Download presentation
Presentation is loading. Please wait.

2
EXTRAPULMONARY TUBERCULOSIS
HamidReza Naderi MD Department of Infectious Diseases Mashhad University of Medical Sciences

3
Extrapulmonary TB, like pulmonary TB, is the result of infection with organisms of the Mycobacterium tuberculosis complex, which include M. tuberculosis, Mycobacterium bovis or Mycobacterium africanum. Extrapulmonary TB is defined as disease involving structures other than lung parenchyma and is less common than pulmonary TB.

4
Extrapulmonary tuberculous disease occurs as result of contiguous spread of tubercle organisms to adjoining structures, such as pleura or pericardium, or by lymphohaematogenous spread during primary or chronic infection. According to the World Health Organization (WHO) patients who are sputum smear-positive and also present with extrapulmonary tuberculous disease manifestations are categorized as pulmonary TB.
 patients who are sputum smear-positive and also present with extrapulmonary tuberculous disease manifestations are categorized as pulmonary TB.")
5
Extrapulmonary TB may occur in multiple sites, with relative frequencies of 42% for lymphatic, 18% for pleural, 12% for bone or joint, 6% for genitourinary, 6% for meningeal, 5% for peritoneal, and 11% for other sites. The lymph nodes are the most common site of extrapulmonary TB for both otherwise normal and HIV-infected patients. Involvement of the meninges is more common in young children than in other age groups (present in approximately 4% of children with TB), and the incidence of TB in the remainder of the extrapulmonary sites increases with age.
, and the incidence of TB in the remainder of the extrapulmonary sites increases with age.")
6
Lymphadenitis Tuberculous lymphadenitis (scrofula) is the most common form of extrapulmonary TB. The diagnosis of scrofula usually is made by fine needle aspiration of an affected lymph node. Although AFB smears are positive in only approximately 20% of cases, granulomatous inflammation may be obvious. Overall, fine needle aspiration has a sensitivity of 77% and specificity of 93% for TB infection.

9
Pleural Effusion Pleural extrapulmonary TB may occur early after primary infection with MTB and manifest as pleurisy with effusion, or more rarely, it may occur late in postprimary cavitary disease and arise as an empyema. Tuberculous pleural involvement often causes no symptoms and resolves spontaneously; however, in untreated patients, a 65% relapse rate has been reported, with development of active pulmonary or extrapulmonary TB within 5 years.

10
The diagnosis usually is confirmed by microscopic and chemical examination of pleural fluid or pleural biopsy. White blood cell counts usually range from 500 to 2500 cells/mL. The fluid is an exudate with protein usually exceeding 50% of the serum protein, and the glucose may be normal to low. Because there are few bacilli, AFB smears rarely are positive, and cultures grow MTB for only 25 to 30% of patients. Pleural biopsy can confirm the diagnosis in .approximately 75% of patients

12
Bone and Joint Infection Bone and joint TB remains a disease of older children and young adults in developing countries. Skeletal TB presumably develops from reactivation of dormant tubercles originally seeded during stage 2 of the primary infection or, in the case of spinal TB, from contiguous spread from paravertebral lymph nodes to the vertebrae. Generally, spinal TB (Pott's disease) accounts for 50 to 70% of the reported cases; the hip or knee is involved in 15 to 20% of cases, and the ankle, elbow, wrists, shoulders, and other bones and joints account for 15 to 20% of cases.
 accounts for 50 to 70% of the reported cases; the hip or knee is involved in 15 to 20% of cases, and the ankle, elbow, wrists, shoulders, and other bones and joints account for 15 to 20% of cases..")
13
Paraspinal “cold” abscesses develop in 50% or more of cases, with occasional formation of sinus tracts. The so-called skip lesions can easily be missed in imaging the spine for Pott's disease. The main complication of Pott's disease is spinal cord compression. Medical management includes chemotherapy, modified bedrest, and early ambulation and results in improvement in approximately 90% of patients without neurologic involvement. Surgical treatment usually is reserved for patients with neurologic complications.

