Download presentation
Presentation is loading. Please wait.

1
Psychological Care in Stroke: What is important and whose responsibility is it? Dr Jane Barton Consultant Clinical Psychologist

2
Overview What is psychological care? What is the scale of the problem? Why are we focussing on this now? The context & current drivers What can we do about it?

3
Emotional experience of stroke “We’re not just legs and arms and a mouth…we are human beings with a mixture of emotions. All these feelings…self esteem, self worth, confidence, identity …they’re all under attack after a stroke…you can feel vulnerable, frightened and you can lose yourself. Psychological support puts you back together again - especially psychological support from someone who’s been down that road before. The timing can’t be predicted…sometimes it’s when you come out into your real world after hospital or it may be two - or more – years later when you discover that you will not make a ‘full’ recovery…it’s about reinvention and finding direction” Harry Clarke, Counsellor at Connect who has aphasia (Taken from Psychological Care after Stroke, NHS Improvement, 2011)
.")
4
Psychological care in physical health settings – what is it? Essentially about integrating a psychological content within the overall physical care. It is not something that stands alone and is separate from physical care. Should be organised, systematic and practical. Everybody’s business!

5
Psychological Care (Nichols 2003) Level 1 Awareness of psychological issues Patient centred listening & communication Awareness of patient’s psychological state Level 2 Monitoring psychological state; keeping records Information & education Counselling & support Level 3 Psychological therapy & interventions
 Level 1 Awareness of psychological issues Patient centred listening & communication Awareness of patient’s psychological state Level 2 Monitoring psychological state; keeping records Information & education Counselling & support Level 3 Psychological therapy & interventions")
6
What is the scale of the problem? Psychological & mental health consequences of stroke

7
Scale of the problem 1 Cognitive impairment Problems with memory, concentration, planning, sequencing, decision making, insight Approx 75% experience cognitive impairment Approx 35% have significant impairment long term Significant proportion go on to develop dementia

8
Scale of the problem 2 Depression Most common psychological presentation Approx 25-50% Independent of disability Fluctuating course

9
Scale of the problem 3 Anxiety Between 30-49% up to 12 years post stroke Phobias, generalised anxiety, panic Trauma response - PTSD 20% show trauma response Flashbacks, avoidance, hyperarousal

10
The Impact Untreated psychological mood disorders are associated with higher rates of : Mortality Suicide Long term disability & institutionalisation Hospital readmission Higher utilisation of outpatient services

11
Mental Illness Associated with Stroke Depressive disorders increase risk of cardiovascular disease by 1.5x the general population, equivalent to risk from smoking or diabetes People with severe mental illness have a 2.5x greater mortality from stroke Those receiving highest doses of antipsychotic medication are at greatest risk of death from both CHD and stroke Psychological stress associated with an 11% increased risk of stroke

12
Why are we focussing on this now? Recent audits National drivers

13
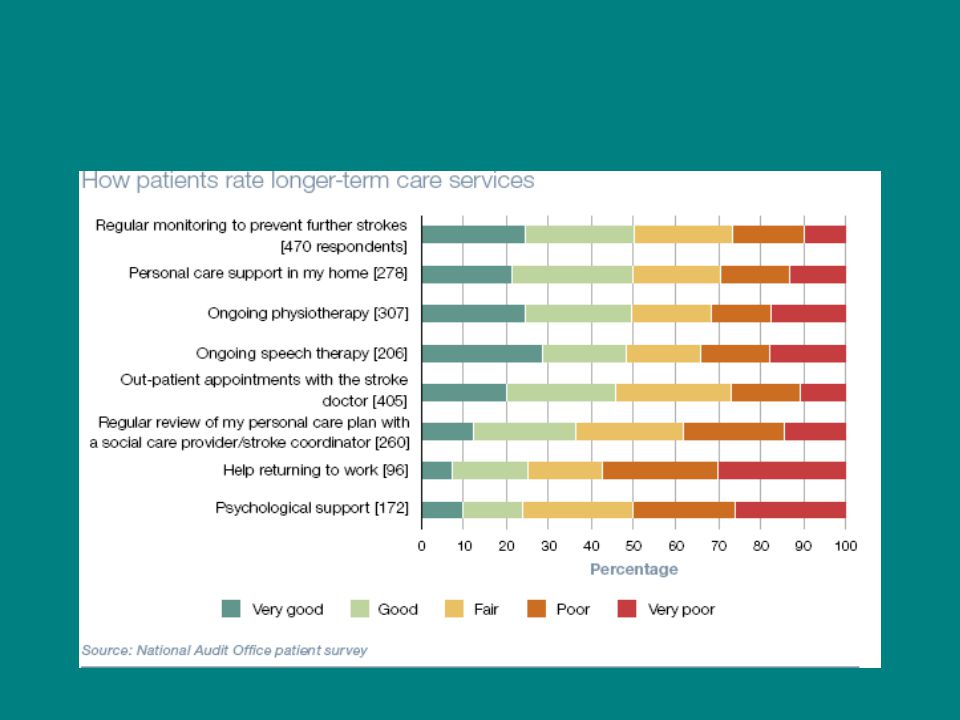
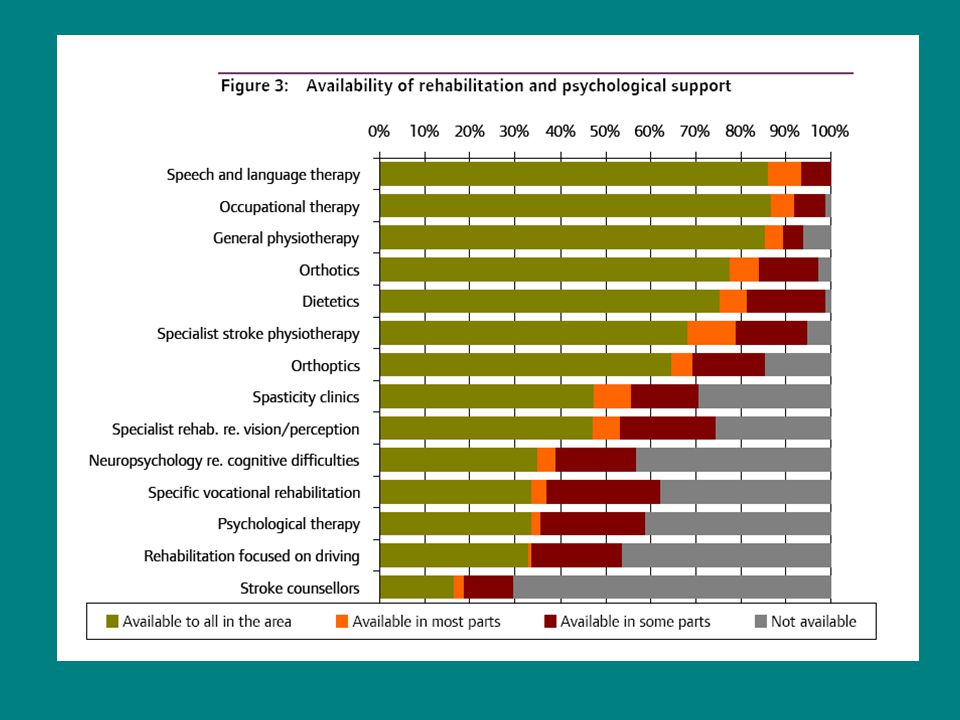
Audits & Reviews National reviews of stroke services demonstrate the need for improvement CQC in 2011 found psychological support for patients and carers was less than readily available NAO reported that psychological support for patients and carers was lacking

