Download presentation
Presentation is loading. Please wait.

1
IMPLEMENTING THE HCH FOR PATIENTS WITH AD: EARLY IDENTIFICATION, CARE COORDINATION & CAREGIVER SUPPORT Health Care Homes Learning Day, November 1, 2012 1

2
Session Overview Introduction to Health Care Home (HCH) Overview Successful HCH: physician & care coordinator perspectives Alzheimer’s Disease and HCH Overview AD in HCH: physician & care coordination roles Alzheimer’s Disease: Firsthand experience Conclusion / Q&A
 Overview Successful HCH: physician & care coordinator perspectives Alzheimer’s Disease and HCH Overview AD in HCH: physician & care coordination roles Alzheimer’s Disease: Firsthand experience Conclusion / Q&A")
3
Successful HCH Dr. Johnson presentation Panel discussion

4
AD Overview 4

5
Facts & Figures& Figures Alzheimer’s Association 2011

6
Today, Alzheimer’s Disease Is: Fatal Prevalent Expensive Misunderstood Stigmatized Under-diagnosed Under-treated ON THE RISE….

7
Alzheimer’s Epidemic By 2050: 13 million to 16 million Americans will have AD Consume 1.1 trillion in healthcare spending

8
Today Fewer than 50% of patients receive formal diagnosis Diagnosis often delayed by 6+ Years Impairment in function by time it is recognized Fewer than 50% of those diagnosed receive any treatment

9
Why is Early Diagnosis Important? 1. Optimize current medical management 2. Relief gained from better understanding 3. Maximize decision-making autonomy 4. Access to services 5. Risk reduction 6. Plan for the future* 7. Improve clinical outcomes* 8. Avoid or reduce future costs 9. Diagnosis as a human right World Alzheimer Report 2011 *Top benefits endorsed by physicians, International Alzheimer’s Disease Physician Survey, 2012

10
Alzheimer’s Disease: Course, Prevention, Treatment Strategies 10 INTERVENTION Primary Prevention Secondary Prevention Treatment CLINICAL STATE Normal Pre- symptomatic AD Mild Cognitive Impairment AD Numbers of people ??? 20 to 60 mil 10 to 15 mil 5.3mil BRAIN PATHOLOGIC STATE No disease No symptoms Early AD brain changes No symptoms AD brain changes Mild symptoms Mild, moderate or severe impairment STRATEGIES Identify at-risk Prevent AD Prevent or delay emergence of symptoms Stimulate memory Slow progression Treat cognition Treat behaviors Slow progression DISEASE PROGRESSION

11
AD: Physician Perspective 11

12
Alzheimer’s, the Scope of the Problem Most significant Risk Factor Age Prevalence of Cognitive Impairment 50% of those >85 Co-morbidities At least one present in 95%

13
Easy Practice Tips

14
Practice Tips Red flags Repetition (not normal in 7-10 min conversation) Tangential, circumstantial responses Losing track of conversation Frequently deferring to family Over reliance on old information/memories Inattentive to appearance Unexplained weight loss or “failure to thrive”
 Tangential, circumstantial responses Losing track of conversation Frequently deferring to family Over reliance on old information/memories Inattentive to appearance Unexplained weight loss or failure to thrive")
15
Practice Tips Family observations: ANY instances whatsoever of getting lost while driving, trouble following a recipe, asking same question repeatedly, mistakes paying bills Ask: “Let’s suppose your family member was alone on a domestic flight across the country and the trip required a layover with a gate change. Would he/she be able to manage that kind of mental task on his/her own?”

