Download presentation
Presentation is loading. Please wait.

1
Case based discussion Pankaj Malhotra PGIMER, Chandigarh, India

2
Case History A 43-year old gentleman presented with weakness and fatigability x 3 months Hb 13.4 gm/dl, WBC 220,000 cells/mm3, Plat 679000 cells/mm3 Spleen 10 cm BM: Hypercellular, 8% blasts, Ph 20/20 positive, Q RT PCR for BCR ABL mRNA 80% Sokal High-risk

3
Case History A 43-year old gentleman presented with weakness and fatigability x 3 months Hb 13.4 gm/dl, WBC 220,000 cells/mm3, Plat 679000 cells/mm3 Spleen 10 cm BM: Hypercellular, 8% blasts, Ph 20/20 positive, Q RT PCR for BCR ABL mRNA 80% Sokal High-risk Availability of Imatinib/Dasatinib/Nilotinib

4
Choice of first line therapy Feb 2013 1.Imatinib 400 mg OD 2.Imatinib 800 mg OD 3.Dasatinib 100 mg OD 4.Nilotinib 300 mg BD 5.Nilotinib 400 mg BD 6.Bosutinib 500 mg OD Would Sokal high-risk score have impact on the choice of first line therapy?

5
Choice of first line therapy Feb 2013 1.Imatinib 400 mg OD 2.Imatinib 800 mg OD 3.Dasatinib 100 mg OD 4.Nilotinib 300 mg BD 5.Nilotinib 400 mg BD 6.Bosutinib 500 mg OD Does enough finances/insurance coverage impact on choice of first line therapy

6
Case History A 43-year old gentleman presented with weakness and fatigability x 3 months Hb 13.4 gm/dl, WBC 220,000 cells/mm3, Plat 679000 cells/mm3 Spleen 10 cm BM: Hypercellular, 8% blasts, Ph 20/20 positive, Q RT PCR for BCR ABL mRNA 80% Sokal High-risk Active coronary artery disease and AF

7
Choice of first line therapy Feb 2013 1.Imatinib 400 mg OD 2.Imatinib 800 mg OD 3.Dasatinib 100 mg OD 4.Nilotinib 300 mg BD 5.Nilotinib 400 mg BD 6.Bosutinib 500 mg OD Would active coronary artery disease & AF impacts your decision making?

8
Case History A 43-year old gentleman presented with weakness and fatigability x 3 months Hb 13.4 gm/dl, WBC 220,000 cells/mm3, Plat 679000 cells/mm3 Spleen 10 cm BM: Hypercellular, 8% blasts, Ph 20/20 positive, Q RT PCR for BCR ABL mRNA 80% Sokal High-risk Past history of pulmonary tuberculosis

9
Choice of first line therapy Feb 2013 1.Imatinib 400 mg OD 2.Imatinib 800 mg OD 3.Dasatinib 100 mg OD 4.Nilotinib 300 mg BD 5.Nilotinib 400 mg BD 6.Bosutinib 500 mg OD Would a past history of lung infection impacts your decision making?

10
Choice of first line therapy depends upon 1.Available finances/Full insurance 2.Side effect profile of the drugs 3.Co-morbid conditions of the patient 4.Phase of the disease(Acc or BC) 5.Sokal score (?)
 5.Sokal score ( )")
12
Choice of first line therapy depends upon 1.Available finances/Full insurance 2.Side effect profile of the drugs 3.Co-morbid conditions of the patient 4.Phase of the disease(Acc or BC) 5.Sokal score (?) 6.Physician preference/Patient preference (?)
 5.Sokal score ( ) 6.Physician preference/Patient preference ( )")
13
Comparison of TKI Favour Imatinib Cheaper Long-term experience Known side effect profile CCyR 70% at 1 year Less effective More than 100 mutations Favour 2 nd G TKI More effective CCyR 80-85% Fewer mutations (<10) Costly Post marketing surveillance suggest some unusual side effect Fewer options if disease progress
 Costly Post marketing surveillance suggest some unusual side effect Fewer options if disease progress")
15
The patient was started on Imatinib 400 mg/day