16
Policy & Guidance National Stroke Strategy (2007) RCP Guidelines for stroke (2004; 2008) And…
 RCP Guidelines for stroke (2004; 2008) And…")
17
“No health without mental health” (DH, 2011) “There is a clear link between mental and physical health and an urgent need to strengthen the provision of mental health care to people with physical illness and the quality of physical health care to people with mental health problems in general hospitals and in primary care”
 There is a clear link between mental and physical health and an urgent need to strengthen the provision of mental health care to people with physical illness and the quality of physical health care to people with mental health problems in general hospitals and in primary care")
18
What can we do about it?

19
NAO report led to NHS commitment to improve 9 domains through Accelerating Stroke Improvement Psychological support – ASI 6 Targets set Guidance on developing services

20
Psychological Care After Stroke (NHS Improvement, 2011) Guidance on developing services Addressing psychological need after stroke should be accepted as an essential part of the culture of stroke services and equivalent to the management of physical need. Stepped care model

21
Stepped Care approach to psychological care A hierarchical approach. Offers simpler interventions first, progressing onto more complex interventions if required. Not necessarily a linear process. Makes best use of skills of MDT & utilises more specialist staff for more complex problems.

22
Stepped Care Model for psychological interventions after stroke ( NHS Improvement 2011) Level 3: Severe and persistent disorders of mood and/or cognition – requiring specialist intervention from clinical psychology / Mental Health Level 2: Mild/moderate symptoms of impaired mood and / or cognition that interfere with rehab – requiring specialist stroke staff with psychol / MH expertise. Level 1: Sub-threshold problems – requiring awareness and screening by stroke specialist staff

23
Level 1 Screening & sub threshold problems Task Awareness of psychological issues & patient’s psychological state Providing low level psychological care: e.g. patient centred listening & communication Alerting others & signposting on Ensuring discussion & review at MDT Mood and Cognitive screening By whom? The whole of the MDT – everyone! Sub group with training

24
Psychological Screening Formal, standardised measures (RCP, 2008) Mood & distress PHQ-9; GAD-7 DISCS – aphasia SADQ – severe aphasia / cognition Cognition ACE-R MOCA
 Mood & distress PHQ-9; GAD-7 DISCS – aphasia SADQ – severe aphasia / cognition Cognition ACE-R MOCA")
25
Level 2 Mild – Moderate problems Task Further assessment & monitoring Brief psychological interventions (including psychotherapeutic groups) Onward referral & signposting – to clinical psychology By whom? MDT staff with additional competence in psychological / mental health

26
Level 3 Severe or persistent mood / cognitive problems Task Specialist assessment with complex mood & cognitive presentations Suicide risk assessment and management Psychological interventions & therapy Liaison & onward referral to specialist MH services By Whom? Clinical Psychologists…….with training in neuropsychology Specialist mental health practitioners

27
Summary Understand the importance of physical and mental health Raise awareness within the services Know your role and level of expertise This is everybody’s business!!

Similar presentations