16
Practice Tips Intact older adult should be able to: Describe 2 current events in some detail Describe what happened on 9/11, New Orleans disaster Name the current President and 2 immediate predecessors Describe medical history and names of some medications

17
Dementia Care Screening Diagnosis Management

19
Rationale for Early Detection 1. Improve quality of life Early treatment is more effective Stabilization vs. improvement Patients can make decisions regarding care Patients can get to their “bucket list” Decrease burden on family and caregivers 2. Connection to services that promote independent (supported) living as long as possible RTC support/counseling intervention (Mittelman et al. Neurology 2006) Non-pharm interventions reduce NH placement by 30% and delay placement for others by 18+ months
 living as long as possible RTC support/counseling intervention (Mittelman et al. Neurology 2006) Non-pharm interventions reduce NH placement by 30% and delay placement for others by 18+ months.")
20
Rationale for Early Detection 3. May find reversible causes NPH, TSH, B12, hypoglycemia, depression 4. Improve management of co-morbid conditions Underlying dementia = a primary risk factor of poor compliance in the elderly Chronic disease (diabetes, hypertension, anticoagulation) Integrity of the brain related to one’s ability to manage health Dementia as the Organizing Principle of Care
 Integrity of the brain related to one’s ability to manage health Dementia as the Organizing Principle of Care.")
21
Rationale for Early Detection 5. Reduce ineffective and expensive crisis-driven use of healthcare resources Unhelpful emergency room visits and hospitalizations Prevent diagnosis during crises (wandering, hospitalization, car accidents, bankruptcy) 6. More time to participate in clinical trials and important scientific studies Knowledge gap re: earlier stages Find a cure
 6. More time to participate in clinical trials and important scientific studies Knowledge gap re: earlier stages Find a cure.")
22
Screening Initial considerations Balance b/w time and sensitivity/specificity How will your practice incorporate screening? Who will administer tests? MDs, Nurses, social workers, allied health professionals What happens when screen is positive?

23
Annual Wellness Visit: Medicare Took effect January 1, 2011 Affordable Care Act Medicare will cover an annual wellness visit which will include the creation of a personalized prevention plan For first time, “detection of cognitive impairment” is core feature of the exam Diagnosis of dementia requires a decline in function over time, so screen provides a baseline on cognition

24
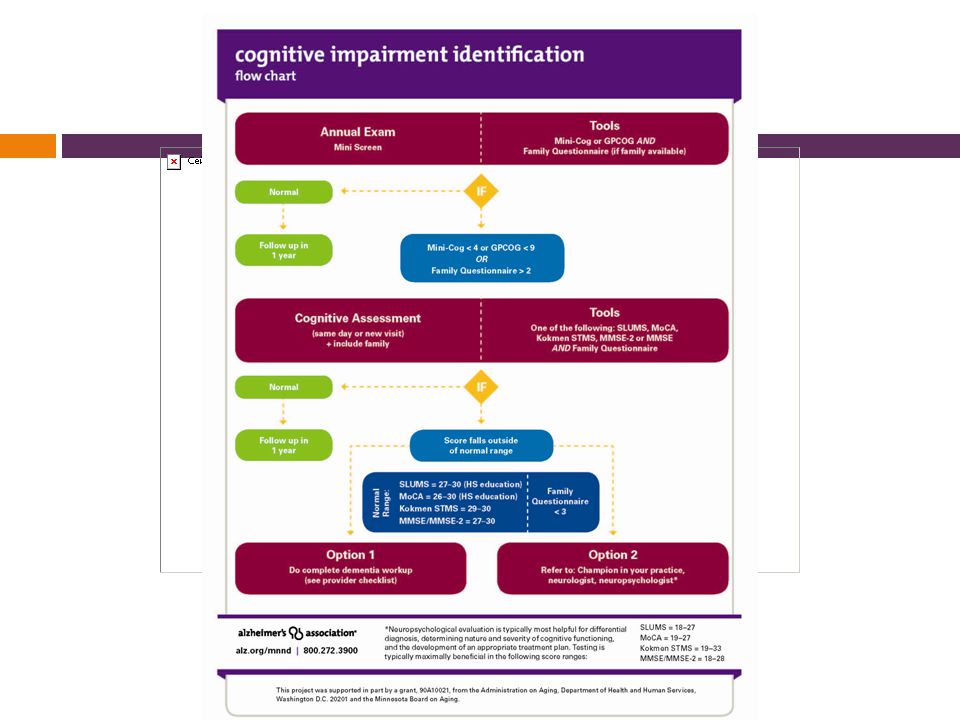
Screening Measures Wide range of options Mini-Cog (MC) Mini-Mental State Exam (MMSE) St. Louis University Mental Status Exam (SLUMS) Montreal Cognitive Assessment (MoCA) All but MMSE free online in public domain Utilize “Family Questionnaire (if family available)
 Montreal Cognitive Assessment (MoCA) All but MMSE free online in public domain Utilize Family Questionnaire (if family available).")
25
Mini-Cog Contents Verbal Recall (3 points) Clock Draw (2 points) Advantages Quick (2-3 min) Easy High yield (executive fx, memory, visuospatial) Subject asked to recall 3 words Leader, Season, Table Subject asked to draw clock, set hands to 10 past 11 +3 +2
 Clock Draw (2 points) Advantages Quick (2-3 min) Easy High yield (executive fx, memory, visuospatial) Subject asked to recall 3 words Leader, Season, Table Subject asked to draw clock, set hands to 10 past")
26
Mini-Cog Performance unaffected by education or language Borson Int J Geriatr Psychiatry 2000 Sensitivity and Specificity similar to MMSE (76% vs. 79%; 89% vs. 88%) Borson JAGS 2003 Does not disrupt workflow & increases rate of diagnosis in primary care Borson JGIM 2007 Failure associated with inability to fill pillbox Anderson et al Am Soc Consult Pharmacists 2008
 Borson JAGS 2003 Does not disrupt workflow & increases rate of diagnosis in primary care Borson JGIM 2007 Failure associated with inability to fill pillbox Anderson et al Am Soc Consult Pharmacists")
27
Mini-Cog Pros Easy to administer Minimal time commitment Clock sensitive to visuospatial & executive dysfunction Simple scoring and interpretation Cons Not as sensitive for MCI or early dementia when compared to longer screens Brevity means less information to interpret

