Download presentation
Presentation is loading. Please wait.

2
Prof., Dr. :sherif wadie

3
Reticular activating system (RAS)
")
4
Good Consciousness = Alertness + Awareness

5
Diminished alertness = Widespread abnormalities of cerebral hemispheres or reduced activity of reticular activating system (RAS)
")
6
Confusion : Impaired attention and concentration, manifest disorientation in time, place and person, impersistent thinking, speech and performance, reduced comprehension and capacity to reason Fluctuate in severity, typically worse at night ‘sundowning’ Perceptual disturbances and misinterpret voices, common objects and actions of other persons Confusion is also found in dementia (progressive failure of language, memory, and other intellectual functions)
")
7
Delirium : confusion and associated agitation, hallucination, convulsion and tremor Amnesia : a loss of past memories and to an ability to form new ones, despite alert and normal attentiveness

8
Alert : normal awake and responsive state Drowsiness : state of apparent sleep, briefly arousal with oral command Lethargic : resembles sleepiness, but not becoming fully alert, slow verbal response and inattentive. Unable to adequately perform simple concentration task (such as counting 20 to 1)
.")
9
Somnolent : easily aroused by voice or touch; awakens and follows commands; required stimulation to maintain arousal Obtunded/Stuporous : arousable only with repeated and painful stimulation; verbal output is unintelligible or nil; some purposeful movement to noxious stimulation Comatose : no arousal despite vigorous stimulation, no purposeful movement- only posturing, brainstem reflexes often absent

10
Dementia Longstanding nature Varies little from time to time Memory problem Confusional state Acute Fluctuate Clouding of consciousness

11
Medical or surgical disease Metabolic disorders Hepatic Uremic Hypo and hypernatremia Hypercalcemia Hypo and hyperglycemia Hypoxia Hypercapnia

12
Infectious illness Pneumonia Endocarditis Urinary tract infection Peritonitis Congestive heart failure Postoperative and posttraumatic states

13
Drug intoxication Opiates Barbiturates Other sedatives

14
Diseases of nervous system Cerebrovascular disease, tumor, abscess Subdural hematoma Meningitis Encephalitis Cerebral vasculitis Hypertensive encephalopathy

15
Alcoholism. Depression. Diabetes. Drug overdose Head injuries Encephalitis Epilepsy Stroke causes of confusional state (5)
.")
16
History --- emphasizing the patient’s condition before the onset of confusion Clinical examination --- focus on signs of diminished attentiveness, disorientation, and drowsiness and the presence of localizing neurological signs

17
Control underlying medical illness Quiet the patient and protect him from injury - Discontinue drugs that could possibly be responsible for the acute confusional state : sedating, antianxiety, narcotic, anticholinergic, antispasticity, corticosteroid, L-dopa, metoclopramide, cimetidine, antidepressant, antiarrhythmic, anticonvulsant, antibiotics.

18
- Haloperidol, quetiapine, risperidone are helpful in calming the agitated and hallucinating patient, but should be used in the lowest effective doses - In alcohol or sedative withdrawal— chlordiazepoxide is the drug of choice. Chloral hydrate, lorazepam, and diazepam are equally effective