16
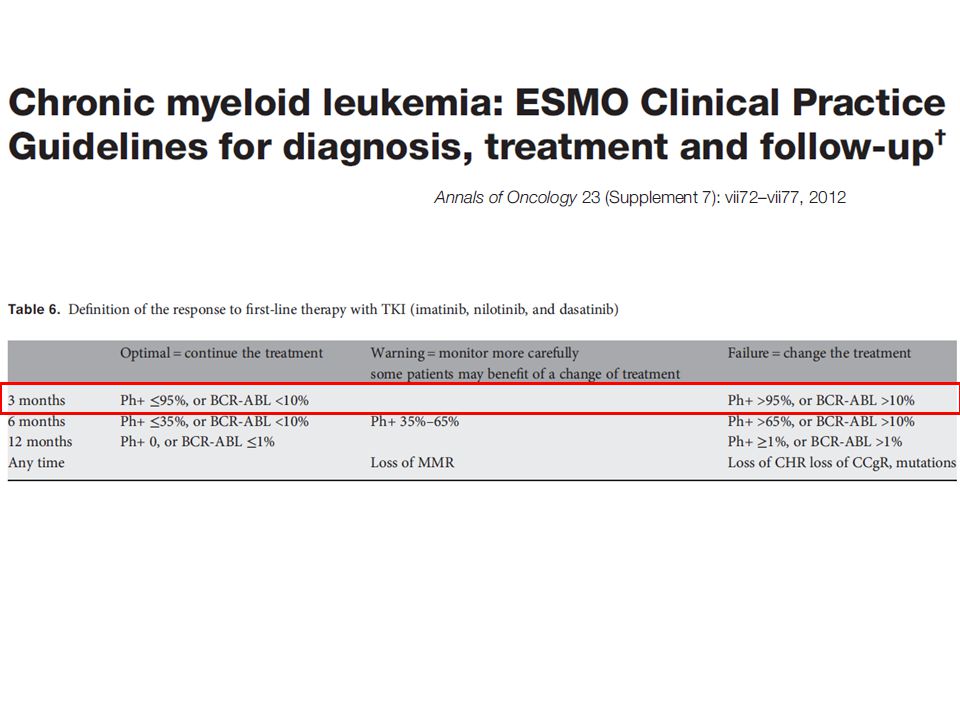
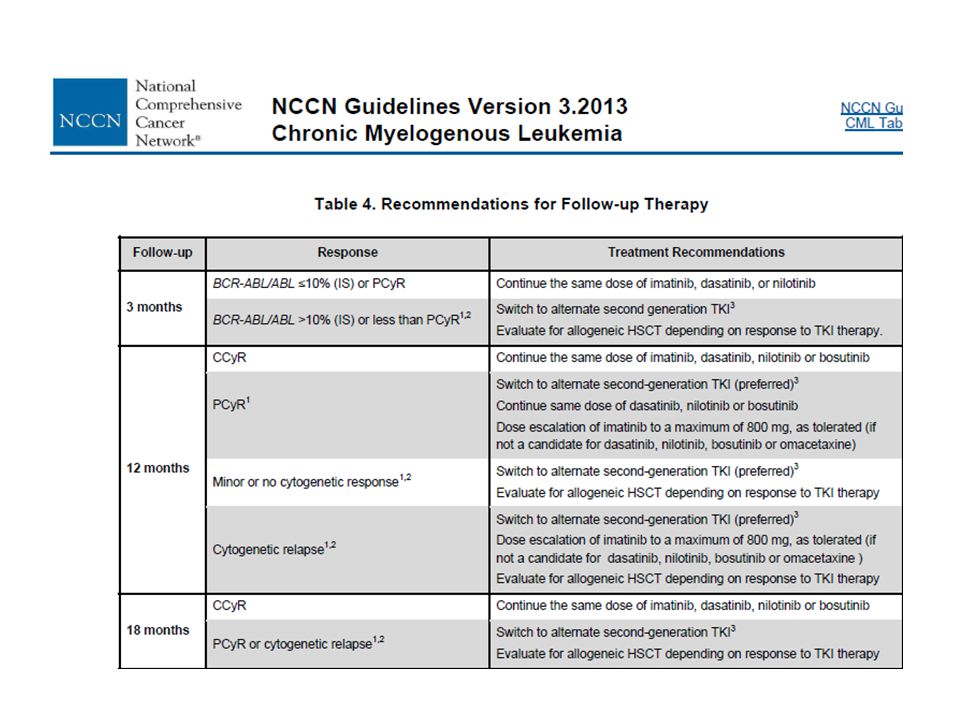
Progress Achieved CHR by 2 months RQ PCR for BCR-ABL at 3 months 22% IS What are the long-term chances of PFS of this gentleman? ( RQ PCR >10% at 3 months)? 1.High 2.Low What are the long-term chances of PFS of this gentleman? ( RQ PCR >10% at 3 months)? 1.High 2.Low
. 1.High 2.Low What are the long-term chances of PFS of this gentleman. ( RQ PCR >10% at 3 months). 1.High 2.Low.")
17
Progress Achieved CHR by 2 months RQ PCR for BCR-ABL at 3 months 12% IS What are the long-term chances of PFS of this gentleman? ( RQ PCR >10% at 3 months)? 1.High 2.Low What are the long-term chances of PFS of this gentleman? ( RQ PCR >10% at 3 months)? 1.High 2.Low
. 1.High 2.Low What are the long-term chances of PFS of this gentleman. ( RQ PCR >10% at 3 months). 1.High 2.Low.")
20
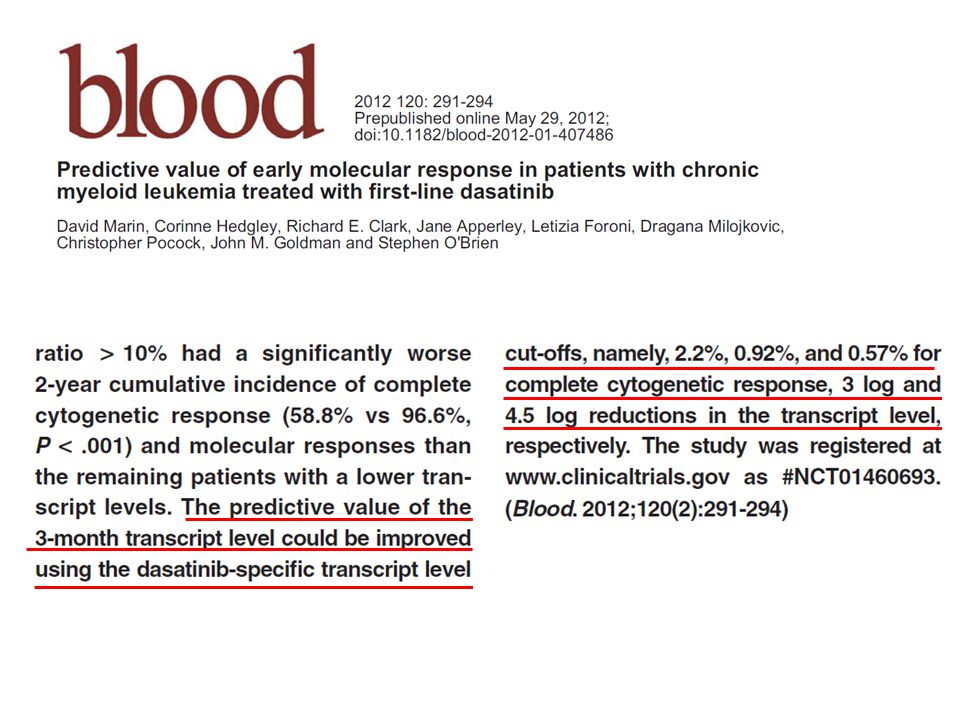
The patient was started on Dasatinib 100 mg/day