29
Screen Failure MiniCog = <4 OR memory complaints by patient/family Schedule follow-up appt Insist on family collateral Perform more complex test (MOCA, SLUMS, MMSE)
")
30
MMSE

31
Pass > 26 Fail 25 or less

32
Pros Widely accepted and validated for dementia screening 30-point scale well known and score easily interpretable Measures orientation, working memory, recall, language, praxis Cons Scale developed 40 years ago, before MCI criteria and when early dementia less well understood Lacks sensitivity to MCI and early dementia Takes 7+ min. to administer Copyright issues MMSE

33
SLUMS

34
Pros More measures of executive functioning Good balance between easy and difficult items More sensitive than MMSE in detecting MCI and early dementia 30-point scale similar to MMSE Score range for MCI and dementia Free online Cons Takes 10 min. to administer Slightly more complex directions than MMSE Less name recognition than MMSE SLUMS

35
Pass > 26 Fail 25 or less

36
MoCA

37
Pass > 26 Fail 25 or less

38
Pros Much more sensitive than MMSE for MCI and early dementia More content tapping higher level executive fx 30-point scale similar to MMSE Translations available in 35+ languages Free online Cons Takes 10-14 min. to administer More complex administration and directions than MMSE MoCA

39
Screening Tool Selection Montreal Cognitive Assessment (MoCA) Sensitivity: 90% for MCI, 100% for dementia Specificity: 87% St. Louis University Mental Status (SLUMS) Sensitivity: 92% for MCI, 100% for dementia Specificity: 81% Mini-Mental Status Exam (MMSE) Sensitivity: 18% for MCI, 78% for dementia Specificity: 100% Larner et al Int Psychogeriatr 2012; Nasreddine et al J Am Geriatr Soc 2005; Tariq et al Am J Geriatr Psychiatry 2006; Ismail et al Int J Geriatr Psychiatry 2010
 Sensitivity: 92% for MCI, 100% for dementia Specificity: 81% Mini-Mental Status Exam (MMSE) Sensitivity: 18% for MCI, 78% for dementia Specificity: 100% Larner et al Int Psychogeriatr 2012; Nasreddine et al J Am Geriatr Soc 2005; Tariq et al Am J Geriatr Psychiatry 2006; Ismail et al Int J Geriatr Psychiatry")
40
Dementia Care Screening Diagnosis Management