20
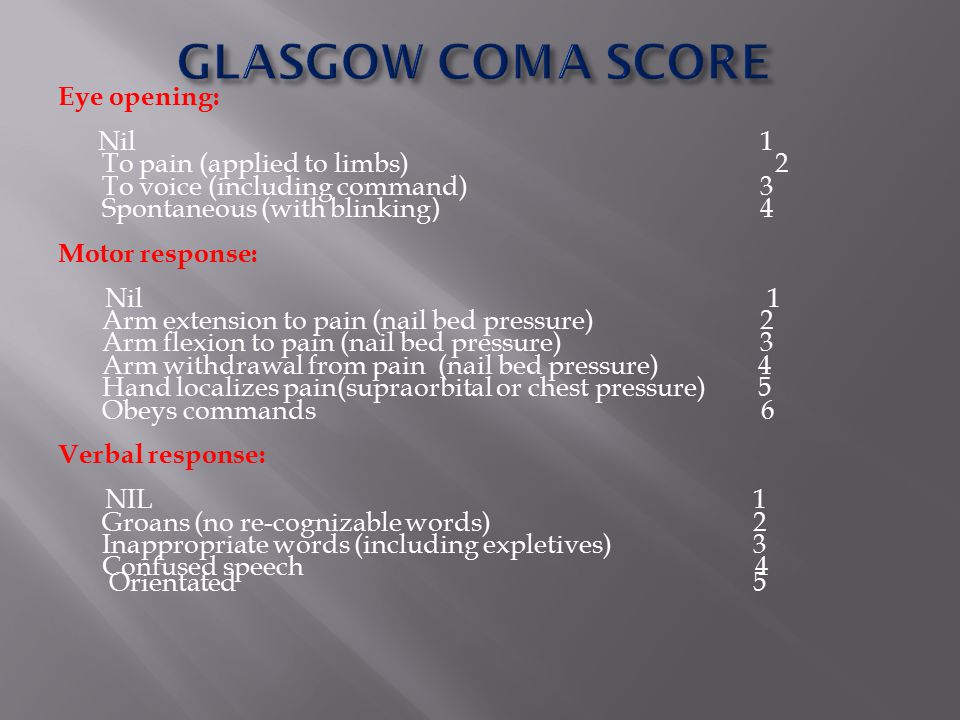
Eye opening: Nil 1 To pain (applied to limbs) 2 To voice (including command) 3 Spontaneous (with blinking) 4 Motor response: Nil 1 Arm extension to pain (nail bed pressure) 2 Arm flexion to pain (nail bed pressure) 3 Arm withdrawal from pain (nail bed pressure) 4 Hand localizes pain(supraorbital or chest pressure) 5 Obeys commands 6 Verbal response: NIL 1 Groans (no re-cognizable words) 2 Inappropriate words (including expletives) 3 Confused speech 4 Orientated 5
 2 To voice (including command) 3 Spontaneous (with blinking) 4 Motor response: Nil 1 Arm extension to pain (nail bed pressure) 2 Arm flexion to pain (nail bed pressure) 3 Arm withdrawal from pain (nail bed pressure) 4 Hand localizes pain(supraorbital or chest pressure) 5 Obeys commands 6 Verbal response: NIL 1 Groans (no re-cognizable words) 2 Inappropriate words (including expletives) 3 Confused speech 4 Orientated 5")
21
Glasgow Coma Scale : Eye opening (E)
")
22
Glasgow Coma Scale : Motor response (M)
")
23
Glasgow Coma Scale : Verbal response (V)
")
24
Notes 1. scoring from the best response 2. verbal response will not correct in the condition of aphasia, intubation and facial injury 3. sensory loss may interfere painful stimulation 4. eye opening may be interfered by orbital swelling and 3 rd CN palsy 5. arm movements may be impaired from local trauma or cervical cord lesion GLASGOW COMA SCORE

25
History Circumstances and rapidity with which neurologic symptoms developed Immediately preceding medical and neurologic symptoms Use of medications, illicit drugs, or alcohol Chronic liver, kidney, lung, heart, or other medical disease

26
Vital sign Temperature Fever Hypothermia -- <31°C causes coma Pulse Respiratory rate and pattern Blood pressure Funduscopic examination Cutaneous lesion

27
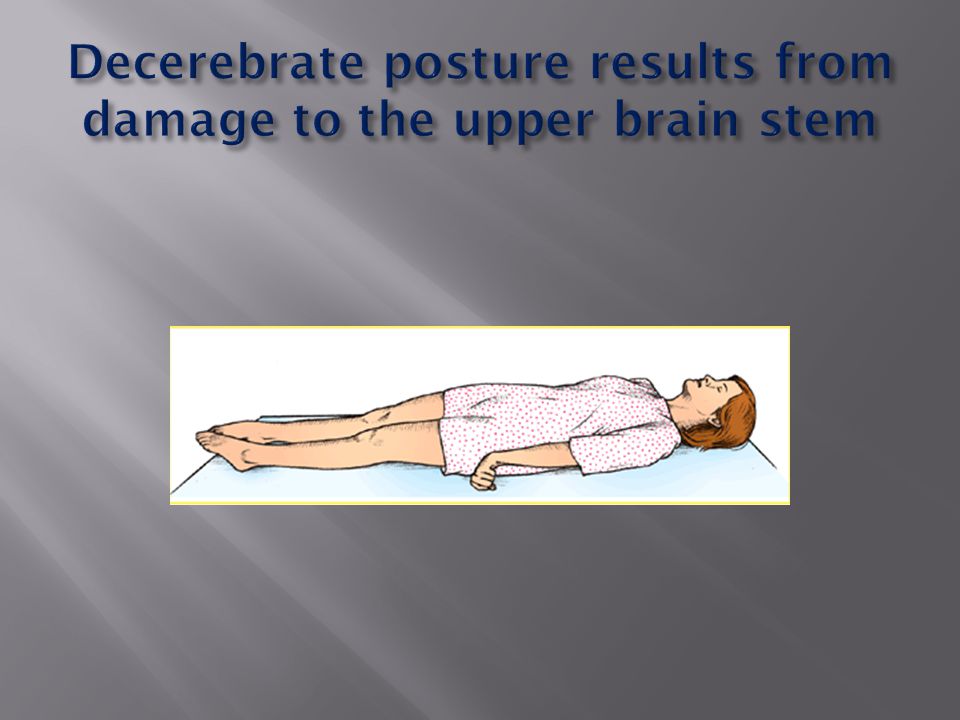
Observe Movement : restless, twitching, multifocal myoclonus, asterisks Decorticate rigidity Suggest severe bilateral damage rostral to midbrain Decerebrate rigidity Indicate damage to motor tracts in the midbrain or caudal diencephalon