21
Progress Achieved CHR by 2 months RQ PCR for BCR-ABL at 3 months 12% IS What are the long-term chances of PFS of this gentleman? ( RQ PCR >10% at 3 months)? 1.High 2.Low What are the long-term chances of PFS of this gentleman? ( RQ PCR >10% at 3 months)? 1.High 2.Low
. 1.High 2.Low What are the long-term chances of PFS of this gentleman. ( RQ PCR >10% at 3 months). 1.High 2.Low.")
25
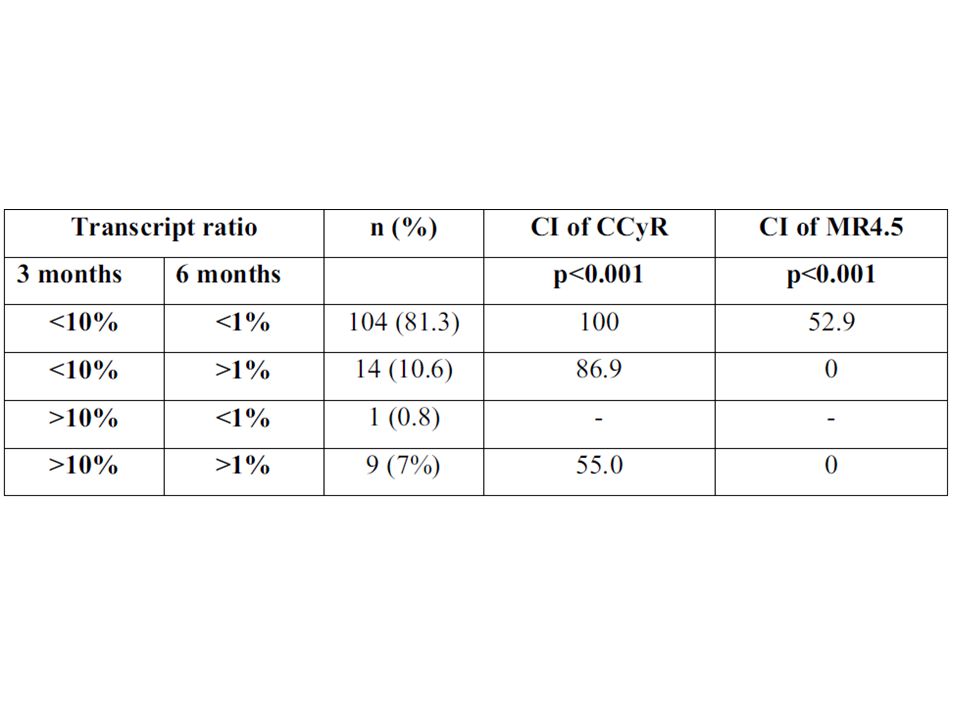
Thus with 2 nd G TKI, you expect more rapid response, may be CCyR at 3 months/BCR ABL <2% at 3months