15
Central Nervous System Disease
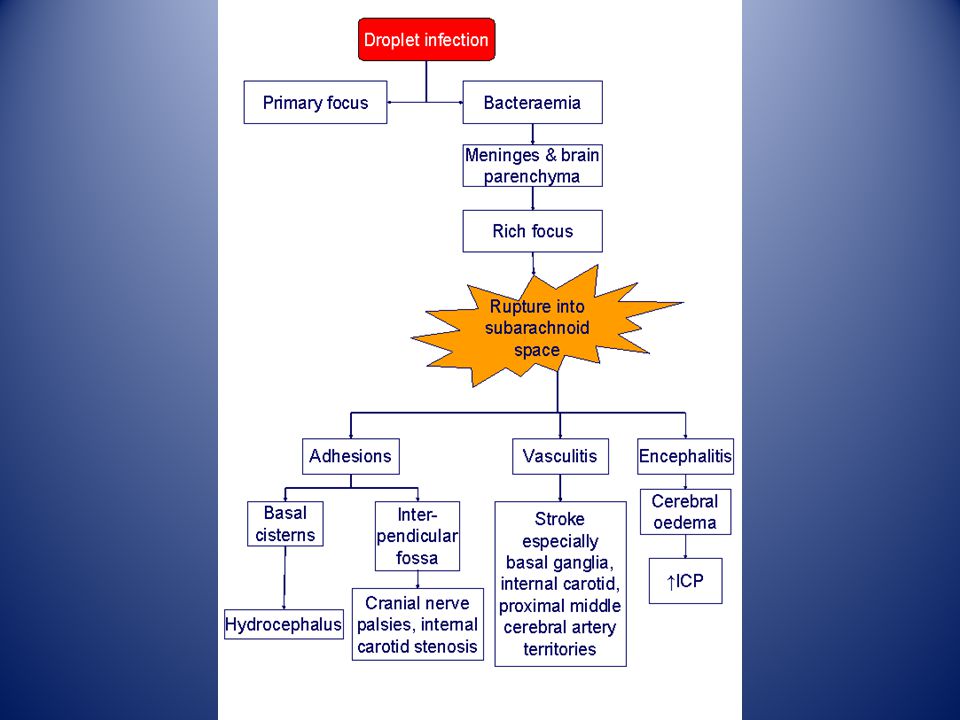
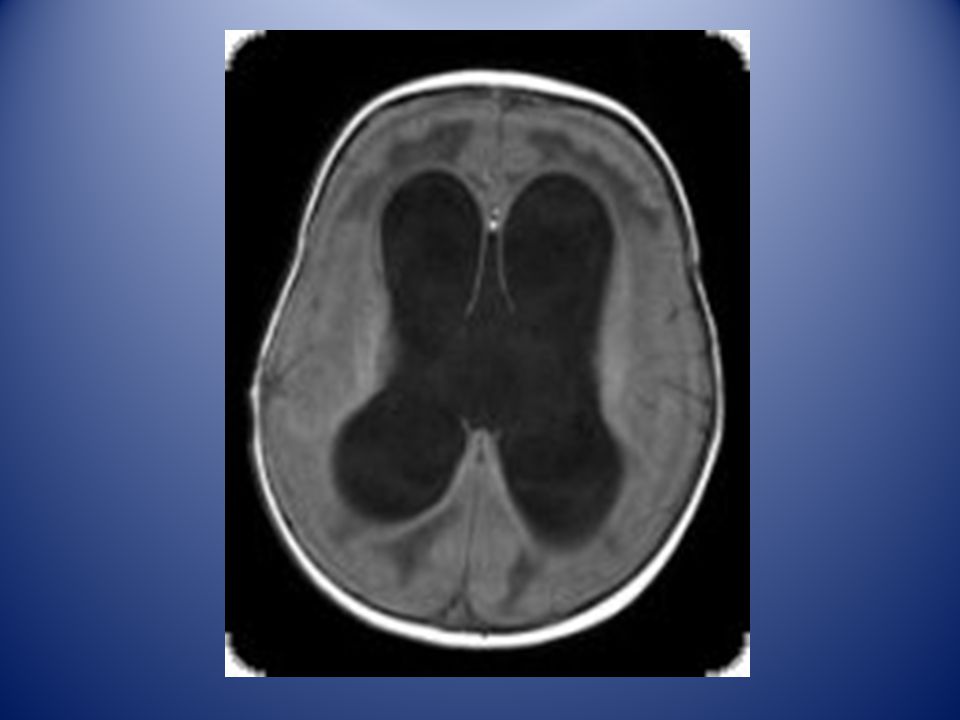
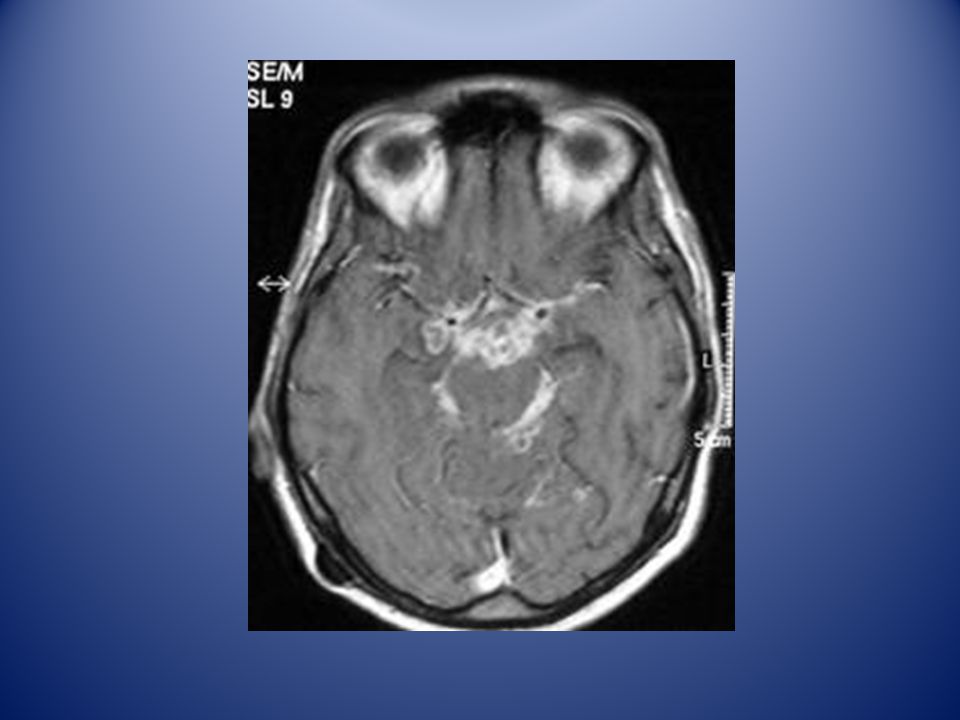
Approximately 6% of all cases of extrapulmonary TB involve the central nervous system (CNS). The peak incidence of CNS TB is in newborn to 4-year-old children. Tuberculous meningitis usually results from the rupture of a subependymal tubercle into the subarachnoid space, rather than from direct hematogenous seeding of the CNS.
. The peak incidence of CNS TB is in newborn to 4-year-old children. Tuberculous meningitis usually results from the rupture of a subependymal tubercle into the subarachnoid space, rather than from direct hematogenous seeding of the CNS.")