30
Level of arousal and elicited movements Brainstem reflexes pupils Ocular movements respiration

31
DESCRIPTIONSINTERPRETATION Small, reactiveMetabolic causes Diencephalic lesion Midposition, fixedMid brain lesion large, fixedExtensive brain stem lesion Anoxia Sedative overdose Anticholinergic poisoning or mydriatic eyedrops Pin pointPontine lesion Opiates Unilateral fixed dilatedThird nerve palsy

33
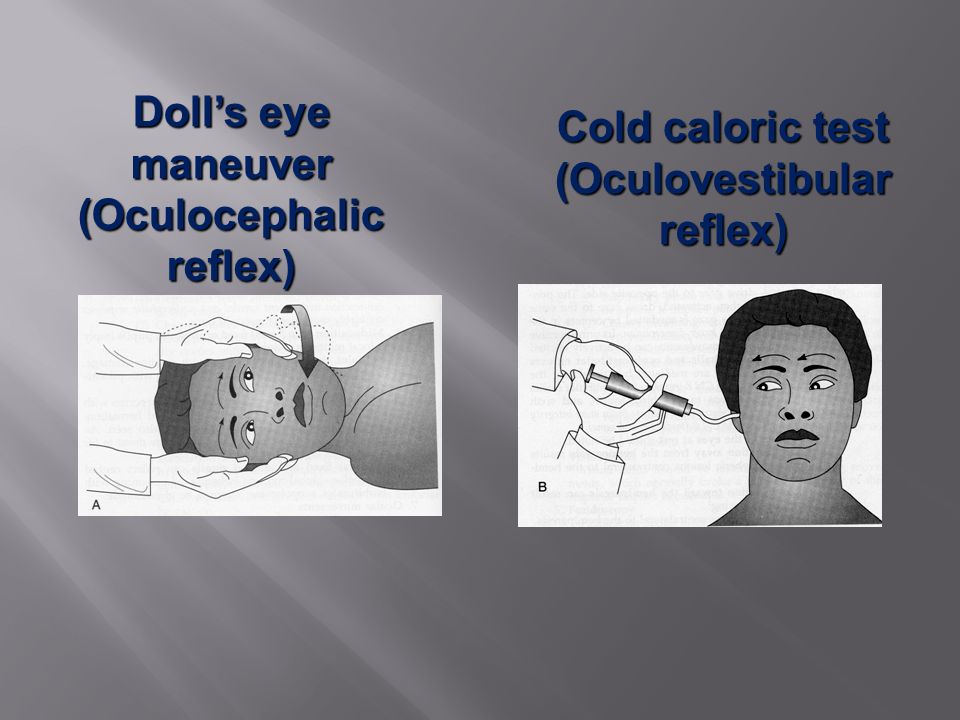
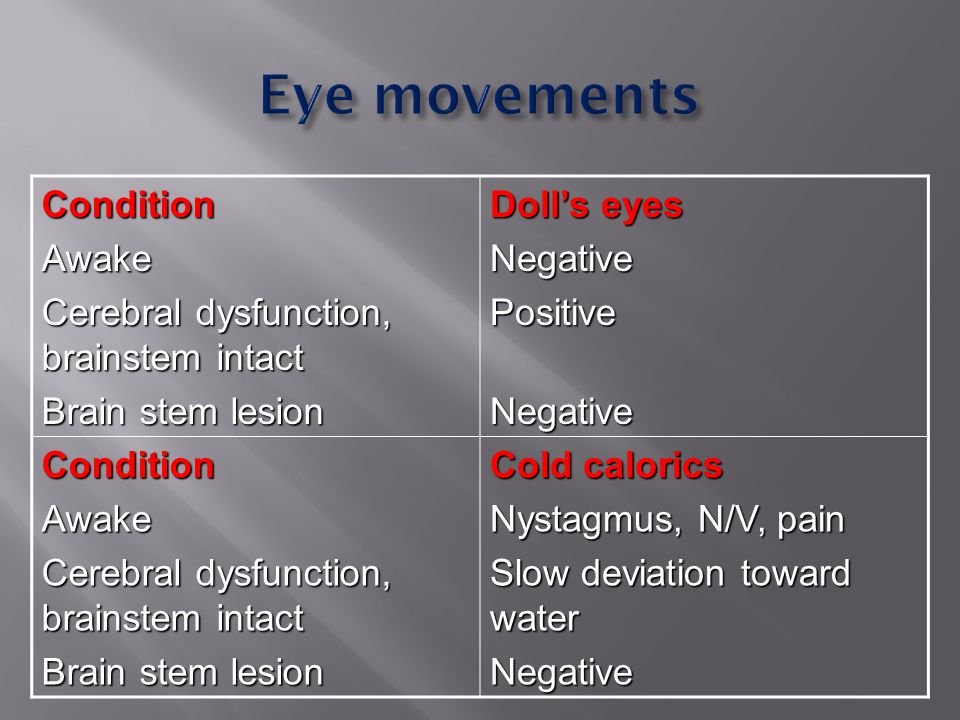
Doll’s eye maneuver (Oculocephalic reflex) Cold caloric test (Oculovestibular reflex)
 Cold caloric test (Oculovestibular reflex)")
35
ConditionAwake Cerebral dysfunction, brainstem intact Brain stem lesion Doll’s eyes NegativePositive Negative NegativeConditionAwake Cerebral dysfunction, brainstem intact Brain stem lesion Cold calorics Nystagmus, N/V, pain Slow deviation toward water Negative