28
Assessment at 6 -months Glivec 400 mg/day continued Hb 10.0 gm/dl MCV 102 WBC 3500 cells/mm3 Plat 100,000 cells/mm3 BM: Mild hypocellular Cytogenetics 2/20 = MCyR Q PCR 1% IS What is your assessment and would you consider change in your strategy?

31
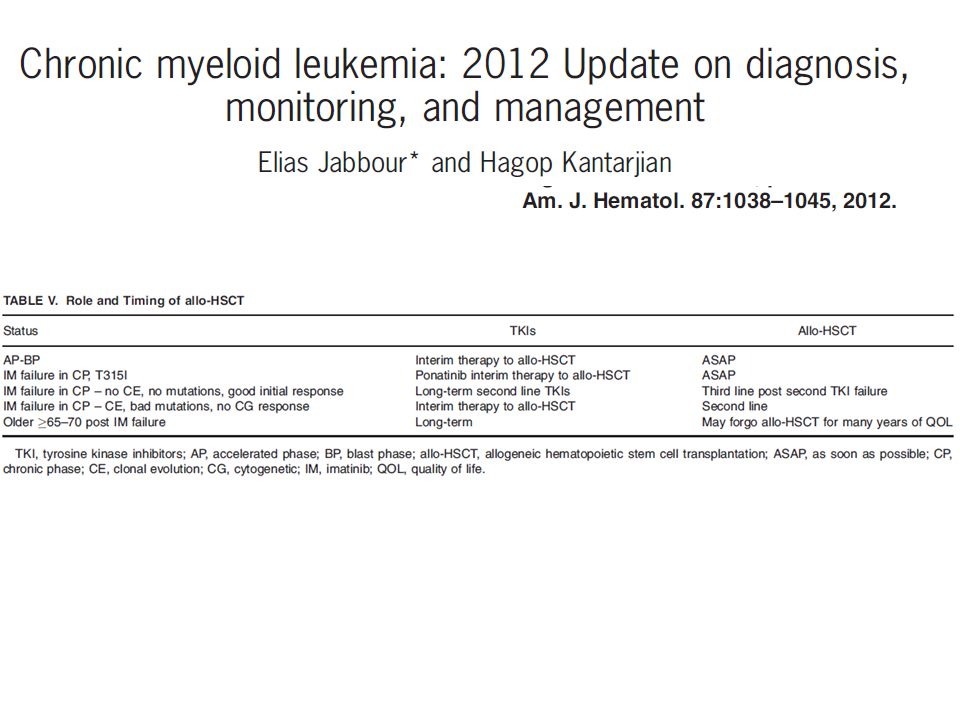
Current role of Allo HSCT

33
Conclusions Rapid advancement taking place in the field of CML Availability of many drugs have made life easy as well as difficult both for the physician as well as the patient Need to continue update our knowledge on CML on the basis of continuously emerging data

Similar presentations










 Trial (DASISION, CA180-056)1.>")






>")
: ENESTnd Beyond One Year Larson.>")




 vs Imatinib (IM) in Patients (pts) with Newly Diagnosed Chronic Myeloid Leukemia in Chronic Phase (CML-CP) and the Impact.>")