20
Gastrointestinal Disease
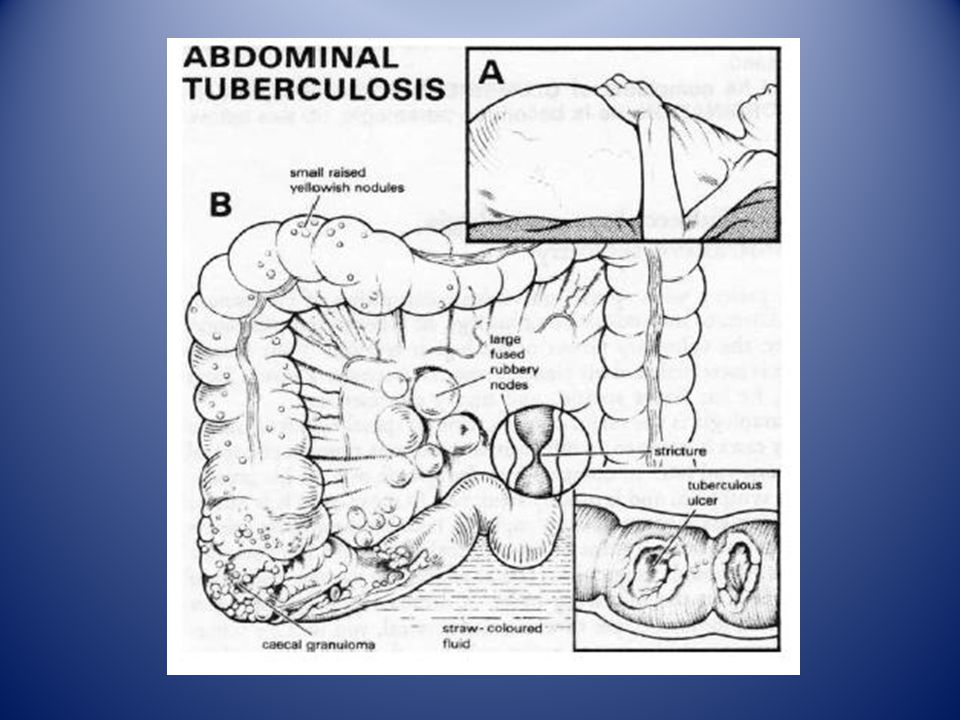
Gastrointestinal TB infection usually is secondary to hematogenous or lymphatic spread but also may result from swallowed bronchial secretions or direct spread from local sites, such as lymph nodes or fallopian tubes. TB may occur in any gastrointestinal location from the mouth to the anus, but lesions proximal to the terminal ileum are rare. The ileocecal area is the most common site of involvement, producing signs and symptoms of pain, anorexia, diarrhea, obstruction, hemorrhage, and often a palpable mass.