42
Diagnostic Workup H&P Diagnostics Labs Imaging Neuropsychological assessment Diagnosis Family meeting

43
History & Physical History (with collateral) Onset, duration, course Examples of memory difficulties Impact on function $ management, meds, driving, cooking Mood, personality or behavior changes Drug or alcohol use Medication side effects Physical + brief neuro exam Do depression screening (PHQ-9), if not already completed
 Onset, duration, course Examples of memory difficulties Impact on function $ management, meds, driving, cooking Mood, personality or behavior changes Drug or alcohol use Medication side effects Physical + brief neuro exam Do depression screening (PHQ-9), if not already completed")
44
Diagnostics: Labs Routine Labs CBC Electrolytes BUN/creatinine Glucose Calcium LFTs--?? Dementia screening Vitamin B12, folate TSH Contingent labs RPR or MHA-TP HIV Heavy metals

45
Diagnostics: Imaging CT adequate for pts with clinical history consistent with AD MRI helpful for determining pattern of focal atrophy Request radiologist comment on hippocampal volume Scans often unremarkable in patients with early AD Rule out focal lesions, trauma, ischemia, NPH No need to repeat if pt. had recent scan Within 12 months No recent hx of trauma

46
Diagnostics: Neuropsych Testing Helpful in distinguishing normal aging from MCI and dementia Atypical presentations Rule out: Pseudodementia, substance abuse factors, etc. Determine type of dementia, stage, capacity, most appropriate level of support Consider particularly when: MoCA 19-27 SLUMS 18-27 MMSE 18-28

48
Loss of Memory Plus one of the following Impairment in handling complex tasks (balancing a check book, calendars, clock drawing) Impairment in reasoning ability Impaired spatial ability and orientation (lost) Impaired language (word finding) Severe enough to impact daily life and is a decline from previous function Dementia Diagnosis
 Impairment in reasoning ability Impaired spatial ability and orientation (lost) Impaired language (word finding) Severe enough to impact daily life and is a decline from previous function Dementia Diagnosis")
49
Diagnosis Alzheimer’s disease: 60-80 % Includes mixed AD + VD Lewy Body Dementia: 10-25 % Parkinson spectrum Vascular Dementia: 6-10 % Stroke related Frontotemporal Dementia: 2-5 % Personality or language problems

50
Vascular Dementia Clinical Features Focal neurological signs Stepwise progression Often overlaps with AD (6-10% dementia related to pure VD) Neuropsychological Testing Predominant deficits in executive function, attention, and processing speed Neuroimaging Cerebrovascular Disease Large vessel stroke Periventricular/subcortical white matter disease
 Neuropsychological Testing Predominant deficits in executive function, attention, and processing speed Neuroimaging Cerebrovascular Disease Large vessel stroke Periventricular/subcortical white matter disease")
51
Dementia with Lewy Bodies Clinical Features Parkinsonism, hallucinations, cognitive fluctuations, REM behavioral sleep disorder Neuropsychological Testing Predominant visuospatial dysfunction with relative sparing of verbal memory Neuroimaging Non-specific MRI atrophy pattern Occipital hypometabolism on FDG-PET

52
Frontotemporal Dementia Clinical Features Typical onset prior to age 65 Behavioral symptoms Disinhibition, apathy, loss of empathy, repetitive stereotyped movements, hyperorality Language symptoms Expressive aphasia, anomia, surface dyslexia Neuropsychological Testing Impairments on executive function/language with relative sparing of episodic memory and visuospatial function Neuroimaging Atrophy of frontal and anterior temporal cortex

53
Dementia Care Screening Diagnosis Management

55
Overall Management Goals; Reduce suffering that accompanies the disease Reduce the negative impacts that dementia has on both health & quality of life Balancing independence & safety Optimize the management of co-morbid conditions Weighing benefits, burdens & risks of treatments Care Plan for acute illness Supporting the Caregiver

56
Management Medication treatment Small component of care plan Education Increase family’s dementia competence Support / Referral Connect to community resources

57
AD: Care Coordination 57

58
Intervention Model - Clinic Patient Care Partners Care Coordinator Physician / Clinic

59
Care Coordination Identify cognitive impairment, facilitate diagnosis Identify ‘team members’, including care partner Conduct needs assessment Develop & initiate care plan Communicate with team Monitor & re-evaluate Termination 59

