRB review, if required; Implement Study, if funded; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care

56
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: A) Selecting potential study sites: –a site may be a local health Department or individual facilities; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 Selecting potential study sites: –a site may be a local health Department or individual facilities; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care")
57
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: B) Selecting common study design: –e.g. Non-Randomized Community Intervention Trial; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care

58
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: C) Determine standard predictor and outcome variables to be measured; –What variables can we consider measuring? Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care

59
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: D) Establish comparable study procedures; –a) Measurement Procedures: Define pre- and post-intervention measures of predictor and outcome variables [e.g. no of contacts generated from each index HIV+ individual per PCRS encounter; eligibility criteria for each intervention type; success of linkage to prevention, care or support services (e.g. linkage to PCRS or case management); CD4; VL; etc]. Measure pre-intervention levels of predictor and outcome variables; Measure post-intervention levels of predictor and outcome variables; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
; CD4; VL; etc]. Measure pre-intervention levels of predictor and outcome variables; Measure post-intervention levels of predictor and outcome variables; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care.")
60
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: D) Establish comparable study procedures; –b) Intervention Procedures: Develop public health intervention/practice protocols to be implemented across sites; Implement public health intervention/practice protocols in each site synchronously (most preferable); Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 Establish comparable study procedures; –b) Intervention Procedures: Develop public health intervention/practice protocols to be implemented across sites; Implement public health intervention/practice protocols in each site synchronously (most preferable); Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care")
61
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: D) Establish comparable study procedures; –c) Analyses Procedures: Define relationships to be analyzed: e.g. r/ship of # successful linkages to case management or county of residence vs. median # cases with unmet need for primary medical care (CD4 or VL or Rx) in a given 12 month period); Perform analyses of within and across-site comparisons of pre- and post-intervention rates of successful linkage to respective interventions such as case management (analyses of covariance); Perform analyses of within and across site comparisons of pre- and post intervention levels of outcome measures such as unmet needs; indicators of implementation of PHS guidelines; median CD4 cell counts; Viral Load; etc (analyses of covariance); Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 in a given 12 month period); Perform analyses of within and across-site comparisons of pre- and post-intervention rates of successful linkage to respective interventions such as case management (analyses of covariance); Perform analyses of within and across site comparisons of pre- and post intervention levels of outcome measures such as unmet needs; indicators of implementation of PHS guidelines; median CD4 cell counts; Viral Load; etc (analyses of covariance); Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care.")
62
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: E) Define common approach for interpreting results and for translating findings into public health action to improve services; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 Define common approach for interpreting results and for translating findings into public health action to improve services; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care")
63
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: F) Develop standard study protocol; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 Develop standard study protocol; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care")
64
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: G) Seek Funding for Study; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 Seek Funding for Study; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care")
65
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: H) Obtain IRB review, if required; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 Obtain IRB review, if required; Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care")
66
Establish Common Methods Applicable to All Participating Sites: Establish Common Methods Applicable to All Participating Sites: – This must include: I) Implement Study, if funded; (how & who?); Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care
 Implement Study, if funded; (how & who ); Design, Conduct Implementation and Evaluation of Response Plans to Unmet Needs Assessment for Primary Medical Care")
Similar presentations





>")