36
Respiratory patterns

37
Cheyne-Stokes respiration : bilateral cortical or bilateral thalamic lesions, metabolic disturbances, incipient transtentorial herniation Hyperventilation : midbrain or pons lesions Apneusis : lateral tegmentum of lower half of pons Cluster : lower pontine or high medullary lesions Ataxic : dorsomedial medulla lesion

38
Least useful sign because : Acid-base derangements Hypoxia Cardiac influences

39
Brain death Locked-in syndrome Vegetative state Frontal lobe disease Non-convulsive status epilepticus Psychiatric disorder (catatonia, depression)
")
40
An awake but unresponsive state Extensive damage in both cerebral hemisphere Retained respiratory and autonomic functions Cardiac arrest and head injury are the most common causes.

41
Awake patient has no means of producing speech or volitional limb, face and pharyngeal movements Vertical eye movement and lid elevation remain unimpaired Infarction or hemorrhage of the ventral pons

42
COMA LOCALIZING SIGNNO LOCALIZING SIGN SUPRATENTORIALINFRATENTORIAL NO STIFF NECK STIFF NECK - CVD - TUMOUR - ABSCESS STRUCTURAL DAMAGE FUNCTIONAL NEURONAL DEPRESSION - HYPOXIA - CARDIAC ARREST - ENCEPHALITIS - HEPATIC - URAEMIC - POST ICTAL STATE - FLUID ELECTROLYTE IMBALANCE - DRUGS - SAH - MENINGITIS

43
CBC FBS BUN, Creatinine Electrolyte, calcium LFT Drug screen, toxicology screen

44
EKG CT or MRI brain CSF exam EEG

45
Recovery from coma depends primarily on the causes, rather than on the depth of coma Intoxication and metabolic causes carry the best prognosis Coma from traumatic head injury far better than those with coma from other structural causes Coma from global hypoxic-ischemic carries least favorable prognosis At 3 rd day, no papillary light reflex or GCS < 5 is associated with poor prognosis

46
Central transtentorial herniation

47
Uncal transtentorial herniation Uncal transtentorial herniation Brain Herniation

48
Intubation and hyperventilation (P CO 2 25-30 mmHg) Mannitol (0.5-1 gm/kg body weight or 20% mannitol 200 cc. infusion 10-20 minutes repeat every 4 hours if necessary Furosemide 20-40 mg IV Dexamethasone 4-10 mg IV q 6 hours decrease perilesional vasogenic cerebral edema. Active at 24-48 hours. Consult surgery

Similar presentations