60
Clinic Care Coordination Needs Care partner / team approach Disease education Assistance with medication management Written materials / plans POA / healthcare directive Appointment reminders Driving assessment / transportation options Occupational therapy / home safety assessment, fall risk Risk reduction strategies Connection to community resources & programs 60

61
Risk Reduction Genetic Factors: APP, Presinilin 1 &2 / APOE4 Environmental Factors: begins in mid-life (50%) Mid-life HTN & Obesity (60%) Physical Inactivity (40 – 80%) Mid-life Depression (40 – 80%) Low Education / Cognitive Reserve (60 – 80%) Smoking (60%) Alcohol – Late Life & Binge Drinking (2xmo) Sleep Hygiene : quality & quantity
 Mid-life HTN & Obesity (60%) Physical Inactivity (40 – 80%) Mid-life Depression (40 – 80%) Low Education / Cognitive Reserve (60 – 80%) Smoking (60%) Alcohol – Late Life & Binge Drinking (2xmo) Sleep Hygiene : quality & quantity")
62
62 Mild Cognitive Impairment (MCI) Current Services in Minnesota Medical Evaluation / Diagnosis / Pharmacological Treatment* Research / Clinical Trials* Care Coaching / Consultation / Counseling* Information / Education* MCI Support Groups* Engagement Programs (arts, social, creativity)* Exercise / Nutrition / Cognitive Habilitation* * limited availability
 Current Services in Minnesota Medical Evaluation / Diagnosis / Pharmacological Treatment* Research / Clinical Trials* Care Coaching / Consultation / Counseling* Information / Education* MCI Support Groups* Engagement Programs (arts, social, creativity)* Exercise / Nutrition / Cognitive Habilitation* * limited availability")
63
63 Early Stage Current Services in Minnesota Medical Evaluation / Diagnosis / Pharmacological Treatment* Research / Clinical Trials* Care Coaching / Consultation Information / Education / Driving Evaluation* Early Stage Support Groups* Engagement Programs (arts, social, creativity)* Exercise / Nutrition / Cognitive Habilitation* Home Care / Companion Services* Assisted Living Medic Alert Safe Return ® * limited availability
* Exercise / Nutrition / Cognitive Habilitation* Home Care / Companion Services* Assisted Living Medic Alert Safe Return ® * limited availability")
65
65

66
66 Middle Stage Current Services in Minnesota Medical Evaluation / Diagnosis / Pharmacological Treatment Research / Clinical Trials* Care Coaching / Consultation / Counseling Information / Education / Driving Evaluation* Caregiver Support Groups* Adult Day Services* Meals on Wheels* Home Care / Home Health Care / Respite Services* Medic Alert Safe Return ® Assisted Living / Nursing Facility * limited availability

67
67 Late Stage Current Services in Minnesota Medical Evaluation / Diagnosis / Pharmacological Treatment Care Coaching / Consultation / Counseling Information / Education Caregiver Support Groups* Adult Day Services* Meals on Wheels* Home Care / Home Health Care / Respite Services* Medic Alert Safe Return ® Assisted Living / Nursing Facility Hospice* * limited availability

68
68 Research Minnesota Resources Alzheimer’s Disease Research Center – Mayo Clinic University of Minnesota VA Medical Center Alzheimer’s Research Center, Regions Hospital Health Partners Research Fund Healthcare Interactive (HCI) TrialMatch: http://www.alz.org/research/clinical_trials/find_clinical_tria ls_trialmatch.asp
 TrialMatch: ls_trialmatch.asp")
69
69 ACL Projects Minnesota Resources Family Memory Care: evidence-based consultation Systems Integration: dementia capability Telephone / Internet Resources Alzheimer’s Association 1-800-272-3900 alz.org Senior LinkAge Line® 1-800-333-2433 MinnesotaHelp.info®

70
AD: The Patient Experience 70

71
Conclusion / Q&A 71

Similar presentations











 Training Program>")


: The Role of Cognitive Assessment in Improving Health Outcomes Dr. William Mansbach October 25, 2011.>")