21
The most common clinical manifestations of gastrointestinal TB are abdominal pain, fever, weight loss, anorexia, nausea, vomiting, and diarrhea. Approximately 12 to 16% of cases present as an acute abdomen. The signs and symptoms can be so similar to those of other diseases that the diagnosis often is made at surgery. The clinical manifestations of anal TB include fissures, fistulas, and perirectal abscesses.

23
Peritonitis Tuberculous peritonitis may develop from local spread of MTB infection from a tuberculous lymph node, intestinal focus, or infected fallopian tube. In addition, peritonitis can develop from seeding of the peritoneum in miliary TB or from the reactivation of a latent focus. The patient commonly has pain and abdominal swelling associated with fever, anorexia, and weight loss.

24
Paracentesis is essential for diagnosis
Paracentesis is essential for diagnosis. The peritoneal fluid is exudative, with a cell count of 500 to 2000 cells per mL. Lymphocytes usually predominate, with rare exceptions early in the process, when polymorphonuclear leukocytes may predominate. AFB smears of the fluid have a low diagnostic yield, with a reported sensitivity of no more than 7%, and the culture result is positive in only 25% of the cases. Peritoneal biopsy often is necessary to confirm the diagnosis.

27
GENERAL COMMENTS ON TREATMENT OF EXTRAPULMONARY TUBERCULOSIS

28
Extrapulmonary foci usually respond to treatment more rapidly than does cavitary pulmonary tuberculosis due to the lower burden of organisms in the former. Therapy with four-drug regimens (INH, RMP, PZA, and EMB) for 2 months, followed by INH and RMP for 4 months, is advised in most cases caused by drug-sensitive organisms. The exceptions include bone and joint disease (6 to 9 months), and tuberculous meningitis (9 to 12 months though optimal duration unknown). Adjunctive corticosteroids are recommended for persons with pericardial or central nervous system (CNS) tuberculosis.
 for 2 months, followed by INH and RMP for 4 months, is advised in most cases caused by drug-sensitive organisms. The exceptions include bone and joint disease (6 to 9 months), and tuberculous meningitis (9 to 12 months though optimal duration unknown). Adjunctive corticosteroids are recommended for persons with pericardial or central nervous system (CNS) tuberculosis.")
29
In lymph node TB, the most common form of extrapulmonary TB, the affected nodes may enlarge while patients are receiving appropriate therapy and even after completion of therapy without evidence of bacteriological relapse. For large lymph nodes that are fluctuant and appear to be about to drain spontaneously, aspiration (traverse through normal skin) or incision and drainage appears to be beneficial.
 or incision and drainage appears to be beneficial.")
Similar presentations















 Environmental.>")


 in the tissues, especially the lungs.>")
 Aboriginal 1 Month Cough, SOBE,Fever Cough non productive No orthopnea, PND, LL swelling Fever.>")





. -Cytological tests (>")

